Dynamic Auscultation Listening to the change in character


CAL Postural change Supine / L Lateral Standing Squatting Valsalva Handgrip")







































- Slides: 69
Dynamic Auscultation Listening to the change in character, behaviour and the intensity of the heart sounds and murmurs to physiological and pharmacological maneuvers……. “AUSCULTATE WITH ALTERED HEMODYNAMICS”
Dynamic Auscultation • Source of murmur : Right Heart ~ Left Heart • Differentiate closely simulating murmurs Outflow ~ Regurgitatnt murmur • Differentiate flow murmurs from those of structural deformity : Austin Flint ~ MS • Differentiate Dynamic from Fixed Obstructions
Maneuvres • • PHYSI(OLOGI)CAL Postural change Supine / L Lateral Standing Squatting Valsalva Handgrip Cycle length change PHARMACOLOGICAL • Amyl nitrite • Phenylephrine
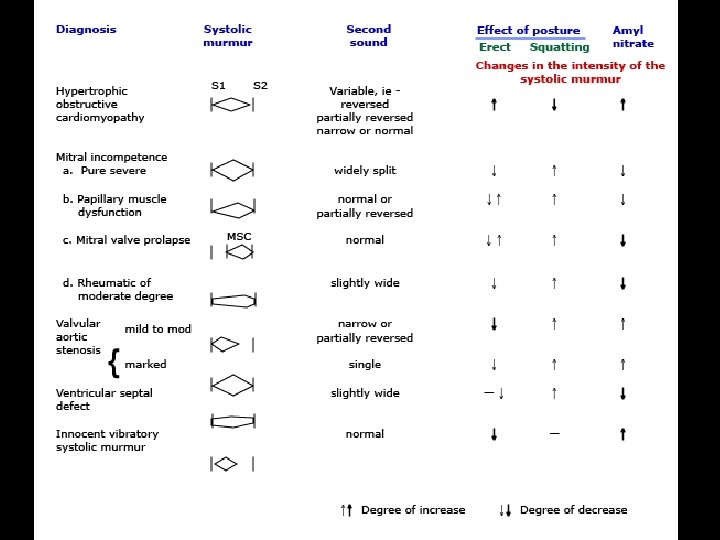
Position • Left lateral decubitus : Augments the murmur of MS, MR, Austin Flint, MVP & S 1, LV S 3 & S 4 • Sitting & Leaning forward : ↑ AR murmur • Sitting with arms raised above the head : ↑ AR • Knee chest position : AR, Pericardial Rub • Passive leg raising : ↑ VR >↑ Right Heart events
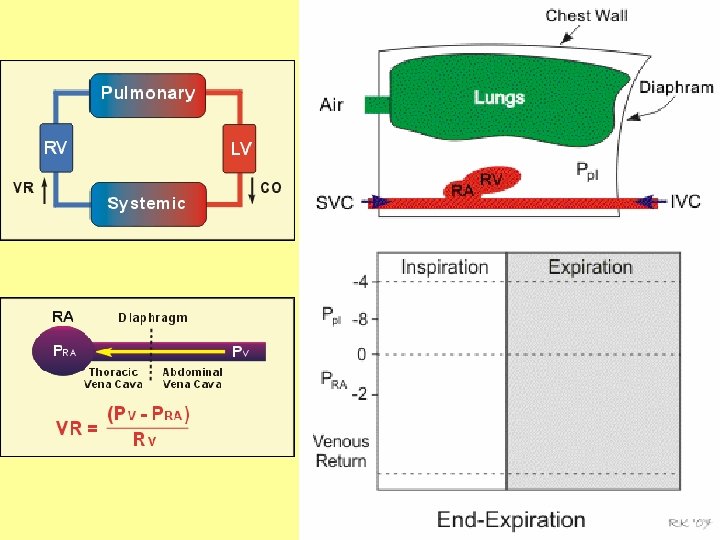
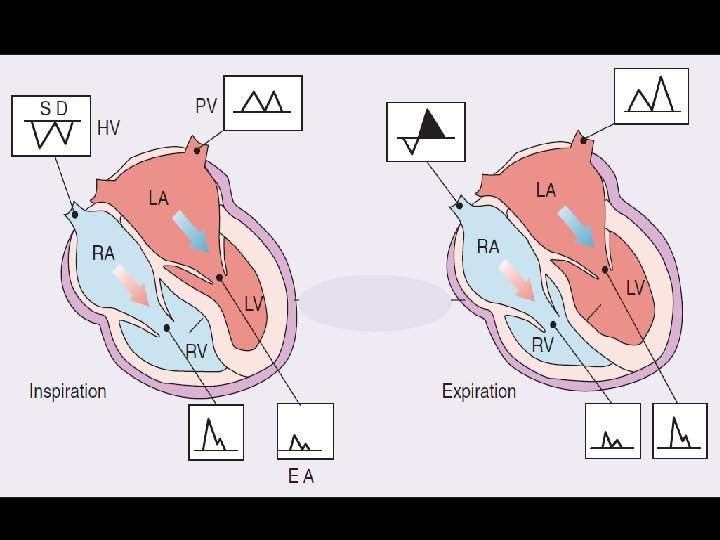
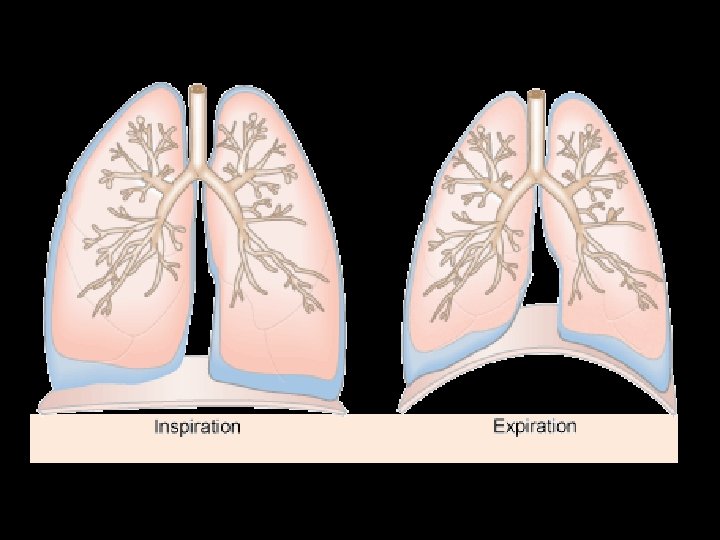
Respiration • Inspiration augments right sided events, as the venous return increases : TR & TS , PR & PS murmurs ; RV S 3, S 4 & TV OS S 1 & S 2 split widen. • Exception is PES – augmented in expiration # Preferably quiet respiration # Avoid apnea # Listen the first few beats # In erect posture if Venous pressure is high
