EBSTEINS ANOMALY First described by Wilhelm Ebstein in

EBSTEIN’S ANOMALY • First described by Wilhelm Ebstein in 1866 ; terminology coined by Alfred Arnstein • 19 yr old cyanotic laborer with CHF • at autopsy Ebstein found an enlarged and fenestrated ATL; STL & PTL were thickened, hypoplastic and adherent to RV. thin , dilated atrialised RV ; enlarged RA ; PFO

EBSTEIN’S ANOMALY < 1 % of CHD 1 per 200, 000 live births No gender preferance Most are sporadic ; familial pattern is rare ? Genetic / reproductive / environmental risk factors • more common in twins • maternal exposure to benzodiazepines / lithium

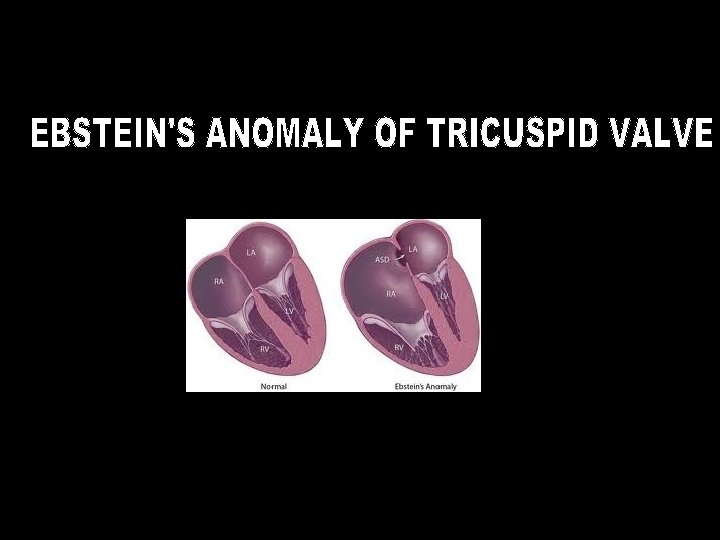
EBSTEIN’S ANOMALY Pathology malformation of the tricuspid valve and right ventricle characterized by * adherence of the septal and posterior leaflets to the underlying myocardium (failure of delamination, namely splitting of the tissue by detachment of the inner layer during embryologic development); * downward (apical) displacement of the functional annulus (septal>posterior>anterior); * dilation of the “atrialized” portion of the right ventricle, with various degrees of hypertrophy and thinning of the wall; * redundancy, fenestrations, and tethering of the anterior leaflet *dilation of the right atrioventricular junction (true tricuspid annulus)

Ebsteins Normal

EBSTEIN’S ANOMALY Pathology atrialised trabecular Right ventricle functional outlet In two third cases RV gets dilated – atrialised part RVapex RVOT

EBSTEIN’S ANOMALY Associated defects interatrial communication in 80 - 94 % rarely • bicuspid AV , subaortic stenosis, coarct , VSD, MVP • PS , pulmonary atresia , hypoplastic pulm. arteries Analysis of 106 cases by Jost et al (Circ. 2007) Left sided anomalies in 39 % 18% of these had LV hypoplasia mimicking LV noncompaction 15 – 50 % of l – TGA has Ebstein’s like malformation of left AV valve AV bypass tracts in 20 - 30 %

EBSTEIN’S ANOMALY Classification Carpentier et al 1988 Type A - - adequate RV volume Type B - - large atrialised RV ; mobile ATL Type C - - restricted mobility of ATL > RVOT obstruction Type D - - near complete atrialisation of RV

EBSTEIN’S ANOMALY Physiology Variable – depends on the degree of pathology RV dysfunction Retards forward flow Tricuspid regurgitation During atrial systole atrialised RV balloons out acting as a passive reservoir ; during ventricular systole, much of this blood is propelled back to RA High RA pressure & low LA pressure leads to R > L shunt at atrial level

EBSTEIN’S ANOMALY Physiology Neonatal period High PVR + RV dysfunction -- behaves like pulm. atresia R > L shunt at atrial level ; ductus dependent Few weeks to months PVR falls > improvement in RV function > fall in RA pressure > cyanosis disappears Adolescence / adulthood RV failure > high RA pr. -- R > L interatrial shunt > cyanosis In patients with intact IAS. . No cyanosis; but severe CHF

EBSTEIN’S ANOMALY Clinical features Depends on the severity of malformaton Asymptomatic to severely symptomatic Cyanosis , dyspnea , palpitation , s/o CHF Cyanosis. . Typical triphasic Pulse. . Low volume ; arrhrythmias JVP. . Unimpressive Elevated ; A + / V+ Precordium. . Relatively quite despite cardiomegaly RVOT pulsation+

