Dual or Triple Antithrombotic Therapy for Patients with

Dual or Triple Antithrombotic Therapy for Patients with ACS and AFib? Jorge F. Saucedo, MD, MBA Division Chief of Cardiovascular Medicine Professor of Medicine Medical College of Wisconsin Director of the Heart & Vascular Service Line Froedtert Health System

Dual or Triple Antithrombotic Therapy for Patients with ACS and AFib? • Triple antithrombotic therapy with warfarin plus DAPT has been the standard of care after PCI for patients with AFib • Triple therapy is associated with a high risk of bleeding. • Need to balance risks of ischemic stroke and thromboembolism, recurrent cardiac ischemia and/or stent thrombosis, and bleeding and hemorrhagic stroke. • Promising approaches to reduce bleeding include using a NOAC and omission of ASA

Incidence Rates per 100 Person-Years of Major Bleeds by Age and Use of Antithrombotic Agents

Incidence Rates per 100 Person-Years of Major Bleeds by CHA 2 DS 2 -VASC and Use of Antithrombotic Agents

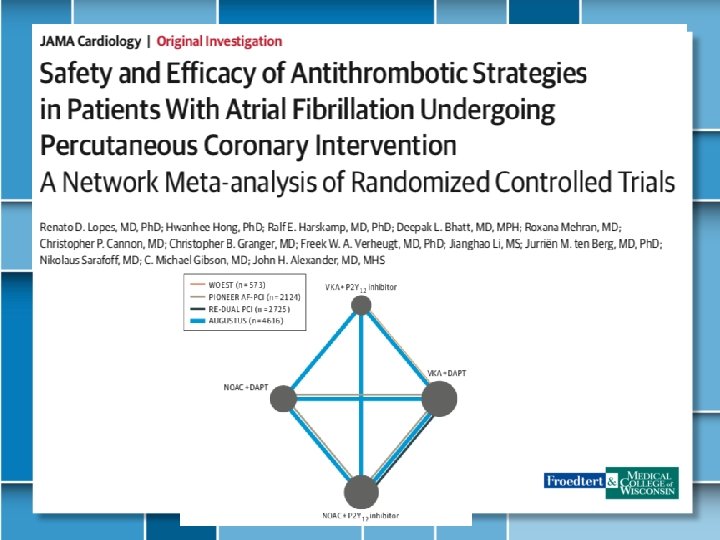
Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial Open-label, multicenter, randomised, controlled trial in 15 centers 573 patients for 279 (98· 2%) patients assigned double therapy and 284 assigned triple therapy.

Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation 2725 pts with atrial fibrillation + PCI to triple therapy with warfarin (clopidogrel or ticagrelor) and aspirin (for 1 to 3 months) (triple-therapy group) or dual therapy with dabigatran (110 mg or 150 mg twice daily) plus a P 2 Y 12 inhibitor.

Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI 2124 atrial fibrillation + PCI with stenting to receive, in a 1: 1: 1 ratio, lowdose rivaroxaban (15 mg once daily) plus a P 2 Y inhibitor for 12 months verylow-dose rivaroxaban (2. 5 mg plus DAPT for 1, 6, or 12 months or standard therapy with a dose- adjusted vitamin K antagonist (once daily) plus DAPT for 1, 6, or 12 months
 – Physician decision")
Augustus Trial Design INCLUSION • Atrial fibrillation (prior, persistent, >6 hr) – Physician decision for OAC • Acute coronary syndrome or PCI – Planned P 2 Y 12 inhibitor for ≥ 6 months Apixaban 5 mg BID Apixaban 2. 5 mg BID in selected patients Randomize n=4600 patients EXCLUSION • Contraindication to DAPT • Other reason for VKA (prosthetic valve, moderate / severe mitral stenosis) Open Label VKA (INR 2– 3) Aspirin for all on the day of ACS or PCI Aspirin versus placebo after randomization Aspirin Double Blind Placebo Primary outcome: ISTH major / CRNM bleeding Secondary outcome(s): death / hospitalization, death / ischemic events Lopes RD, et al. Am Heart J. 2018; 200: 17 -23.
 Age, median (25 th, 75 th), years Female, %")
AUGUSTUS Baseline Characteristics Total (N=4614) Age, median (25 th, 75 th), years Female, % CHA 2 DS 2 -VASc score, mean (SD) HAS-BLED score, mean (SD) Prior OAC, % P 2 Y 12 inhibitor, % Clopidogrel Prasugrel Ticagrelor Number of days from ACS/PCI to randomization, mean (SD) Qualifying index event, % ACS and PCI ACS and no PCI Elective PCI 70. 7 (64. 2, 77. 2) 29. 0 3. 9 (1. 6) 2. 9 (0. 9) 49. 0 92. 6 1. 1 6. 2 6. 6 (4. 2) 37. 3 23. 9 38. 8

AUGUSTUS Major / CRNM Bleeding Apixaban vs. VKA HR 0. 69, 95% CI 0. 58– 0. 81 P<0. 001 for non-inferiority P<0. 001 for superiority ARR=4. 2% NNT=24 VKA: 14. 7% Apixaban: 10. 5% ARR: absolute risk reduction NNT: number needed to treat

AUGUSTUS Major / CRNM Bleeding Aspirin vs. Placebo HR 1. 89, 95% CI 1. 59– 2. 24 P<0. 001 ARI=7. 1% NNH=14 Aspirin: 16. 1% Placebo: 9. 0% ARI: absolute risk increase NNH: number needed to harm
 Apixaban + Aspirin (13.")
AUGUSTUS Major / CRNM Bleeding VKA + Aspirin (18. 7%) Apixaban + Aspirin (13. 8%) VKA + Placebo (10. 9%) Apixaban + Placebo (7. 3%) Apixaban + Placebo vs. VKA + Aspirin: 11. 4% absolute risk reduction (NNT=9)
 VKA + Placebo (27. 3%)")
AUGUSTUS Death / Hospitalization VKA + Aspirin (27. 5%) VKA + Placebo (27. 3%) Apixaban + Aspirin (24. 9%) Apixaban + Placebo (22. 0%) Apixaban + Placebo vs. VKA + Aspirin: 5. 5% absolute risk reduction (NNT=18)

TIMI Major or Minor Bleed

Dual Vs Triple Antithrombotic Therapy All Cause Mortality Cardiac Death Golwala H, et al Eur Heart J (2018) 39, 1726 Golwala H, et al. Eur Heart J (2018) 39, 1726– 1735

Bleeding and Ischemic Risk for Dual Vs Triple Antithrombotic Therapy Golwala H, et al. Eur Heart J (2018) 39, 1726– 1735

Triple Vs. Dual Therapy Safety Outcomes TIMI major bleeding Trial Defined Primary Safety Outcome TIMI major and minor bleeding Intracranial Hemorrhage

Triple Vs. Dual Therapy Efficacy Outcomes Trial Defined Primary MACE Cardiovascular Death All Cause Death Myocardial Infarction

Triple Vs. Dual Therapy Safety and Efficacy Outcomes Odds Ratios for TIMI Major Bleeding and MACE

Conclusions • Dual Therapy is safe and effective in patients with AFib undergoing PCI and should be therapy of choice • NOAC + P 2 Y 12 appears to be the best combination • Questions – – Which NOAC? What Dose? Cost-effective? Which P 2 Y 12? Which is the ideal combination? Is there a role for short term triple therapy in high risk patients?
- Slides: 21