DYSPHAGIA By Dr Olayiwola Adeyemi NITMED TUTORIALS ANATOMY

DYSPHAGIA By Dr Olayiwola Adeyemi ©NITMED TUTORIALS

ANATOMY OF THE OESOPHAGUS �Hollow muscular tube which begins at level of C 6 and end at the OG junction (T 12) � 25 cm in length from upper border of the cricopharyngeus/ 40 cm from the upper incisors �Lack serosa layer �Contains 2 different types of muscle �Upper 1/3 - striated muscle �Lower 2/3 - smooth muscle �Lined by squamous epithelium except for lower 2 - 3 cm which correspond to the squamo-columnar junction(OG junction) �Has segmental blood supply

� Divided into 3 part �Cervical �Thoracic �Abdominal � Areas of anatomic narrowing �Cricopharyngeus �Bronchoaortic constriction �Diaphragmatic � Arterial supply: inf. Thyroid, inf. Phrenic esophageal branches of aorta, gastric artery � Venous drainage: inf. Thyroid, bronchiocephalic, left hemiazygous, azygous vein, splenic vein and inferior phrenic vein

�Lymphatic drainage: lymphatic drainage arranged longitudinally and it drains into paraoesophageal, perieosphageal and lateral esophageal group �Nerve supply: vagus and intrinsic supply (mainly Auberch plexus) �Types of peristalsis �Primary: progressive and triggered by swallowing �Secondary: progressive and generated by distention or irritation �Tertiary: non progressive initiated by left over food in the esophagus �LES is a physiologic with resting pressure of 10 - 25

Definition �A subjective awareness of difficulty in swallowing caused by impaired progression of matter from pharynx to stomach. �TYPES �preoesophageal dysphagia �esophageal dysphagia

PREOESOPHAGEAL DYSPHAGIA � Difficulty emptying bolus material from the oropharynx into the esophagus. � Abnormal function proximal to the esophagus � Causes � Myaesthenia gravis � Muscular dysthrophy � Bulbar poliomyelitis � Pseudobulbar palsy � Parkinson’s disease

OESOPHAGEAL DYSPHAGIA �Difficulty passing food down the esophagus. �Causes o Congenital o Acquired

Oesophageal Dysphagia �Causes �Congenital o Associated with esophageal atresia/ tracheooesophageal fistula o Webs o Dysphagia lusoria �Acquired �Diseases of the wall of the esophagus �Intraluminal lesions �Extrinsic pressure on the esophagus �Diseases of the stomach

Disease of the wall of the esophagus � Carcinoma of the esophagus � Benign tumours � Oesophagitis/ stricture � Corrosive burns ( acids, alkalis, various chemicals) � Reflux oesophagitis � Perforation � Oesophageal diverticulae � Neuromuscular dysfunction � Achalasia cardia � Diffuse spasm � Connective tissue diseases � Scleroderma � SLE � Polyarteritis nodosa

OESOPHAGEAL DYSPHAGIA �Acquired �Diseases of the wall of the esophagus �Intraluminal lesions �Extrinsic pressure on the esophagus �Diseases of the stomach

Intraluminal Lesions �Impacted foreign bodies �Bolus obstruction e. g welle! �Oesophageal web→ Plummer-Vinson Syndrome �Schatzki’s ring


OESOPHAGEAL DYSPHAGIA �Acquired �Diseases of the wall of the esophagus �Intraluminal lesions �Extrinsic pressure on the esophagus �Diseases of the stomach