Carvallo’s sign Inspiratory accentuation of TR murmur Early systolic murmur > holosystolic Blowing quality > musical Absent in severe RV failure associated TS is severe • If venous pressure is very high, listening in upright posture may help • •
Reversed Carvallo sign HCM with RVO obstruction - ? ↑ VR > widened RVO
Respiration • Left sided events are better heard in expiration MR, MS, AS & AR murmurs LV S 3 & S 4, Mitral OS Click & murmur of MVP occur later @ PV – LA gradient increases > ↑ LV filling @ Lung overlap decreases @ Apnea for faint AR murmur
Pms = mean systemic pressure; Ppc = pulmonary capillary hydrostatic pressure; Ppi = pulmonary interstitial hydrostatic pressure; Ptm = pulmonary capillary transmural pressure
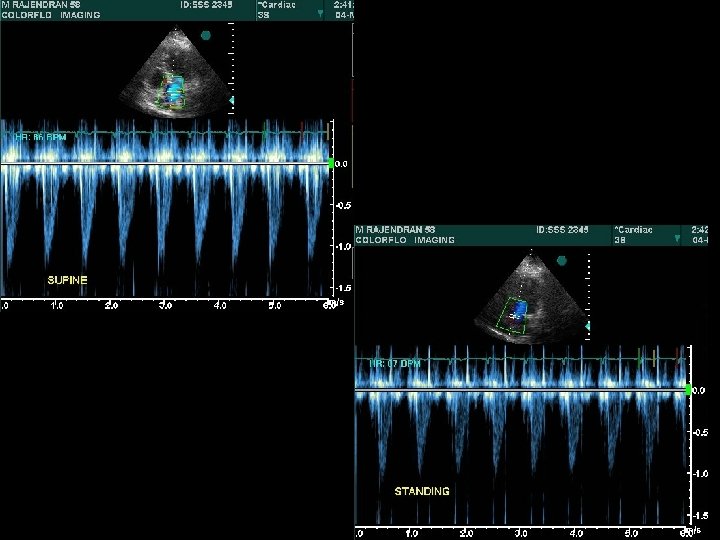
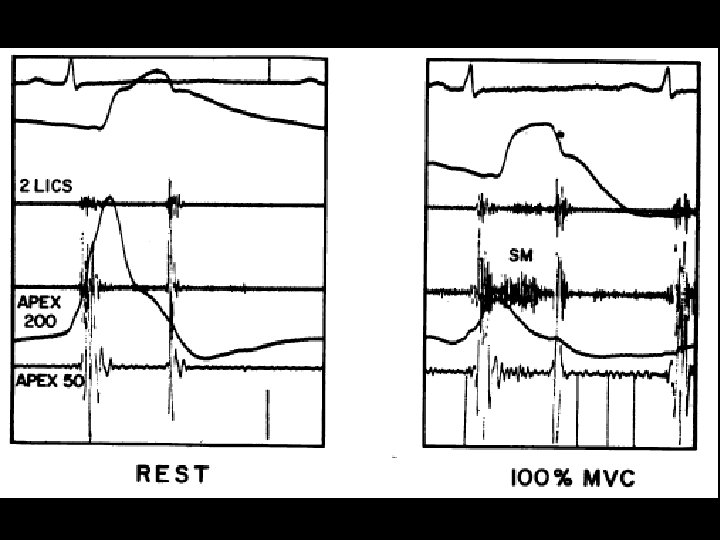
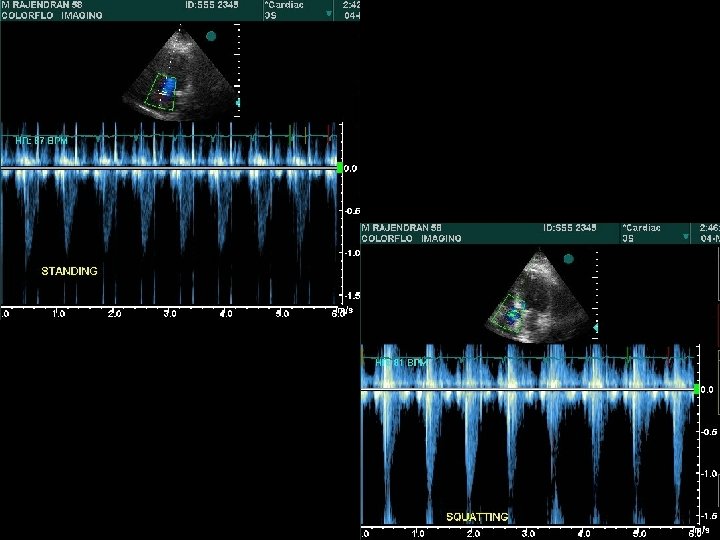
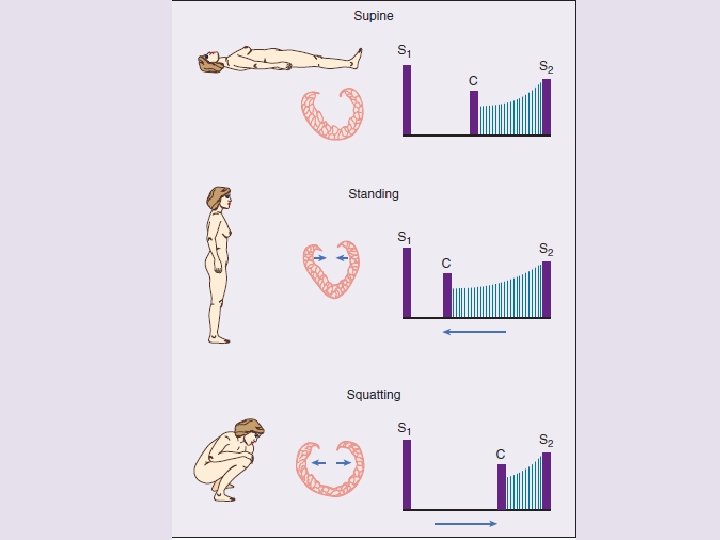
