Each year more than eleven million children die










")



 • merozoites produced")




 • fusion of micro- and macrogametes")


. Studies in Africa have shown that ITNs")
 take weekly The most commonly reported minor side effects include nausea,")


 Sickle Cell- single point mutation- abnormal shape")




- Slides: 36
Each year, more than eleven million children die from the effects of disease and inadequate nutrition. In some countries, more than one in five children die before they reach their fifth birthday, and many of those who do survive are unable to grow and develop to their full potential. Seven out of 10 of childhood deaths in developing countries can be attributed to just five main causes, or often to a combination of them: pneumonia, diarrhea, measles, malaria and malnutrition. Around the world, three out of every four children seen by health services are suffering from at least one of these conditions.
Infectious diseases are the leading killer of young people in developing countries: These deaths occur primarily among the poorest people because they do not have access to the drugs and commodities necessary for prevention or cure. Approximately half of infectious disease mortality can be attributed to just three diseases – HIV/AIDS, TB and malaria. These three diseases cause over 500 million illnesses and more than 5 million deaths each year. None of these diseases has an effective vaccine to prevent infection in children and adults. Africa's GDP would be up to $100 billion greater if malaria had been eliminated years ago.
Malaria - TB - HIV/AIDS Many low income countries have shown that, by using available tools both widely and wisely, TB deaths can be reduced five-fold, HIV infection rates can also be reduced by 80% and malaria death rates can be halved. But, when a country has a healthcare budget of less than, for example, $50 per capita, the costs of the tools needed to fight TB, malaria and HIV are prohibitive. Many of the world's poor people live in countries with very low budgets for health care.
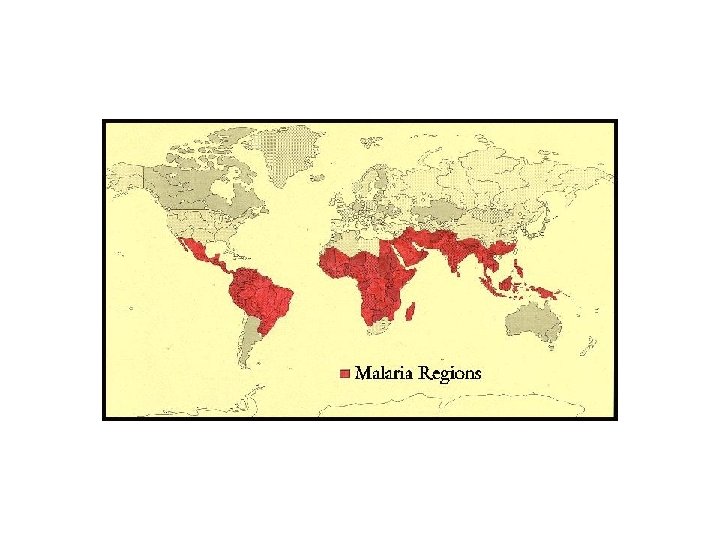
MALARIA * Cosmopolitan disease in tropical and sub tropical regions of the world * Most important vector-borne disease * Romans called it “mala aria”- disease emanating from the swamps * Caused decline in the Roman empire? * Caused problems in finishing the Panama Canal- Gorgas * The causal agent only identified in 1897 * Malaria symptoms and use of insect repellents recorded in Ebers papyrus (~ 3000 bc) * Was malaria present in the Americas before the arrival of Columbus?
MALARIA 40% of the world population is at risk for contracting malaria. It occurs in over 90 countries. 500 million new cases and 2 -3 million deaths annually. Most deaths occur among young children in tropical Africa who are infected with Plasmodium falciparum. Problems with vector resistance to insecticides, Plasmodium resistance to drugs, no vaccine have made malaria an excellent example of a reemerging infectious disease. How many is 3 million people?
Malaria Cases Number of deaths / year Deaths/day # Jumbo Jets day 3, 000 8, 200 20 2, 000 5, 500 14 A few years ago about 250, 000 people died in the S. Asian tsunami. The equivalent number occurs approximately every 30 -50 days for malaria alone- or every 10 -21 days for a combination of malaria, TB, and HIV/AIDS.