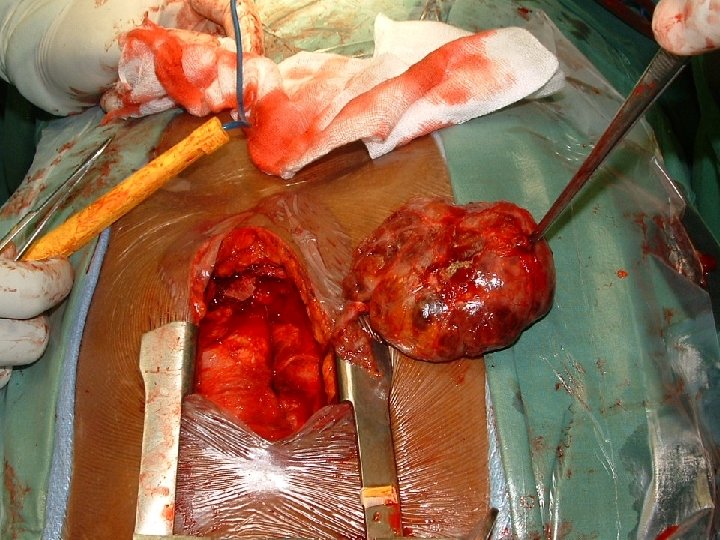
Extrinsic pressure on the esophagus �Goitre – neck or mediastinum �Enlarged mediastinal lymph nodes �Mediastinal tumours �Aneurysm of ascending or arch of the aorta

OESOPHAGEAL DYSPHAGIA �Acquired �Diseases of the wall of the esophagus �Intraluminal lesions �Extrinsic pressure on the esophagus �Diseases of the stomach : Carcinoma of the cardia.

MANAGEMENT OF DYSPHAGIA �History �Physical examination �Investigations �Treatment

History AGE �Neonate -Congenital �Child: -Foreign body �Third or fourth decade: -Achalasia �Elderly: -Carcinoma

History �History of accidental or suicidal ingestion of corrosive, or swallowing of a foreign body �History of dyspepsia �History of alcoholism/smoking �Duration of Symptoms

Duration of symptoms �Very short history suggests inflammatory or traumatic lesion �Long and intermittent – Achalasia �Long and progressive – Stricture �Short and progressive – Carcinoma

MANAGEMENT OF DYSPHAGIA �History �Physical examination �Investigations �Treatment

Physical examination �Usually unhelpful �Weight loss �Anaemia �Dehydration �Peripheral lymph nodes �Epigastric mass

MANAGEMENT OF DYSPHAGIA �History �Physical examination �Investigations �Treatment