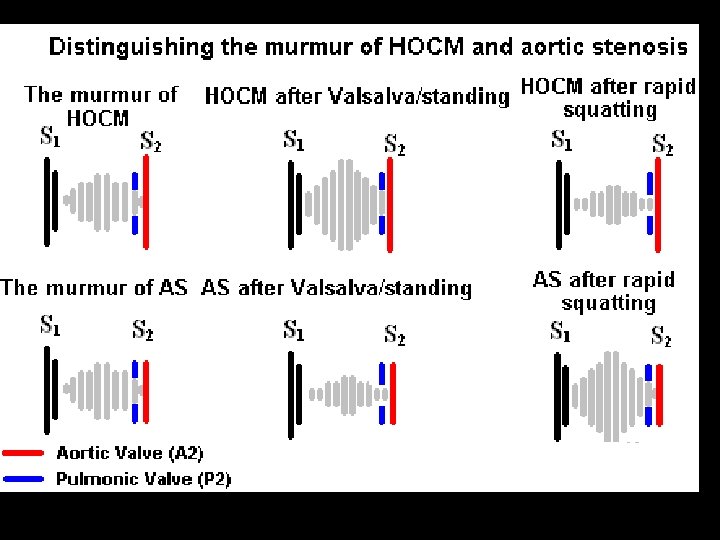
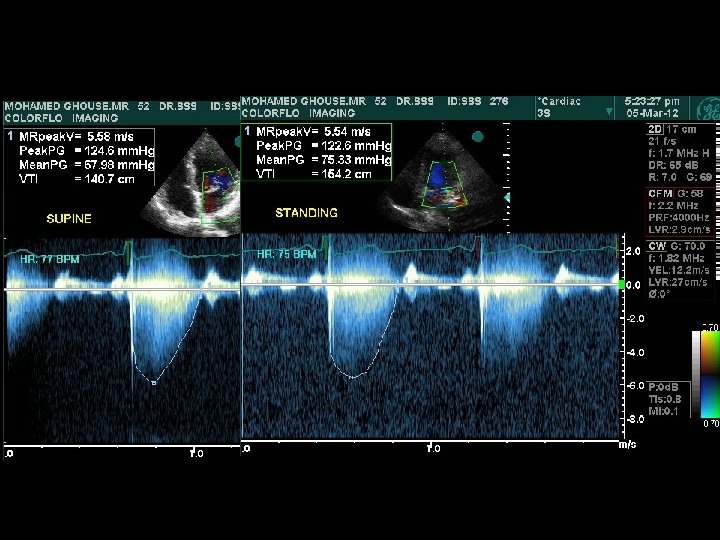
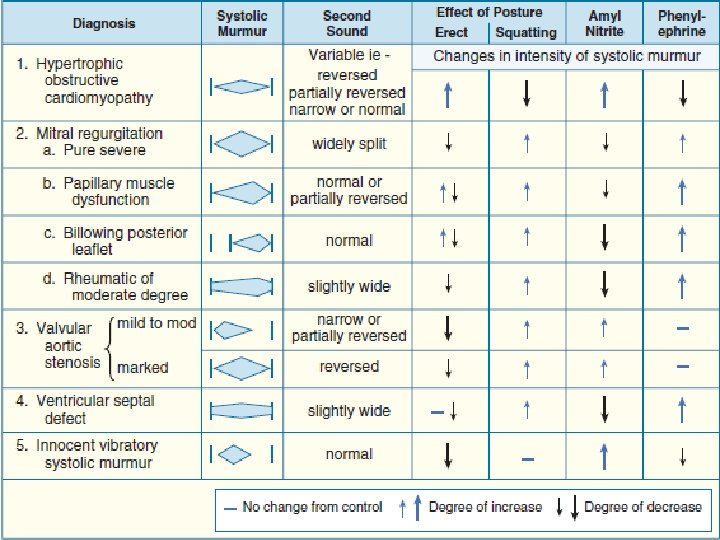
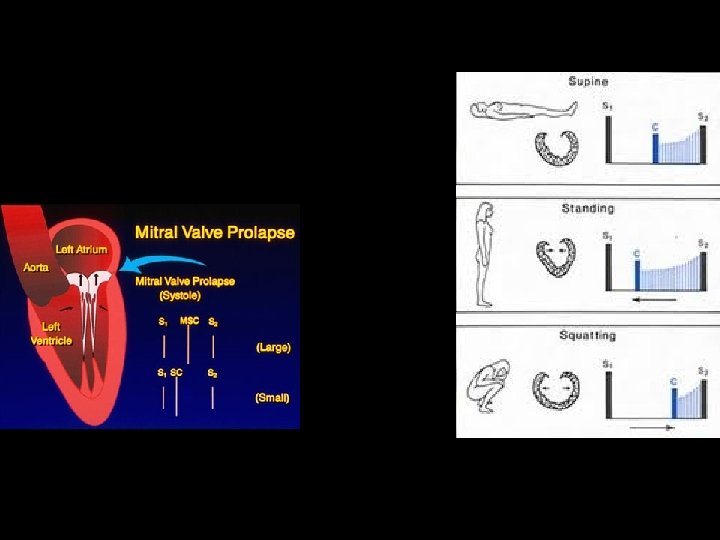
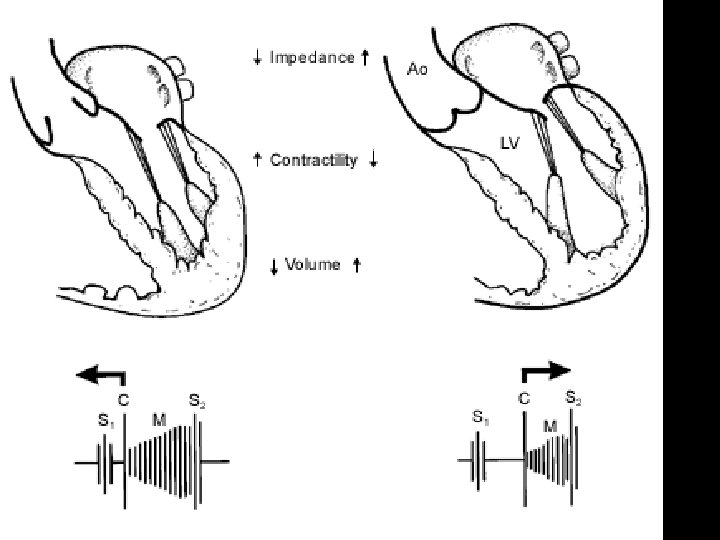
Abrupt standing • S 2 split which may be wide, may narrow down , while the fixed split may persist • A 2 OS interval widens – differentiates from wide split of S 2 • All murmurs ( except MVP/HOCM) decrease • ESM of HOCM becomes louder and longer • Click occurs earlier, murmur becomes longer in MVP – loudness shows variable response
Isometric Hand Grip HAND DYNAMOMETER
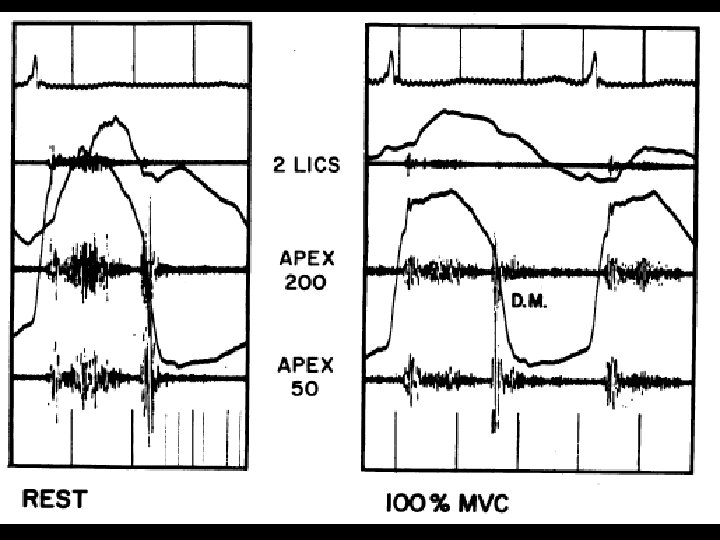
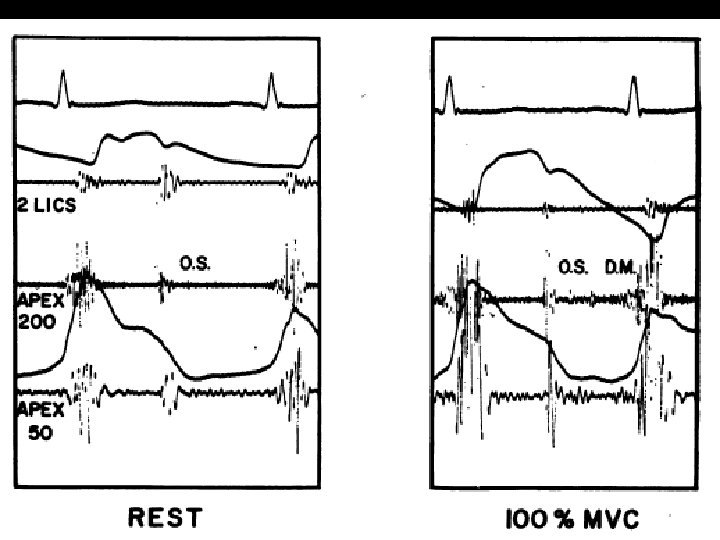
Physiological changes of ISOMETRIC HANDGRIP EXERCISE
Isometric Hand Grip Ø LV S 3 & S 4 get augmented Ø Murmurs of MR, AR, VSD intensify Ø Mitral stenotic murmur may augment Ø Systolic murmur of HOCM may diminish Ø Click & late sytolic murmur of MVP get delayed
