Dysplasia in inflammatory bowel disease Richa Shukla Faculty

Dysplasia in inflammatory bowel disease Richa Shukla Faculty mentors: Dr. Joseph Sellin and Dr. Jason Hou April 30, 2015

HPI • 67 M with history of ulcerative colitis • Diagnosed >20 years ago while living in Mexico, treated only with Asacol • Presented to BTGH with symptoms of UC flare in 2012 – colonoscopy in 5/2012 showed evidence of pancolitis • Treated with prednisone taper and transitioned to maintenance therapy with weight based azathioprine 100 mg daily and Lialda

Colonoscopy 2/2015 • Polypoid area in transverse colon – CHRONIC FOCALLY ACTIVE COLITIS WITH LOWGRADE DYSPLASIA • Sigmoid colon polyp – 1. 5 cm, biopsied – TUBULAR ADENOMA • Random colonic and rectal biopsies – chronic active colitis with low grade dysplasia
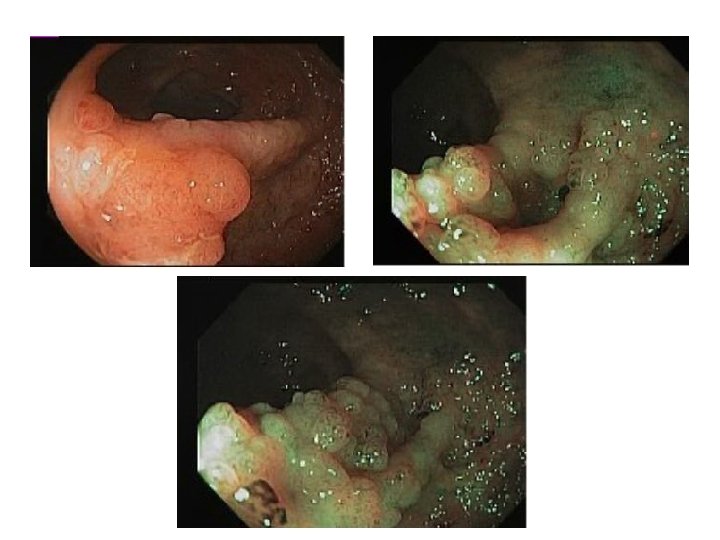

Colon , Transverse, polypoid lesion : LGD

Rectum Bx: LGD

Colon sigmoid, polyp: TA
.")
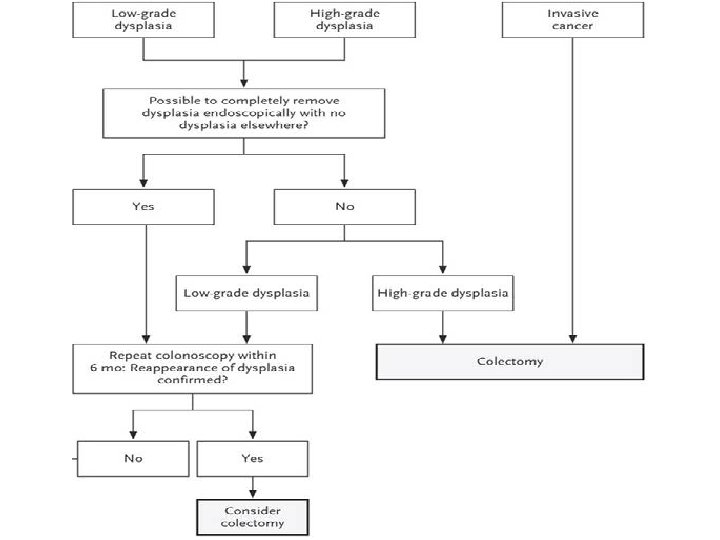
Algorithmic approach to the treatment of dysplasia in patients with inflammatory bowel disease (IBD). DALM, Dysplasia-associated lesion or mass.

Summary of Differentiating Features between IBD-Associated Polypoid Dysplasia and Sporadic Adenomas Feature Dysplasia Probable Adenoma Probable Polypoid Dysplasia Patient age Older (>60 years) Younger (<50 years) Extent of disease Usually subtotal Usually total Disease activity Usually inactive Usually active Disease duration Shorter (<10 years) Longer (>11 years) Polyp location Usually non-diseased area (more R colon) Diseased area (more L colon) Associated flat dysplasia Never Occasionally Increased lamina propria inflammation Usually absent Usually present Villous architecture Usually absent Occasionally present Mixture of benign and Usually absent dysplastic crypts at surface of polyp Usually present LOH of 3 P Uncommon Common LOH of P 16 Rare Common Odze Mod Pathol 2003; 16(4): 347– 358

Clinical Questions • What is the epidemiology of colorectal cancer in inflammatory bowel disease? • What is the risk of cancer in a patient with dysplasia? • What are the guidelines for dysplasia surveillance and management in IBD?

Clinical Questions • What is the epidemiology of colorectal cancer in inflammatory bowel disease? • What is the risk of cancer in a patient with dysplasia? • What are the guidelines for dysplasia surveillance and management in IBD?