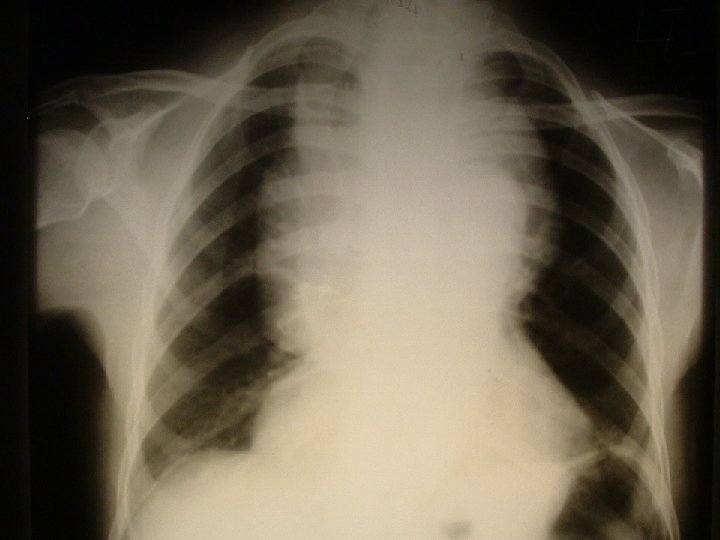
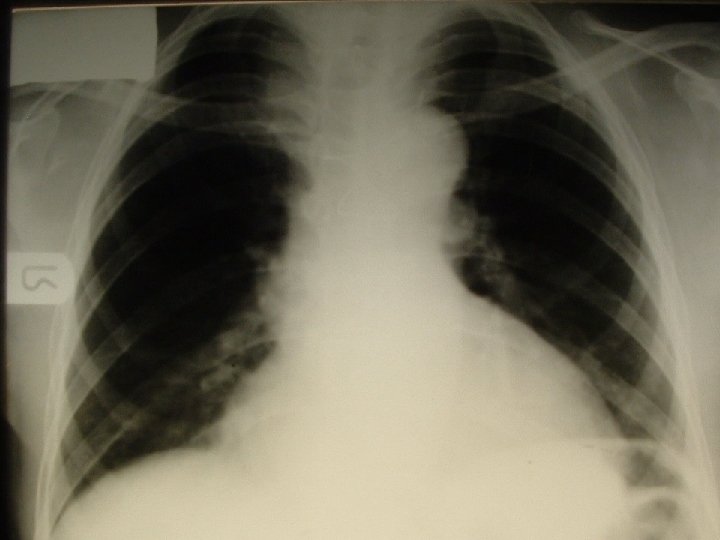
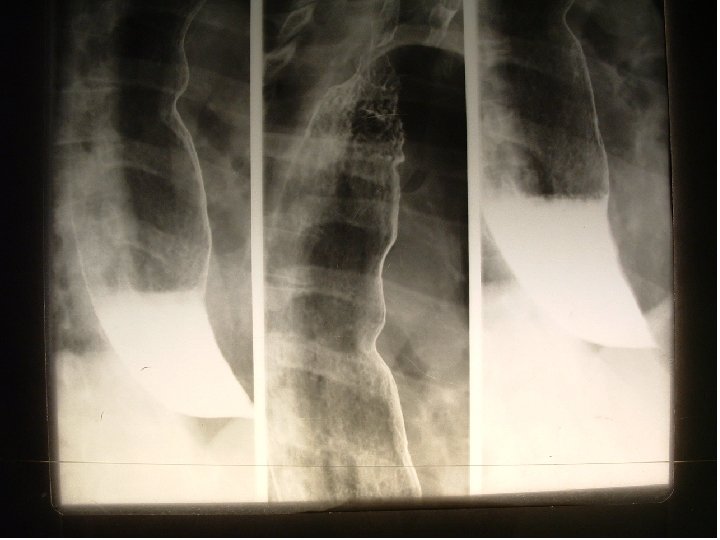
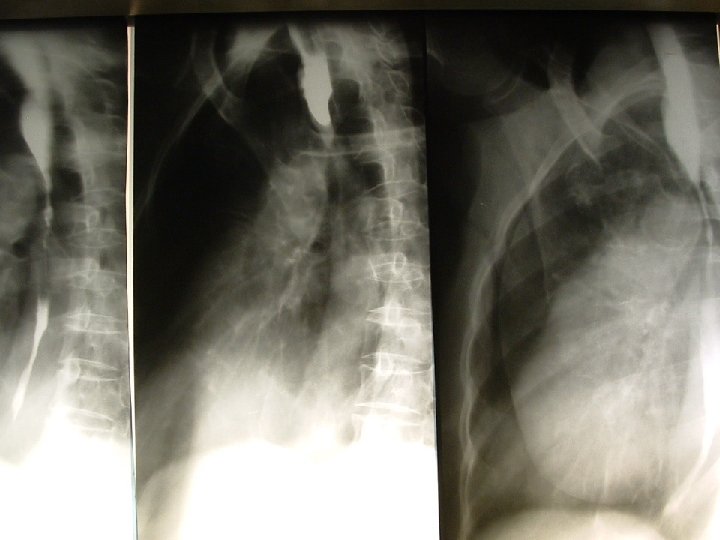
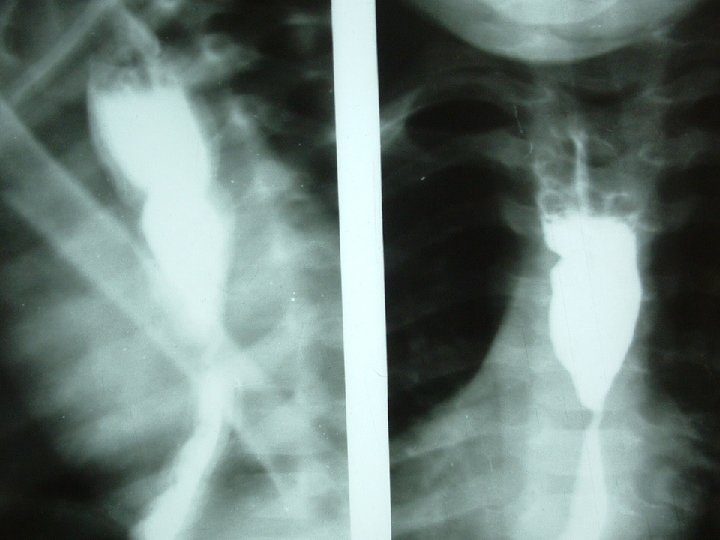
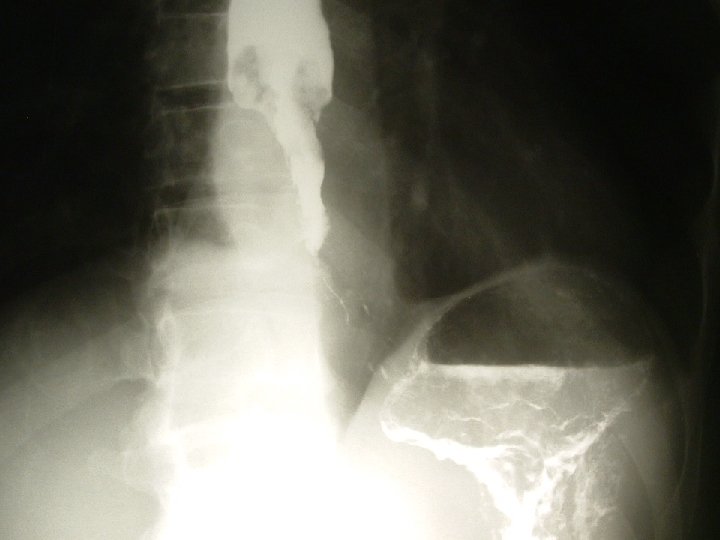
Investigations � Chest X-ray o FB, Widened mediastinum, retrosternal or mediastinal masses � Barium swallow. o Precedes oesophagoscopy- very important � Oesophagoscopy o identifies lesion and allows biopsy � Manometry o achalasia � CT scan, MRI, USS � Full Blood Count, BUE, LFTs, etc.

