Early Pregnancy Problems Introduction Bleeding in early pregnancy


Early Pregnancy Problems

Introduction Bleeding in early pregnancy and miscarriage Ectopic Pregnancy Gestational Trophoblastic Disease Hyperemesis Gravidarum

Bleeding in Early Pregnancy & Miscarriage

Definitions Remember – MISCARRIAGE not ABORTION Threatened miscarriage Vaginal bleeding at < 20 weeks gestation (cervix closed) Inevitable miscarriage Bleeding, pregnancy still in uterus (cervix open) Incomplete miscarriage Retained products of conception in uterus (cervix open) Complete miscarriage Uterus empty (cervix closed) Delayed miscarriage Gestational sac with/without fetus present (but no FH), cervix closed

Miscarriage Approximately 30% of pregnant women will experience bleeding in early pregnancy At least 50% of women with threatened miscarriage will have continuing pregnancy Miscarriage occurs in 15 -20% of clinically diagnosed pregnancies

Causes of miscarriage Genetic abnormalities Progesterone deficiency? Maternal illness e. g. diabetes Uterine abnormalities ‘Cervical incompetence’
, clots Pain: type – crampy/sharp/dull location: lower abdomen, shoulder")
History LMP Bleeding: amount (spotting/gush), clots Pain: type – crampy/sharp/dull location: lower abdomen, shoulder tip, back pain Passed products?
 stable or cervical shock Abdominal tender/ rebound tenderness Vaginal (speculum)")
Examination ABC (vital signs) stable or cervical shock Abdominal tender/ rebound tenderness Vaginal (speculum) Cervix: open/closed Amount of bleeding Products visible? . . . TAKE IT OUT!

Speculums Cusco speculum Sims speculum

Investigations Ideally in dedicated ‘Early Pregnancy Assessment Unit’ Ultrasound Measurement of serum βh. CG Determination of blood & Rhesus group admit if significant bleeding Psychological support

Ultrasound Expect to see viable fetus from around 6. 5 weeks transabdominally, 5. 5 weeks transvaginally Other possible appearances Incomplete miscarriage Empty uterus Not pregnant Too early gestation Extrauterine pregnancy Complete miscarriage Empty sac Non-viable pregnancy Too early gestation Fetal pole with no FH gestation If tiny, may be very early Delayed miscarriage

Gestational sac

Very early. .

Normal 8 -9 wk pregnancy

Empty sac

Measurement of βh. CG Not necessary if diagnosis unequivocal on scan Useful as part of investigations to diagnose/exclude extrauterine pregnancy/miscarriage Doubling time approx 2 days in viable pregnancy Halving time 1 -2 days in complete miscarriage Should see fetal pole with βh. CG of 1500 -2000

Management of Incomplete Miscarriage Conservative Risk of bleeding, infection, retained POC, unpredictable Medical (Prostaglandin e. g. Misoprostol) Risk of bleeding, retained POC, need for D&C Surgical [Evacuation of retained products of conception (ERPC)] Suction curettage usually under GA, risk of bleeding, infection, perforation of uterus, longer term complications (e. g. Ashermans syndrome)

Ectopic Pregnancy

Definition Pregnancy occurring outside uterine cavity Approx 0. 5 -1% of pregnancies – rate increasing Maternal mortality in 1/2500 ectopic pregnancies (13 deaths 1997 -1999 in UK)

Site Fallopian tube Ovary Abdominal cavity Cervix
")
Risk factors Previous PID Previous ectopic pregnancy Previous tubal surgery (e. g. sterilisation, reversal) Pregnancy in the presence of IUD

Symptoms Acute Low abdominal pain – peritoneal irritation by blood Vaginal bleeding – shedding of decidua Shoulder tip pain – referred from diaphragm Fainting - hypovolaemia Chronic (Atypical) Asymptomatic, gastrointestinal symptoms, back pain

Signs Shock – tachycardia, hypotension, pallor Abdominal tenderness Adnexal mass None

Diagnosis Ultrasound Serum βh. CG Empty uterus, adnexal mass, free fluid in Abdomen, rarely live pregnancy outside of uterus Suboptimal rise, plateau Laparoscopy

Ultrasound

Left Ectopic on laparoscopy

Management Medical Surgical Methotrexate Laparoscopic salpingectomy / salpingotomy Laparotomy ‘Conservative’ Self resolving with close watch

Gestational Trophoblastic Disease

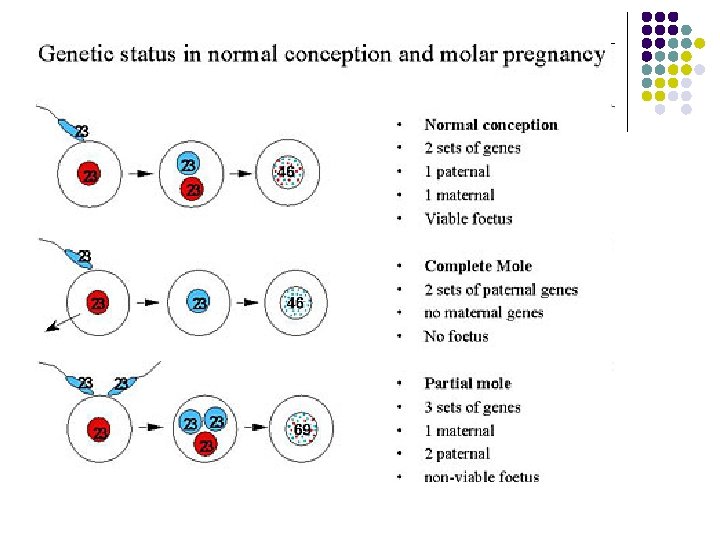
Hydatidiform Mole 1 in 1000 pregnancies Partial Associated with fetus, triploid Complete No fetal pole, diploid chromosomes paternally derived

Presentation Asymptomatic – incidental finding at dating or anomaly USS Vaginal bleeding Hyperemesis gravidarum Uterus large for dates
 Histology after surgical evacuation")
Diagnosis Ultrasound (Snow storm appearance) Histology after surgical evacuation

Snowstorm appearance

Hydatidiform Mole after hysterectomy

Follow-up Monitor via regional centre 3% risk choriocarcinoma following complete mole, less following partial mole Choriocarcinoma may follow any subsequent pregnancy – miscarriage, TOP, term delivery Choriocarcinoma is curable Monitor βh. CG levels to check resolution – for 6 months to 2 years Avoid pregnancy for minimum 6 months or until all clear

Hyperemesis Gravidarum

Hyperemesis Gravidarum Nausea/vomiting in pregnancy is normal – ‘morning sickness’ Rarely excessive – hyperemesis gravidarum Related to level of βh. CG

Associated Factors UTI Multiple pregnancy Molar pregnancy Socio-economic factors

Investigations Renal function Liver function CBC Urinalysis Ultrasound

Consequences & Dehydration Management Electrolyte imbalance Metabolic alkalosis, hypokalaemia, hypernatremia IV fluids Electrolyte replacement Antiemetics Thromboprophylaxis Dietary advice Vitamin supplementation Steroids Oesophageal tears (Mallory Weiss) Thrombosis DVT/PE/Cerebral sinus Weight loss Vitamin deficiency (vit B 1 - thiamine) Wernicke's encephalopathy Psychological impact Antibiotics if UTI Termination of pregnancy

in CONCLUSION GYNAECOLOGICAL EMERGENCIES 1. MISCARRIAGE 2. ECTOPIC 3. PELVIC SEPSIS 4. OVARIAN TORSION

Thank you for your attention
- Slides: 43