EBSTEIN’S ANOMALY Clinical features Auscultation Cadence of sounds • split S 1 ; loud T 1 ( sail sound ) • split S 2 ; soft P 2 • RV S 3 , S 4 • tricuspid OS Murmurs • TR murmur • tricuspid MDM mimics percardial rub
")
EBSTEIN’S ANOMALY ECG RA dilatation > tall P waves -- Himalayan P ( Taussig) Marked RA dilatation > widening & notching of P. indicates poor prognosis Right sided pre excitation in 20 – 30 % ( LAD of delta & QRS ) Without WPW RBBB pattern QRS axis. . rightward ; rarely normal / leftward polyphasic QRS in precordial leads RVH pattern. . Unusual Arrhythmias – due to RA dilatation / WPW SVT / A flutter / A fib Ventricular arhhythmias / AV blocks. . Less common

EBSTEIN’S ANOMALY

EBSTEIN’S ANOMALY Xray

EBSTEIN’S ANOMALY Echocardiogram Mmode Parasternal view. . Simultaneous visuslistion of mitral & tricuspid echoes Measure the delay from mitral to tricuspid clousre normal – 20 – 40 ms > 60 ms. . in favour of Ebsteins 2 D detailed evaluation of the tricuspid valve apparatus Apical displcement of septal leaflet chambers associated lesions RV function R > L shunt at atrial level

EBSTEIN’S ANOMALY TV closure MV closure RVdilatation ; Paradoxical septal motion

EBSTEIN’S ANOMALY Echocardiogram Apical displacement of STL Normal. . AML to STL distance is upto 8 mm / sq. m BSA. Ø 15 mm / sq. m in children < 14 yrs Ø 20 mm /sq. m in adults Diagnostic of Ebstein’s Grading score. . Celemajor et al The ratio of the combined area of the right atrium and atrialized right ventricle is compared with that of the functional right ventricle and left heart ratio <0. 5 ratio of 0. 5 to 0. 99 ratio of 1. 0 to 1. 49 ratio ≥ 1. 5 grade 1 grade 2 grade 3 grade 4

EBSTEIN’S ANOMALY

EBSTEIN’S ANOMALY CMR

EBSTEIN’S ANOMALY Cardaic cath Not really needed now Mainly for EPS / RFA Angiographic data can be obtained by CMR Hemodynamics Low PA and RV pressure High RA pressure Systemic desaturation Atrialised RV … RA pressure morphology with RV electrogram

EBSTEIN’S ANOMALY Management • Asymptomatic --- follow up • Newborn with cyanosis. . Maintain PDA with PGE 1 • Symptomatic CHF. . Medical - digoxin , diuretics Surgery Arrhythmia. . Antiarrhtyhmics EPS > RFA Pacing for AV block ( 4 %) Cyanosis without significant TR ? Role of device closure of ASD

EBSTEIN’S ANOMALY Surgery 1959 1962 1974 Repair of TV in 2 pts – both died First successful surgery. . TV replacement Initial publication on TVR. . 54 % mortality Indications • NYHA III – IV • NYHA I – II + CT ratio > 0. 65 • significant cyanosis • paradoxical embolism • resistant tachyarrhythmias Methods • Tricuspid valve replacement • Tricuspid valve repair. . Different techniques • one and a half ventricular repair • Heart transplant

EBSTEIN’S ANOMALY Surgery Mayo clinic series 1972 – 2005 ; 540 pts Valve reconstruction – Valve replacement - in 35 %. . Early death – 5. 4 % in 65 %. . Early death - 7. 6 % Technique • construction of a monocuspid valve using ATL • plication of free wall of atrialised RV • posterior tricuspid annuloplasty • reduction right atrioplasty

EBSTEIN’S ANOMALY Surgery 1988 – Carpentier et al • longitudinal plication of atrialised RV and adjacent RA • mobilisation of ATL and adjacent PTL and repositioning to cover the orificearea at normal level • remodeling and reinforcement of annulus by prosthetic ring 191 cases early mortality 9% mean late 20 yr survival 80%

EBSTEIN’S ANOMALY Surgery One and a half ventricular repair • tricuspid valve repair • reduction of atrialised RV • closure of ASD • end to side anastamosis of SVC to RPA
 220 cases from 1958")
EBSTEIN’S ANOMALY Natural history Celemajor et al (JACC 1994 ) 220 cases from 1958 to 1991 ; FU 1 – 34 yrs Actuarial survival 67 % at 1 yr ; 59 % at 10 yrs Predictors of death • echo grade – 2. 7 fold increase in risk for each grade increase • fetal presentation • RVOT obstruction

- Slides: 29