MANAGEMENT OF DYSPHAGIA �History �Physical examination �Investigation �Treatment

TREATMENT �Depends on the diagnosis

ACHALASIA OF THE CARDIA

DEFINITION �Motility disorder of esophagus of unknown aetiology characterized by: �Absence of peristalsis in the body of the esophagus �High resting pressure in the lower esophageal sphincter �Inadequate or incomplete relaxation of the LES in response to swallowing �Hypertrophy and dilatation of the esophagus

AETIOLOGY � Cause is unknown � Neurological basis o Generally accepted o Supported by absence/ or diminished ganglion cells of Auerbach’s plexus. � Vagus nerve dysfunction o Indicated by abnormalities of gastric secretion, also supports neurologic aetiology o Similar clinical condition created in cats by destruction of the vagal nuclei � Chagas’ disease(Trypanosoma cruzi infection) o In south America o Show changes in Auerbach’s plexus indistinguishable from those of Achalasia
 In South America Produces lesions indistinguishable from achalasia")
AETIOLOGY �Chagas Disease (Trypanosoma cruzi infecton) In South America Produces lesions indistinguishable from achalasia

Pathology �Oesophageal obstruction at the gastro- oesophageal junction with thickening and tonic contraction of the sphincter �Proximal esophageal dilatation with hypertrophy of the muscle layer �Advanced cases show marked proximal dilatation with food stasis and tortuosity of the esophagus

