Early Mobilization After Stroke JERED NELSON Defining Early

Early Mobilization After Stroke JERED NELSON

Defining Early 1 Mobilization The term is problematic because there is no clear definition of early mobilization in current research not enough volume of research to generalize the data to specific subgroups of stroke patients Hours? Days? Weeks? Types of movement: limbs in bed, sitting, out of bed, walking?

Evidence In Recent Despite limited evidence guidelines for post-stroke rehabilitation have shifted to include early mobilization 30 acute stoke guidelines worldwide with recommendations on early mobilization: 22 recommended to mobilize early Only 8 defined the intervention 13/22 guidelines used a primary justification of preventing complications not promoting recovery 1 Years

Potential 1 Benefits : Primary rationale is to prevent or reduce immobility related complications (infections, DVTs, falls) What we do know: Organized stroke units experienced fewer immobility-related complications faster mobilization and rehabilitation Stroke Unit Facts: Median mobilization time 18 hrs 30% of day time in bed, 46% out of bed, 20% standing and walking Brain recovery: Critical sensitive period of enhanced neuroplasticity after early stroke Areas ipsilesional and contralesional are hyperexcitable long term potential is enhanced

Stroke Units and Quality Review of RCTs comparing stroke unit outcomes to general wards 5 Pts more likely to be alive, independent and living alone w/i 1 year if care given in stroke unit ↓’d odds of death or institutionalization Did not increase LOS Potential unique characteristics of stroke units (as compared to general wards) Teamwork, staff education, functional training, and integrated care Shorter time to start of the systematic mobilization/training ↑’d use of oxygen, heparin, intravenous saline solutions, and antipyretics Less variation in diastolic and systolic blood pressure (BP), avoiding the lowest diastolic BP, and lowering temperature Indredavik et al. , 1999; Stroke Unit Trialists’ Collaboration, 2013

Potential 1 Harm : Concerns for upright position early inhibiting restoration of blood flow to salvageable penumbral tissue. Increased blood pressure associated with activity my worsen outcomes Concerns for starting early mobilization in pts with hemorrhagic stroke for risk of further bleeding Out of bed activities could result in more falls with injury

A Closer Look At Recent Evidence

Early Mobilization After 2 Stroke AVERT: A Very Early Rehabilitation Trial After multiple pilot studies conducted in various countries showed beneficial results for early mobilization (within 24 hrs), a large scale experiment was conducted to gain a greater insight Clinical hypothesis: More intensive, early out-of-bed activity would improve functional outcome at 3 months, reduce immobility-related complications and accelerate walking recovery with no increase in neurological complications

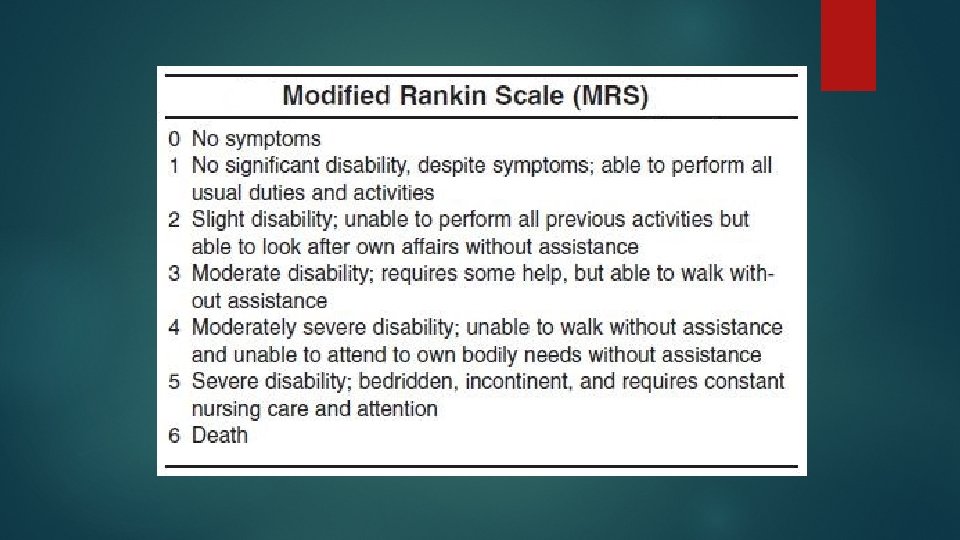
2 Methods Randomized control, single-blinded, international, pragmatic study with data collected from 56 stroke units across 5 counties Inclusion criteria: >18 yo Confirmed 1 st or recurrent stroke (infarct or cerebral hemorrhage) Admitted within 24 hrs of stroke onset Exclusion criteria: Significant pre-morbid disability (>2 on modified Rankin Scale) No response to voice Systolic BP <110 mm. Hg or >220 mm. Hg O 2 <92% with supplementation Resting HR <40 bpm or >110 bpm Subarachnoid hemorrhage
 Begin within 24 hrs")
Methods 2 Cont. Interventions for VEM group (3 crucial elements) Begin within 24 hrs of stroke onset Focus on sitting, standing, and walking activity Result in at least 3 additional out-of-bed sessions to usual care Outcome measure Favorable outcome at 3 months was defined by a score of 0 -2 on the modified Rankin Scale

Intervention 2 Summary

Outcomes at 3 2 Months

Statistics of 2 Study Data collected between 2006 -2014 2104 patients assigned to VEM (1054) or usual care (1050) 1 st time stoke for 80% of patients 45% of patients classified as having moderate/severe (NIHSS>7) 26% of patients were older than 80 The median time to mobilization was 18. 5 hrs in the VEM group while the usual care group was almost 5 hrs later

Conclusions Drawn After data was adjusted for baseline age and NIHSS, results showed a statistical significance between patient outcomes in VEM and usual care The VEM intervention significantly reduced the odds of a favorable outcome 3 months after a stroke compared with lower dose usual care starting, on average, 5 hrs later.

Limitations of Study and Next 2 Step Unable to account for patient-staff interaction Not having a set mobilization protocol for usual care practices 60% of patients receiving usual care had started out-of-bed therapy within 24 hrs of stroke onset The next priority in stroke research is to look at dose-response to establish the effect of dose of rehabilitation on efficacy and safety

Strok. EDGE: Exams for Acute Care http: //www. neuropt. org/docs/edge-documents/strokedge_acute_care_recs. pdf? sfvrsn=2 Accessed 3 -7 -17

Intervention: Acute Hospital 3 Discharge planning Prognostic indicators: initial NIHSS score, size of lesion, movement in arm within few days, ambulatory day 2, dysphagia, continence, improvement over first few days Attempt to minimize 2° impairments, pathologies Educate and prevent falls **do NOT do intense PT early (w/I 24 hours) as of now

Acute Hospital: General Recs • Early rehab • Intensity? • NOT early (w/i 24 hours) and intense rehab Winstein et al. , 2016

References 1. Bernhardt J, English C, Johnson L, Cumming TB. Early mobilization after stroke: early adoption but limited evidence. Stroke. 2015; 46(4): 1141– 6. doi: 10. 1161/STROKEAHA. 114. 007434. 2. Efficacy and safety of very early mobilization within 24 h of stroke onset (AVERT): a randomized controlled trial. The Lancet , Volume 386 , Issue 9988 , 46 – 55 3. Indredavik B, et al. Treatment in a combined acute and rehabilitation stroke unit: which aspects are most important? Stroke. 1999; 30: 917– 923. 9.
- Slides: 20