DRUGS AFFECTING the CENTRAL NERVOUS SYSTEM Module 1


 depress the CNS to permit the surgery operations and unpleasant procedures.")

 anesthetics: 1. Short acting (ad 15 minutes) Ketamine is an arylcyclohexylamine.")

 Three derivatives of barbituric acid are used for")
 Sodium oxybate (Sodium oxybutyrate) Sodium oxybutyrate has")













 ● ● ● μ-OR of the central nervous")
")
 – is the")




 when the drug is administered")






 Non-narcotic analgesics block COX and inhibit")
 -the first representative of non-narcotic analgesics. The drug is used")
 shows a pronounced analgesic, anti-inflammatory and")
 in the chemical structure is a metabolite")

 shows a pronounced anti-inflammatory, analgesic and antipyretic effect, caused by blockade of")



- Slides: 45
DRUGS AFFECTING the CENTRAL NERVOUS SYSTEM Module 1
TH 1. Drugs affecting the CNS. ● Drugs for general anesthesia: ○ ○ Non-inhalational (intravenous, parenteral) anesthetics Inhalational anesthetics ● Ethyl alcohol ● Hypnotic drugs. Antiepileptic and antiparkinsonism drugs. ● Analgesics (opioid, non-opioid) ● Antipsychotics (Neuroleptics) ● Anxiolytics (Tranquilizers) ● Sedative drugs ● Antidepressants ● Psychomotor stimulants ● Nootropics (Cognitive Enhancers) ● Adaptogens, Actoprotectors
General anesthetics (GAs) depress the CNS to permit the surgery operations and unpleasant procedures. General anesthesia is a reversible depression of CNS function with the loss of response and perception of all external stimuli. The features of the use of General anesthetics are: ● Decrease in systemic arterial blood pressure due to vasodilatation, myocardial depression, blunting of baroreceptor control, reduction in central sympathetic tone. ● Reduction or elimination ventilatory drive and reflexes that maintain airway patency. ● Loss of passive and active regurgitation due to the loss of gag reflex and cough reflex, and decrease of lower esophageal sphincter tone. ● During surgery the hypothermiais is developed in patients as a result of low environment temperature, exposed body cavities, cold intravenous fluids, altered termoregulatory control, reduced metabolic rate. ● Peripheral vasoconstriction is activated to defend against heat loss. Total body oxygen consumption is decreased by 30%. ● Nausea and vomiting in the post-operative period are caused by an action of general anesthetics on chemoreceptor trigger zone and brainstem vomiting center, which are modulated by serotonin, histamine, acetylcholine, and dopamine.
Classification of General Anaesthetics: I. Inhaled Anaesthetics: · · · 1. Fluid Volatile agents: Aether pro narcosi Phthorothanum (Halothanum) Isofluran Eufluran 2. Casiform agents: Nitrogenium oxydulatum II. Intravenous (non-inhaled) general anaesthetics: 1. Short acting (ad 15 min. ): · Propanidid · Ketamin 2. Medium acting (20 -30 min. ) · Thiopentalum-natrium (Pentothalum) · Hexenalum 3. Long-acting: · Natrii oxybutiras
Non-inhalational (intravenous, parenteral) anesthetics: 1. Short acting (ad 15 minutes) Ketamine is an arylcyclohexylamine. Ketamine is typically administrated intravenously but may be introduced intramuscularly, oraly and rectaly. It is metabolized in the liver and is excreted with the bile and urine. In case of intravenous introduction of ketamine the onset of anesthesia after single bolus is 20 -60 seconds and the duration of anesthesia is 5 -10 minutes. The drug increases the heart rate, cardiac output and blood pressure which is due to sympathetic stimulation. Respiration is not depressed, muscle tone increases and reflexes are not abolished during anaesthesia. Ketamine has been recommended for short operations, unpleasant therapeutic and diagnostic procedures in children, operation in shocked patients and in obstetrics. Adverse reactions include delirium, hallucinations and unpleasant dreams. It should not be used in hypertensive cases and to patients with ischaemic heart disease.
Propanidid is a propyl ester of phenylacetic acid. In case of its intravenous single bolus onset of anesthesia arises in 20 -40 seconds without stage of excitement and lasts 4 -10 minutes. In human body Propanidid rapidly is hydrolyzed by plasma cholinesterase. Propanidid is excreted by kidney and is not accumulated. Side effects of Propanidid: spontaneous limb movements, tremor; slight decrease in general blood pressure, tachycardia; laryngeal spasm; transient tachypnea, followed by a brief apnea; nausea, vomiting, headache, salivation, phlebitis, thrombophlebitis, and anaphylactic shock due to its ability to increase histamine release. Propanidid is suited the best for the short painful procedures, examinations, reposition of bone fragments, and removal of stitches. Contraindications for Propanidid use: kidney and liver insufficiency, shock
2. Medium acting (20 -30 minutes) Three derivatives of barbituric acid are used for general anesthesia the most widely. There are sodium thiopental, thiamylal, and methohexital. Sodium thiopental is most frequently used for inducing anesthesia and does not elicit pain on injection, but has anti-analgesics effect and reduces the pain threshold. Thiopental has been used as a protectant against cerebral ischemia, but for this purpose the large doses are required that elicits prolonged sedation and limits such use. Thiopental is effective in case of status epilepticus. Sodium thiopental in single induction may elicit mild transient depression of newborn activity. Thiopental does induce precipitation of neuromuscular blockers or other drugs during anesthetic induction.