Clinical Features � High incidence in patients btw 30 - 60 yrs � M: F is 1: 1 � Dysphagia with sticking sensation in the substernal area � Precipitated by an emotional disorder � Odynophagia in 30% of patents, especially with cold fluids � Weight loss – long standing achalasia � Malignant change ( middle of esophagus)

Clinical Features �Retrosternal Pain �Regurgitation of food after meals and in late stages during sleep �Tracheobronchopulmonary soilage results in recurrent bouts of bronchitis, pneumonia and lung abscess. �Weight loss-long standing achalasia �Malignant change

Investigations CXR: widened mediastinum with or without an air fluid level Absent gastric air bubble Barium swallow with fluoroscopy: shows dilated esophagus, lack of peristalsis, retained food in the esophagus


Investigations � Oesophagoscopy Stasis, dilated esophagus with retained food oesophagitis r/o carcinoma or other causes of stricture � Manometric evaluation -failure of relaxaton of the LES -absent peristalsis in the body of the esophagus -elevated LES pressure

TREATMENT �Aim is to relieve obstruction caused by the hypertensive LES �Medical �Surgical

TREATMENT �Medical – 50 - 60 % satisfactory �Dilatation of lower sphincter o Mechanical o Pneumatic- Stark dilator o Hydrostatic- Negus hydrostatic bag Complications: Perforation, gastro-oesophageal reflux �Nitrates and calcium channel blockers. Results limited by side effects �Botulinum toxin

TREATMENT �Per oral endoscopic myotomy �HELLER MYOTOMY

CORROSIVE OESOPHAGEAL STRICTURES

INTRODUCTION �Occurs in both developed and developing countries �Bimodal age distribution �Children under the age of 5 years � Adults �The bimodal age distribution also reflects the aetiology in the different age groups 44

AETIOLOGY �Ingestion of strong acid or alkali �Children under 5 years of age- accidental ingestion �The result of an inquisitive toddler ingesting improperly stored corrosive substance �Usually the first swallow of the noxious substance stops further ingestion 45

AETIOLOGY �In adults the ingestion of large amounts of caustic agents is a suicide attempt �Recently forceful ingestion of caustic substances as instant justice for suspected robbers �Other causes: long term indwelling nasogastric tube, chronic reflux oesophagitis 46

PATHOLOGY �Ingestion of strong acid produces coagulation necrosis which limits the depth of injury �Ingestion of strong alkali produces liquefaction necrosis and an increased depth of injury 47

PATHOLOGY �Considerable damage to the mouth, buccal cavity, pharynx, esophagus, stomach down to the jejunum �The laryngotracheal inlet may be affected �Toxic fumes may damage the lung parenchyma 48

PATHOLOGY �Oesophagus mostly damaged at physiological points of narrowing-cricopharyngeus, level of tracheal bifurcation, distal thoracic esophagus �Severity of injury depends on the concentration of the agent, duration of contact with the mucosa and the nature of the agent- alkalis cause severe damage to the esophagus 49

PATHOLOGY �Necrosis and sloughing of tissues �Ulceration of variable depth �In severe cases perforation into the mediastinum, pericardium, pleural or peritoneal cavity �Ulceration results in secondary infection �Compounded by acid reflux �Intense fibrotic reaction �Healing results in stricture in 3 weeks to three months 50

PATHOLOGY Bremner classified corrosive stricture into 3 degrees � First degree: Hyperaemia and oedema of the mucosa only � Second degree: Damage extends to the submucosa, blisters with vesicles and pseudomembrane formation � Third degree: Necrosis extends to perioesophageal tissues with mediastinal, pleural or peritoneal perforation. There is eschar formation 51

CLINICAL FEATURES �There is a history of ingestion of a caustic fluid �Obtain a history of estimated amount and nature of ingested agent �Dysphagia �Burning pain in the mouth, throat, retrosternum and epigastrium especially on swallowing 52