Ulcerative colitis and colorectal cancer • Risk of CRC depends upon extent and duration of disease • Greatest risk of cancer: disease extending to the hepatic flexure or more proximally • >19000 patients followed for 35 months – Longstanding and extensive colitis (LEC) had increased risk for CRC compared with general population (HR 7. 0) – Without LEC, risk was equivalent to general population (HR 1. 1) Beaugerie et al. Gastroenterology. 2013 Jul; 145(1): 166 -175. e 8

Ulcerative colitis and colon cancer • Risk increases 8 -10 years after symptom onset • Incidence of colon cancer in patients with pancolitis estimated at 5 -10% after 20 years of disease, 12 -20% after 30 years Mir-Madjlessi SH et al Cancer. 1986; 58(7): 1569. Eaden JA et al Gut. 2001 Apr; 48(4): 526 -35.

UC, PSC and risk of colon cancer • Increased risk of cancer in patients with UC and PSC – Historical cohort study of 132 patients with UC and PSC: 33 (25%) developed cancer or dysplasia v. 11 (5. 6%) of 196 control patients (UC without PSC) • Right sided cancer more common – 17 cancers in PSC group – 76% were proximal to splenic flexure, 35% advanced stage v. control group with 1/5 proximal and none advanced stage • Possible role of bile acids in oncogenesis Shetty K et al Am J Gastroenterol. 1999; 94(6): 1643.

Crohn’s disease and CRC Study Location Number of patients Risk of CRC Van den Heuvel et al Netherlands 1162 patients 33% increased risk of developing CRC as compared with general population Ekbom et al Sweden 1655 patients -RR 2. 5 for CRC -RR 5. 6 for colonic disease -RR 21 for those diagnosed <30 years of age Van den Heuvel J Crohns Colitis. 2015 Feb; 9 Suppl 1: S 33 -5. Ekbom et al Lancet. 1990 Aug 11; 336(8711): 357 -9.

Declining risk of colon cancer? • CRC risk in a nationwide cohort of 47, 374 Danish IBD patients from 1979 -2008 – 268 UC patients, 70 CD patients developed CRC – UC: overall RR for CRC decreased from 1. 34 in 1979– 1988 to 0. 57 in 1999– 2008. • Increased risk of CRC: those diagnosed in childhood (RR 43. 8), those with long duration of disease (RR 1. 5), and those with concomitant PSC (RR 9. 16) – CD: overall RR for CRC was 0. 85, no change over time. Jess T et al Gastroenterology. 2012 Aug; 143(2): 375 -81. e 1

Risk factors for CRC in IBD • Factors that increase CRC risk: – Long duration of colitis – Extensive colonic involvement – Family history of colorectal cancer – Primary sclerosing cholangitis – Young age of IBD onset (some studies) – Backwash ileitis – marker of severe disease – ? Severity of inflammation Itzkowitz et al Gastroenterology. 2004 May; 126(6): 1634 -48 Heuschen et al Gastroenterology. 2001 Mar; 120(4): 841 -7. .

Clinical Questions • What is the epidemiology of colorectal cancer in inflammatory bowel disease? • What is the risk of cancer in a patient with dysplasia? • What are the guidelines for dysplasia surveillance and management in IBD?
")
Risk of cancer with dysplasia • Meta-analysis of 10 prospective studies (1225 UC patients) on surveillance colonoscopy – At immediate colectomy, risk of cancer with HGD was 42%, was 19% for LGD – When HGD found after initial colonoscopy, 32% patients also had cancer – 16 -29% of patients with untreated LGD progressed to high-grade dysplasia, or cancer. – 2. 4% of patients with negative studies progressed to HGD, DALM or cancer Bernstein et al Lancet. 1994 Jan 8; 343(8889): 71 -4.

High grade dysplasia • Risk of concurrent cancer high in HGD in UC and CD • Finding of HGD warrants colectomy • Management of HGD in CD identical to UC – For segmental Crohn’s colitis, unknown if segmental resection sufficient or if total proctocolectomy should be considered Maykel et al Dis Colon Rectum. 2006 Jul; 49(7): 950 -7 Itzkowitz et al Inflamm Bowel Dis. 2005 Mar; 11(3): 314 -21.

Progression of low grade dysplasia Study Number of patients Risk of progression to CRC or HGD Ullman et al 46 patients -7 cases CRC -4/17 advanced neoplasia at colectomy (for LGD) -Rate of progression – 53% at 5 years Thomas et al Meta-analysis, 20 studies -508 patients (477 flat LGD, 31 LGD +DALM) -9 x risk of CRC once LGD diagnosed -12 x risk for advanced neoplasia -High PPV for CRC with LGD+DALM Navaneethan et al 997 patients -102 with LGD -4. 9% progressed to advanced neoplasia over 3 years -Distal colonic flat LGD progression – HR 3. 6 Thomas et al Aliment Pharmacol Ther. 2007 Mar 15; 25(6): 657 -68. Navaneethan et al J Crohns Colitis. 2013 Dec 15; 7(12): e 684 -91 Ullman et al Gastroenterology. 2003 Nov; 125(5): 1311 -9.