Transient Arterial Occlusion
Squatting • Increased venous return and CO > augments most murmurs atleast initially (AS, PS, MR, AR, VSD) Right heart murmurs do so earlier • Increased ventricular volume > murmur of HOCM ↓ murmur of MVP ↓→ • Ejection murmur of TOF ↑
P Hanson Br Heart. J 7 1995; 74: 154
Central Aortic Pressure T Murakami AHJ 2002; 15: 986– 988
Hemodynamics of Squatting T Murakami AHJ 2002; 15: 986– 988
T Murakami AHJ 2002; 15: 986– 988
Valsalva Maneuver Decreased venous return & CO, HR ↑; PP↓ S 2 split narrows down, S 3 & S 4 diminish
Valsalva Maneuver • Reduces the intensity of all murmurs except that of HOCM & MVP • Murmur of HOCM intensifies as the LV cavity size decreases • Click occurs earlier, the murmur lengthens in MVP – may not intensify • During release, the intensity of right heart murmurs returns earlier - 1 to 3 vs 5 beats for left heart murmurs
VALSALVA STRAIN
ASD, HF, MS
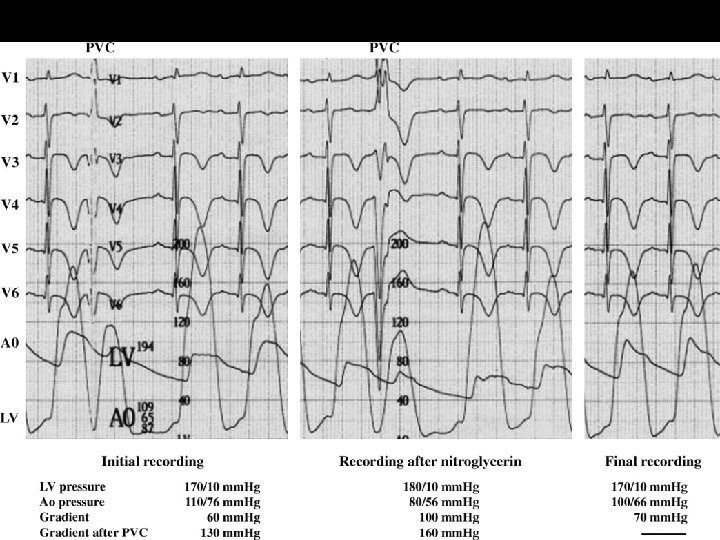
Cycle Length Variation Post premature beat / Long cycle short cycle of AF • Post VPD / Long > Short cycle of AF : Outflow murmurs ( AS/PS) accentuate Regurgitant murmurs do not change
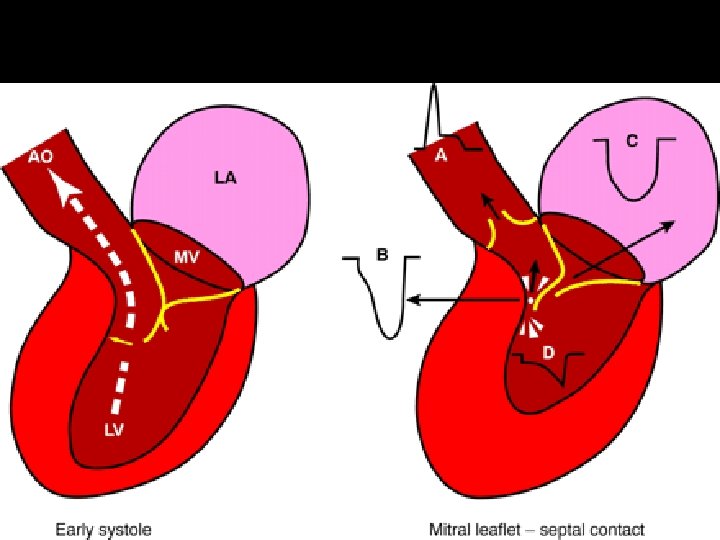
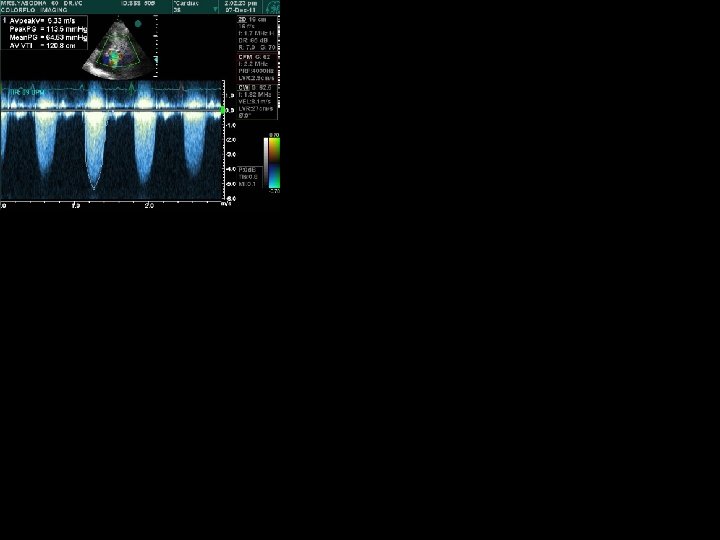
Aortic Stenosis HOCM
Amylnitrite Inhalation q < 30 secs : Systemic vasodilatation q 30 – 60 secs : ↑ HR & CO § Augments S 1, LV S 3 & S 4, TV & MV OS, murmurs of AS, PS, TR & HOCM § A 2 – OS may widen § Diminishes the murmurs of MR, AR, VSD, PDA & Systemic AVF § Click & Murmur of MVP occur earlier