Symptoms of malaria include fever and flu-like illness, including shaking chills, headache, muscle aches, and tiredness. Nausea, vomiting, and diarrhea may also occur. Malaria may cause anemia and jaundice (yellow coloring of the skin and eyes) because of the loss of red blood cells. Infection with one type of malaria, P. falciparum, if not promptly treated, may cause kidney failure, seizures, mental confusion, coma, and death. For most people, symptoms begin 10 days to 4 weeks after infection, although a person may feel ill as early as 8 days or up to 1 year later. Two kinds of malaria, P. vivax and P. ovale, can create problems later: some parasites can rest in the liver for several months to 40 years after a person is bitten by an infected mosquito, and can cause disease.
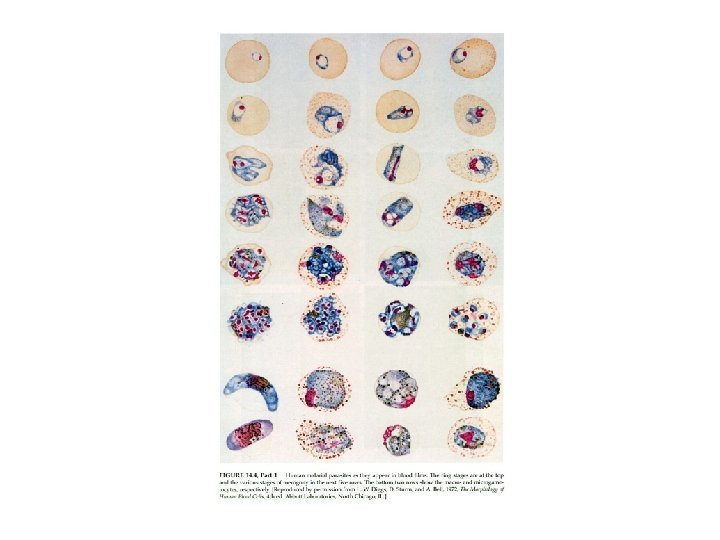
Human malaria There are four species of the genus Plasmodium that commonly infect man, P. falciparum, P. vivax, P. malariae and P. ovale. The most important of these is P. falciparum because it can be rapidly fatal and is responsible for the majority of malaria related deaths. Plasmodium vivax benign tertian malaria, vivax malaria Plasmodium falciparum malignant tertian malaria, falciparum malaria Plasmodium ovale tertian malaria, ovale malaria Plasmodium malariae quartan malaria, malariae malaria
Human malaria vector: Anopheles sp. Anopheles gambiae Anopheles albimanus Anopheles nunez tovari Anopheles stephensi Anopheles pseudopunctipennis Anopheles arabiensis
A merozoite, showing the apical prominence with a rhoptry, dense granules, and a very indented nucleus.
Section of liver showing a greatly enlarged parenchymal cell full of merozoites (see arrow) Section of brain showing blood vessels blocked with developing P. falciparum parasites (see arrows).
Important differences: P. vivax can maintain a liver infection, P. falciparum does not P. falciparum has a single exoerythrocytic cycle 1) Relapse: reactivation after a relative inactive period 2) Recrudescence: reappearance of parasitemia after therapy P. vivax has hypnozoites- dormant stages in the liver cells- reactivated later in life.