Progression of low grade dysplasia • No consensus on management of UC and LGD • LGD is predictor of advanced neoplasia

Colitis associated dysplastic lesions • Formerly known as DALM • High risk of progression to CRC, high risk of concurrent cancer • Difficult to differentiate from sporadic adenomas • Important to biopsy base of any removed polyp to assess for dysplasia • Indication for colectomy • Case series of 12 patients with polypoid dysplasia – Carcinoma present in resection specimens in 7/12 of cases Blackstone et al Gastroenterology. 1981 Feb; 80(2): 366 -74 Neumann et al World J Gastroenterol. 2011 Jul 21; 17(27): 3184– 3191.

Pseudopolyps • Residual mucosal islands of stroma, epithelium, and inflammatory cells found between regions of repeated mucosal ulceration and regeneration • No malignant potential • May be associated with higher risk of CRC - 188 patients with UC associated cancer studied - Pseudopolyps associated with increased risk of CRC (OR 2. 5, 95% CI: 1. 4– 4. 6) Velayos et al Gastroenterology. 2006 Jun; 130(7): 1941 -9 .

Pseudopolyps • Association between pseudopolyps and CRC may represent: – improper recognition of malignant polypoid lesions – mucosal lesions obscured by pseudopolyps – Difference in the number of biopsy specimens taken in patients with and without pseudopolyps – pseudopolyps are a visible surrogate marker of significant inflammation predisposing to cancer

Clinical Questions • What is the epidemiology of colorectal cancer in inflammatory bowel disease? • What is the risk cancer in a patient with dysplasia? • What are the guidelines for dysplasia surveillance and management in IBD?
 recommend")
CRC Surveillance in IBD • AGA and European Crohn’s and Colitis Organisation (ECCO) recommend surveillance begin after 8 years of colitis or from time of diagnosis of PSC • British Society of Gastroenterology recommends surveillance after 10 years of colitis, chromendoscopy preferred method
: 1441 -52")
Beaugerie et al N Engl J Med. 2015 Apr 9; 372(15): 1441 -52

Newer surveillance guidelines • SCENIC International consensus statement – After complete removal of endoscopically resectable polypoid and nonpolypoid dysplastic lesions, surveillance colonoscopy is suggested rather than colectomy – For endoscopically “invisible” dysplasia – recommend surveillance HD colonoscopy with CE by expert IBD endoscopist – Discontinuation of adenoma-like, non-adenoma like DALM Laine et al Gastroenterology. 2015 Mar; 148(3): 639 -651. e 28

Novel endoscopic technologies • Narrow band imaging • Confocal laser endomicroscopy • Chromendoscopy with methylene blue, indigo carmine – May increase detection of dysplastic lesions – Thus far studies have not proven increased detection of unexpected cancer – Subject to the skill of the endoscopist Farraye et al Gastroenterology. 2010 Feb; 138(2): 738 -45.

Role of novel endoscopic technologies • AGA Position statement 2010: – “Thus, at this time, normal white light colonoscopy, using standard or high-definition colonoscopes along with multiple colon biopsies, remains a reasonable method of surveillance for patients with IBD. However, chromoendoscopy with targeted biopsies is considered an acceptable alternative to white light endoscopy for endoscopists who have experience with this technique. ” Farraye et al Gastroenterology. 2010 Feb; 138(2): 738 -45.

Role of chromoendoscopy • SCENIC Consensus Statement – When performing surveillance with standarddefinition or high-definition colonoscopy, chromoendoscopy is recommended rather than white-light colonoscopy. – CE increases detection of dysplasia, though whethere is associated increased risk of CRC is unknown Laine et al Gastroenterology. 2015 Mar; 148(3): 639 -651. e 28

Chromoendoscopy • Retrospective cohort study, 440 colonoscopies in 401 patients with chromoendoscopy, compared with 1802 colonoscopies in 772 patients undergoing WLE – Chromoendoscopy group: Dysplasia detected during 48 surveillance procedures (11%) – WLE: Dysplasia in 189 procedures (10%) – Conclusion: no significant difference in dysplasia detection between WLE and chromoendoscopy Mooiweer et al Am J Gastroenterol. 2015 Mar 31

Back to our patient • Underwent flex sig in 3/2015 with removal of sigmoid polyps; tubular adenoma and serrated adenoma found • Patient was offered colectomy given finding of dysplasia, abnormal polypoid lesions on multiple colonoscopies • He has elected to undergo close surveillance program with q 6 month colonoscopy for now • Clinically, symptoms are controlled on current medical regimen

Take Home Points • Risk of colorectal cancer is likely increased in UC and CD, the risk is largely related to duration and extent of disease • HGD and colitis associated dysplastic lesions have a high risk of progression to cancer or even concurrent cancer and likely warrant colectomy • Management of LGD is more subjective though there is a substantial risk of progression to advanced neoplasia

Take Home Points • Surveillance is recommended in UC and likely in CD as well • Novel endoscopic technologies may increase rate of dysplasia detection though this is still user dependent

Thank you!
- Slides: 38