Amyl Nitrite Inhalation Augments • • • Diminishes Aortic stenosis Mitral regurgitation Pulmonary stenosis TOF Tricuspid regurgitation Mitral stenosis Austin Flint Pulmonary regurgitation Aortic Regurgitaation
Phenylephrine v↑ BP & SVR ↓ CO & HR – last for 3 -5 mts • Reduces intensity of S 1, A 2 -OS may widen • Augments the murmurs of VSD, PDA, MR, AR, TOF, Systemic AVF • Diminishes AS, MS & functional murmurs • ESM of HOCM diminishes • Click & murmur of MVP get delayed
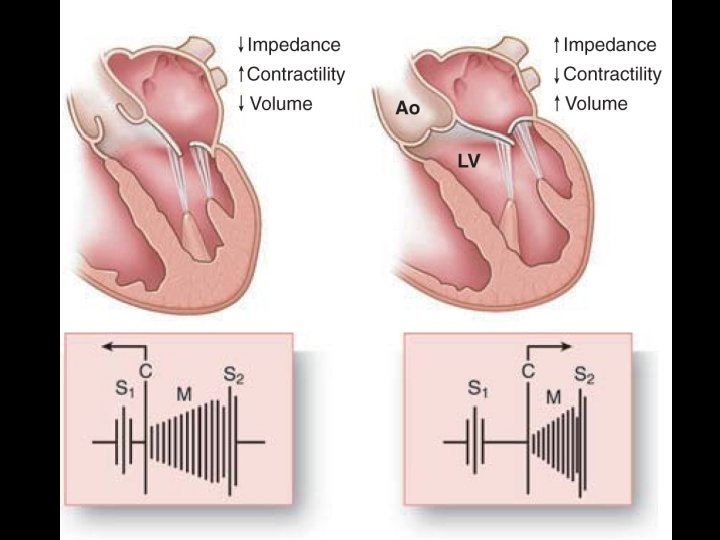
↑Afterload, ↑Preload, ↓Contractility ↓Afterload, ↓Preload, ↑Contractility
Valslava
the caveats are……… • Avoid dynamic auscultation in sick patients • When postures are changed, transition should be abrupt • Continuous auscultation is required, when maneuvres are being elicited • Concentrate on the first few cycles after maneuvres • Realize that each maneuvre induces more than one alterations in hemodynamics