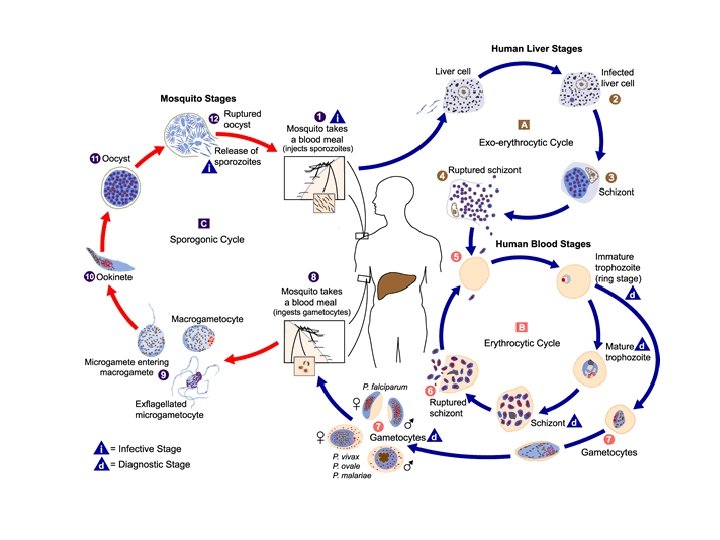
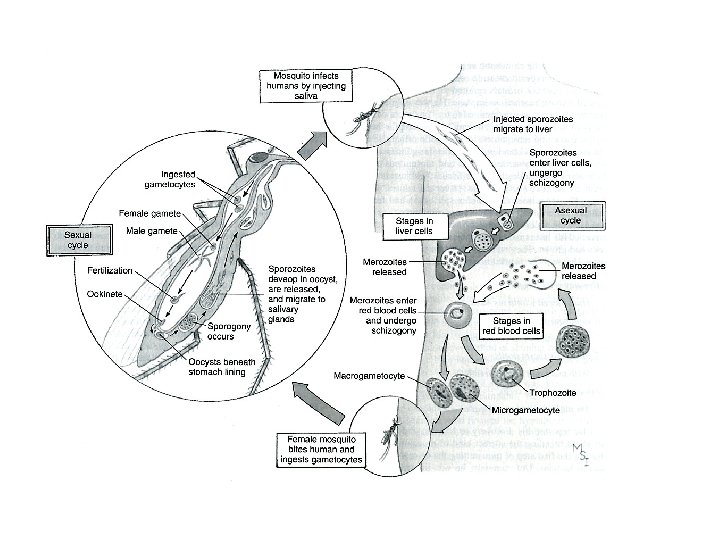
Transmission • sporozoites injected with saliva • enter circulation • trapped by liver Anopheles
Exoerythrocytic Schizogony • • • hepatocyte invasion asexual replication 6 -15 days 1000 -10, 000 merozoites no overt pathology
Hyponozoite Forms • some EE forms exhibit delayed replication (ie, dormant) • merozoites produced weeks-tomonths after initial infection • only P. vivax and P. ovale relapse = hypnozoite recrudescence = subpatentt
Erythrocytic Schizogony • intracellular parasite undergoes trophic phase • young trophozoite called ‘ring form’ • ingests host hemoglobin • cytostome • food vacuole • hemozoin (malarial pigment)
erythrocytic schizogony • 48 hr in Pf, Pv, Po • 72 hr in Pm gametocytes
Gametocytogenesis • alternative to asexual replication • induction factors not known • drug treatment #'s • immune response #'s • ring gametocyte • sexual dimorphism • microgametocytes • macrogametocytes • no pathology • infective stage for mosquito
• occurs in mosquito gut • ‘exflagellation’ most obvious • exposure to air induces • temperature (2 -3 o. C) • p. H (8 -8. 3) • gametoctye activating factor in mosquito • xanthurenic acid
Sporogony • occurs in mosquito (9 -21 d) • fusion of micro- and macrogametes • zygote ookinete (~24 hr) • ookinete transverses gut
OF THE 1 -3 MILLION or more deaths from malaria that occur worldwide each year, most are in African children under the age of five. Children in Africa south of the Sahara are vulnerable to malaria from about four months of age. In areas of intense transmission, young children may have as many as six episodes of malaria each year. Of the more than 500, 000 African children who develop cerebral malaria (a severe form of the disease that affects the brain) each year, 10 -20% die and approximately 7% are left with permanent neurological damage. Fever, vomiting, headache and flu-like symptoms may progress rapidly (often within 24 hours) to convulsions, coma, and death. Malaria is a major cause of anaemia in many parts of the world. Chronic anaemia may adversely affect a child’s growth and intellectual development. Repeated episodes of malaria may lead to severe, life-threatening anaemia. Blood transfusions may save lives in these circumstances, but also expose the child to the risk of HIV and other blood-borne infections.
Preventative Measures Prevent Insect Bites Wear long sleeved shirts and long pants in the evening. Use insect repellents Select hotels/housing with nets- preferably pemethrin-impregnated bednets Take effective drugs Reduce mosquito habitat Use residual insecticides (DDT? ? )
Prevention: Sleep under insecticide-treated nets (ITNs). Studies in Africa have shown that ITNs can reduce deaths among under-fives by up to one-third. There is an urgent need to ensure that effective and affordable antimalarial drugs or drug combinations are widely available to all individuals living in malariaendemic areas. Since, in Africa, many people first go to their local store for antimalarial drugs, shopkeepers are now being trained to supply the appropriate dose and duration of treatment.