CLINICAL FEATURES �Nausea, vomiting and diarrhoea. Vomitus may be bloodstained �Difficulty in breathing, stridor, hoarseness �Shock-hypotension, rapid thready pulse, pallor, sweating- in severe cases �Discoloured and oedematous skin around the mouth and the mucosa of the mouth �Temperature from secondary infection, mediastinitis, pneumonia from aspiration 53

CLINICAL FEATURES COMPLICATIONS �Shock �Perforation of the esophagus or stomach �Bleeding �Mediastinitis �Pneumonia �Septicaemia �Stricture �Gastric outlet obstruction �Malignant change 54

CLINICAL FEATURES CAUSTIC STRICTURE �History of caustic ingestion �Increasing dysphagia �Malnutrition �Dehydration �Anaemia �Electrolyte imbalance �Vitamin deficiencies 55

MANAGEMENT INVESTIGATIONS �X-Rays- Chest and abdomen to detect evidence of perforation or respiratory complications �When general status is stable- flexible fibreoptic oesophagogastroduodenoscopy �Barium swallow at 3 to 4 weeks 56

ACUTE MANAGEMENT �Admit patient and place on NPO �Do not induce vomiting to avoid repeat exposure of injured area to the agent �Fluid resuscitation �Broad spectrum antibiotic therapy �Prophylactic acid suppression medication 59

MANAGEMENT �Pain relief �Steroids? ? ? �Intubation or tracheostomy and ventilation if there is significant laryngotracheal injury �Parenteral nutrition 60

MANAGEMENT �First degree injury- no specific treatment- 61 graded oral intake �For more severe injury- careful dilatation from three weeks �Feeding gastrostomy or jejunostomy �Resection of esophagus with cervical oesophagostomy and a feeding gastrostomy for transmural necrosis with mediastinitis- delayed reconstruction

MANAGEMENT ESTABLISHED STRICTURE �Intermittent dilatation- antegrade or retrograde �Oesophageal reconstruction with colon, stomach or jejunum 62

CARCINOMA OF THE OESOPHAGUS

AETIOLOGY �Not definitely known �Endemic/ high prevalence areas o China, Japan, Iran, Chile, Puerto Rico etc. �Associated factors o Age- 5 th – 6 th decade o Dietary factors – alcohol, tobacco, malnutrition & Nitrosamine o Premalignant – Plummer-Vinson Syndrome, Barret’s esophagus, Lye burns of esophagus o Familial lesions – tylosis
 �Primary adenocarcinoma �Adenocarcinoma in a Barret’s esophagus")
PATHOLOGY �Squamous cell Ca commonest ( >95%) �Primary adenocarcinoma �Adenocarcinoma in a Barret’s esophagus �Adenoid cystic Ca �Mucoepidermoid Ca

Pathology �Early lesion �Erosive lesions �Plaques �Papillary �Advanced lesion �Fungating lesion �Ulcerative lesion �Infilterative lesion ( tend to produce malignant strictures)

Clincal features � Progressive dysphagia o From solid → semisolid → liquid and saliva � Weight loss and weakness � Regurgitation/ Aspiration/ Haematemesis/ Melaena � Adjacent structure involvement � Persistent back pain : paravertebral fascia � Hoarseness & Dysphonia : Recurrent Laryngeal Nerve � Hiccups : Phrenic nerve & diaphragm � Respiratory difficulty: tracheal, bronchi

Investigations �Diagnostic �Barium swallow �Oesophagoscopy + biopsy/ smear for cytology �Chest x-ray �CT scan of chest �USS abdomen �Supportive �FBC �BUE, Cr �LFT’s


TREATMENT �Depends on stage �Early lesions � Limited to esophagus, no lymph node or metastasis � Suitable for curative resection �Advanced lesions � Benefit from palliative treatment

TREATMENT �Surgery �curative �palliative �Chemotherapy �Radiotherapy �Oesophageal intubation �Photodynamic therapy

TREATMENT �Palliative surgery � Bypass; stomach o Gastric tubes o Whole stomach o Colon �Resection + replacement/ bypass �Endoprosthesis


THANK YOU
- Slides: 75