Dyspnea respiratory obstruction UNIT II COMMON SIGNS SYMPTOMS

Dyspnea & respiratory obstruction

UNIT –II COMMON SIGNS & SYMPTOMS TOPIC: Dyspnea & Respiratory obstruction Prepared by, Mrs. Anju Ullas Lecturer Dept. of Medical Surgical Nursing Yenepoya Nursing College

Learning objectives Students will be able to, • define Dyspnea. • list down the causes of dyspnea • clarify the Physiology of Breathing. • understand the Pathophysiology of dyspnea. • Explain the clinical features of dyspnea • mention the Diagnostic Investigations. • enumerate First Aids & Treatments

Dyspnea refers to sudden and severe shortness of breath, or difficulty in breathing.

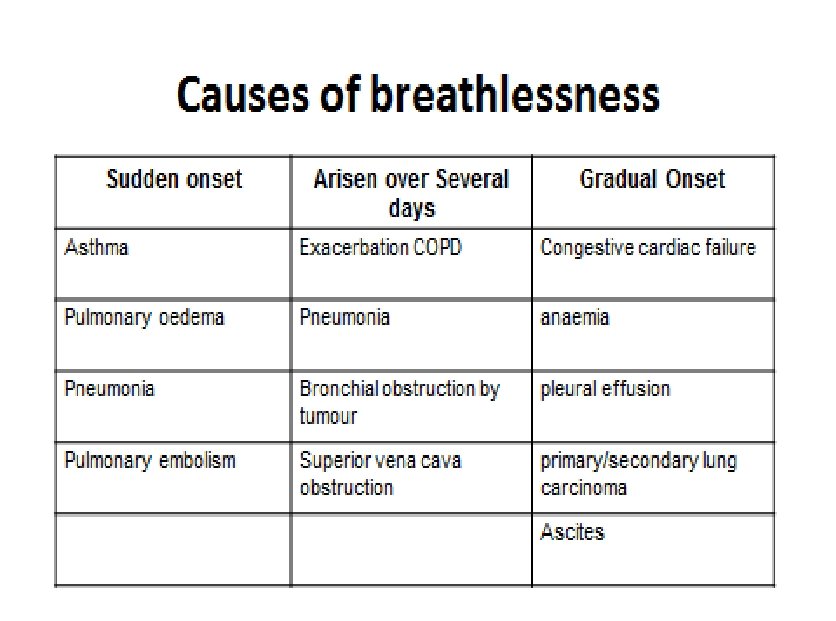
Etiology Four general categories: Cardiac Pulmonary Mixed cardiac or pulmonary non-cardiac nonpulmonary

Pulmonary Etiology COPD Hereditary Lung Disorders Asthma Restrictive Lung Disorders Pneumonia Pneumo- thorax
 Valvular dysfunction Coronary Artery Disease (CAD) Recent or")
Cardiac Etiology Congestive Heart Failure (CHF) Valvular dysfunction Coronary Artery Disease (CAD) Recent or past history of Myocardial Infarction (MI) Cardiomyopathy Left ventricular hypertrophy Pericarditis Arrhythmias

Mixed Cardiac/Pulmonary Etiology COPD with pulmonary HTN and/or cor pulmonale Deconditioning Chronic pulmonary emboli Pleural effusion
 Neuromuscular disorders Pain Functional (anxiety,")
Noncardiac or Nonpulmonary Etiology Metabolic conditions (e. g. acidosis) Neuromuscular disorders Pain Functional (anxiety, panic, hyperventilation) Trauma Chemical exposure

Physiology of Breathing
 Increase in left ventricular and atrial pressure Increase in pulmonary")
Pathophysiology Causes (cardiac cause) Increase in left ventricular and atrial pressure Increase in pulmonary capillary pressure Interstitial edema Vital capacity, restrictive physiology, air trapping Respiratory muscle fatigue Hypoxemia Dyspnea

Clinical features • shortness of breath after exertion or due to a medical condition • feeling smothered or suffocated as a result of breathing difficulties • labored breathing • tightness in the chest • rapid, shallow breathing • heart palpitations • wheezing • coughing
 images to make a more")
Diagnostic evaluation • Chest X-rays • Computed tomography (CT) images to make a more specific diagnosis of dyspnea and evaluate the health of the person's heart, lungs, and related systems. • An electrocardiogram (ECG) may help to show any signs of a heart attack or other electrical problem in the heart. • Spirometry tests to measure airflow and the patient's lung capacity. • ABG analysis

Complication • temporary or permanent cognitive impairment. • Unconsciousness • Paralysis

Management- First Aid call local emergency. Help the person use any prescribed medication Check the airway, breathing, and pulse. If necessary, begin CPR. monitor breathing and pulse. open wounds (esp with air bubbles) in neck or chest must be closed Loosen any tight clothing. Bandage the sucking wound with plastic wrap sealing it except for one corner.
 DO NOT • Do NOT give the person food or")
First Aid (Cont…. ) DO NOT • Do NOT give the person food or drink. • Do NOT move the person if there has been a chest or airway injury, unless it is absolutely necessary. • Do NOT wait to see if the person's condition improves before getting medical help. Get help immediately.