DRUGS Mefloquine: (Lariam®) take weekly The most commonly reported minor side effects include nausea, dizziness, difficulty sleeping, and vivid dreams. Mefloquine has very rarely been reported to cause serious side effects, such as seizures, hallucinations, and severe anxiety Doxycycline take daily Take doxycycline on a full stomach to lessen nausea; Women who use doxycycline may develop a vaginal yeast infection. Do not give doxycycline to children under the age of 8; teeth may become permanently stained. Malarone™ take daily Malarone is a new combination of two drugs (atovaquone and proguanil) abdominal pain, nausea, vomiting, and headache can occur. Chloroquine taken weekly nausea and vomiting, headache, dizziness, blurred vision, and itching Quinine: obtained from the bark of a tree in Peru
Quinine has been used for more than three centuries and until the 1930's it was the only effective agent for the treatment of malaria. It is an alkaloid found in the bark of the Cinchona tree and is the only drug which over a long period of time has remained largely effective for treating the disease. It is still used for treating severe falciparum malaria partly but has undesirable side effects. In Africa in the 1930's and 40's it was known for people to take quinine when they thought they had "a touch of malaria" and the association of repeated infections with falciparum malaria and inadequate treatment with quinine, resulted in the development in some of acute massive intravascular haemolysis and haemoglobinuria ie. black water fever. Chloroquine: A very effective 4 -amino-quinoline both for treatment and prophylaxis. It was first used in the 1940 s shortly after the Second World War and was effective in curing all forms of malaria, with few side effects when taken in the dose prescribed for malaria and it was low in cost. Unfortunately many strains of falciparum malaria are now resistant to chloroquine and more recently chloroquine resistant vivax malaria has also been reported.
Stable malaria: continuous transmission year round Unstable malaria: transmission is seasonal In stable malaria: tolerance/resistance can be developed In unstable malaria: tolerance/resistance is often lost
Human malaria: adaptations to the parasite 1) Sickle Cell- single point mutation- abnormal shape of a percentage of RBC will not allow parasite development RBC have bumps on surface- stick to capillary walls, loss of potassium, parasites inside die Only benefit is to heterozygous individuals: double dominant are susceptible double recessive often die from anemia Example of strong evolutionary pressure to respond to a parasite 2) G-6 -Phosphate dehydrogenase deficiency: results in reduced parasitemias 3) Duffy Blood group: double recessive- completely resistant to P. vivax. parasite cannot find receptors to enter RBC Found in 80% of W. African black population
Yahoo and Newspaper column “This weekend, the Pittsburgh Steelers take on the Denver Broncos in the AFC Wildcard playoff game. But Steelers safety Ryan Clark will be watching from the sidelines. Last time he played in Denver, he nearly died. Clark has a sickle cell trait. In 2007, it still hadn't been diagnosed and flared up when he played in Denver. Clark ended up having his gall bladder and spleen removed in addition to losing 30 pounds. This time, he'll be on the bench”. According to the National Heart Lung and Blood Institute, more than two million Americans have sickle cell trait.
Future of malaria management New drugs New insecticides Greater involvement by governments in vector control and monitoring Habitat manipulation to reduce mosquito populations Involve people in their own primary health care Transgenic mosquitoes- resistant to Plasmodium sp.
Vector Populations Some bite indoors, alight on wall for pre-diuresis, then leave homes Some bite indoors, fly outside for pre-diuresis Some only bite outdoors Which ones are susceptible to DDT sprays on houses? “For the next five to ten years, until an effective vaccine is developed, malaria control will largely be dependent on vector control measures such as improvements in housing construction, source reduction, impregnated bednets, and residual insecticide treatment”.
Malaria as therapy? ? ? * Syphilis in Europe had asylums filled with syphilitic paretics: people made crazy, blind, convulsing, by the Treponema pallidum * T. Pallidum very sensitive to temperature * in 1917 Von Jauregg treated syphilitic patients with Plasmodium vivax- allowed 3 -4 bouts of fever- treated with quinine * Institutions using malaria therapy sprouted in Europe and the US, tens of thousands infected people saved * Von Jauregg awarded Nobel prize in 1927