Management Non Pharmacological • Positioning- semi-fowlers position • Ventillation - use of fan /window • Relaxation / Distraction • Controlled Breathing techniques • Loose clothing

Comfortable Positions

Breathing Techniques • Start with position of ease • Relax shoulders / upper chest • Diaphragmatic ‘tummy’ breathing • breath in and Breath out

Pharmacological Management • Oxygen therapy • Steroids – asthma • Bronchodilators (Salbutomol 2. 5 5 mg) • Nebulization – saline to thin secretions – Carbocisteine if secretions difficult to expectorate and exacerbating breathing difficulties

Nursing management Assessment • Assess and record RR and depth at least every hour. • Assist patient to comfortable position, such as supporting upper extremities with pillows. • Assess ABG levels, according to facility policy. • Assess for use of accessory muscle. • Monitor for diaphragmatic muscle fatigue or weakness (paradoxical motion).

• Observe for retractions or flaring of nostrils. • Utilize pulse oximetry to check oxygen saturation and pulse rate. • Assess ability to mobilize secretions. • Observe presence of sputum for amount, color, consistency. • Note for changes in level of consciousness. • Evaluate level of anxiety.

• Evaluate skin color, temperature, capillary refill; observe central versus peripheral cyanosis. • Keep away from high concentration of oxygen in patients with chronic obstructive pulmonary disease (COPD). • Evaluate nutritional status (e. g. , weight, albumin level, electrolyte level).

Nursing diagnosis • Ineffective breathing pattern related to hypoxia as evidenced by shortness of breath/ bronchoconstriction/ use of accessory muscles/ O 2 saturation of 85%/ abnormal ABG analysis.

Nursing interventions • Place patient with proper body alignment for maximum breathing pattern. • A fowlers position permits maximum lung excursion and chest expansion. • Encourage sustained deep breaths by: Ø Using demonstration: highlighting slow inhalation, holding end inspiration for a few seconds, and passive exhalation ØUtilizing incentive spirometer

• Encourage diaphragmatic breathing for patients with chronic disease. • Evaluate the appropriateness of inspiratory muscle training. • Provide respiratory medications and oxygen, per doctor’s orders. • Avoid high concentration of oxygen in patients with COPD.

• Maintain a clear airway by encouraging patient to mobilize own secretions with successful coughing. Suction secretions, as necessary. • Ambulate the patient • Chest physiotherapy • Encourage small frequent meals. • Provide proper ventilation • Educate about breathing and coughing exercises

• Teach patient about: Ø pursed-lip breathing Ø abdominal breathing Ø performing relaxation techniques Ø taking prescribed medications

Respiratory obstruction • An airway obstruction is a blockage in any part of the airway.

Types • Upper airway obstructions • Lower airway obstructions • Partial airway obstructions • Complete airway obstructions • Acute airway obstructions - Choking on a foreign object • Chronic airway obstructions

Causes • inhaling or swallowing a foreign object • small object lodged in the nose or mouth • allergic reaction • trauma to the airway from an accident • breathing in a large amount of smoke from a fire • viral infections • bacterial infections

• respiratory illness that causes upper airway inflammation • swelling of the tongue • abscesses in the throat or tonsils • Injury to the tracheal wall • asthma • Bronchitis • COPD

Clinical manifestation • Tachypnea • Wheezing • Increased respiratory effect • Retraction • Nasal flaring • Prolonged expiration

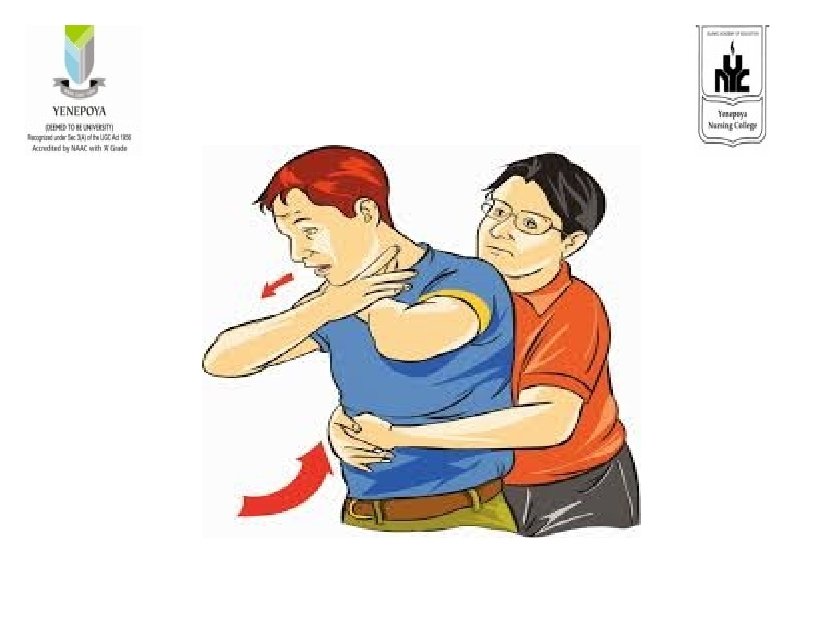
Managment The Heimlich maneuver • The maneuver involves person standing behind the person who is choking, wrapping their arms around the choking person’s waist. • Make a fist and place it in the xiphoid • They should then grab that fist with their other hand press into the person’s abdomen with five quick thrusts.

• Cough • Symptomatic treatment – Bronchodialotors – Nebulizations – Steroids

Prevention • Eat small bites of food. • Eat slowly. • Supervise small children when eating. • Chew thoroughly before swallowing. • Make sure that dentures fit properly. • Keep small objects away from children.

Nursing Diagnosis • Ineffective airway clearance related to respiratory secretions • Ineffective breathing pattern related to hypoxia as evidence by shortness of breath
- Slides: 39