3. Long acting ( over 30 minutes) Sodium oxybate (Sodium oxybutyrate) Sodium oxybutyrate has a sedative, anxiolytic, antihypoxic, myorelaxant effect, and mild analgesic effect. Sodium oxybutyrate is excreted basically by the lungs as carbon dioxide. Sodium oxybutyrate can be used intravenously and peroral for general anesthesia. The basic place of its action is tissue metabolism, first of all – the carbohydrate metabolism. Overdose may depress respiratory center. Sodium oxybutirate can be used for the induction and basic anesthesia in case of labor pains, brain hypoxia and shock. The stage of surgical anesthesia occurs 30 -40 minutes after intravenous administration and lasts 1. 5 -3 hours. Analgesic effect is not expressed, relaxes the skeletal muscles. Sometimes develops hypokalemia, vomiting is possible.
Inhaled Anaesthetics Ether for anesthesia is the volatile highly flammable liquid, dangerously explosive. Advantages of Ether for anesthesia are: the large latitude of therapeutic action, rapid recovery from anesthesia, and simple control of the depth of anesthesia. The main place of its distribution is the brain. The ether for anesthesia is mainly eliminated by the lungs in an unchanged form and the remains of it are eliminated by kidney, skin and GIT. The ether for anesthesia has analgesic effect, which is saved in after recovery from anesthesia; depresses of the cortex activity; it does not influences blood pressure, increases the heart rate; causes myocardial depression, but produces epinephrine and norepinephrine release, it does not change sensitivity of myocardium to catecholamines; the ether for anesthesia does not damage internal organs; it has myorelaxant effect, improves the action of neuromuscular blockers. The disadvantages of ether for anesthesia are long-term introduction of anesthesia with a severest phase of excitation due to induction of subcortical activity and depression of cortex activity; irritation of the mucous membranes that cause inflammatory process in respiratory ways, vomiting; it depresses the renal function and may provoke proteinurua; ether for anesthesia may elicit acidosis, ketonemia. Premedication by atropine.
Halothane is the volatile liquid at the room temperature and it must be stored in a sealed container. Halothane and its mixtures with air or oxygen are neither flammable nor explosive. About 80% of halothane is eliminated by lungs in unchanged form in the first 24 hours, and remainder of it is biotransformed by hepatic enzymes. Halothane does not irritate the respiratory tract; it diminishes bronchial secretion and causes bronchodilatation, inhibits both laryngeal and swallowing reflexes, reduces salivation, relaxes masticatory muscles, and accelerates the rate of breathing. The analgesic effect of halothane is weak. Bronchodilatory properties of halothane are allowed to use it in patients with status asthmaticus as a last resort. Due to uterine smooth muscle relaxation effect of halothane, it is used for manipulation of the fetus (version) in the prenatal period and for delivery of retained placenta postnatally. Halothane can provoke specific fatal syndrome with malignant hyperthermia, severe muscle contraction, and increase in metabolic rate in genetically sensitive patients.
Isoflurane is halogenated inhalation anesthetic similar to halothane for most of the pharmacokinetic and pharmacodynamic parameters. About 99% of inhaled isoflurane is eliminated by the lungs in unchanged form; the remainder of it is metabolized in liver. Isoflurane is typically used for maintenance of anesthesia after induction of other agents. Isoflurane is safe anesthetic for the patients with ischemic heart disease. If it is used together with opioids or nitrous oxide isoflurane concentration may be reduced. Side effects of isoflurane: decrease in general blood pressure due to the decreased systemic vascular resistance, vasodilatation without reduction of cardiac output; isoflurane improves cardiac blood flow and decreases myocardial oxygen consumption. Isoflurane reversibly reduces renal blood flow and glomerular filtration; splanchnic and hepatic blood flow is reduced according elevated doses of isoflurane as systemic arterial pressure decreases. Isoflurane is not recommended for analgesia or anesthesia for labor and vaginal delivery.
Sevoflurane is a widely used anesthetic for outpatient, especially for children, due to the rapid recovery profile and due to the absence irritant effect on the airways. Sevoflurane is a preferable agent in patients who are inclined to myocardial ischemia because it does not provoke tachycardia. The greater part of absorbed sevoflurane is excreted in unchanged form and insignificant part of it is metabolized in the liver. Side effects of sevoflurane: a concentration-dependent decrease in arterial blood pressure, systemic vasodilatation, a concentration-dependent decrease in cardiac output; a concentration -dependent reduction in tidal volume and increase in respiratory rate, and an increase in partial pressure of carbon dioxide in the blood, sevoflurane like other inhalational agents is bronchodilatator; its cerebral vasodilatation is less than of isoflurane and desflurane, an increase in intracranial pressure, delirium in children; skeletal muscle relaxation; and it improves the effects of non-depolarizing and depolarizing neuromuscular blocking agents like other inhalational anesthetics; transient renal injury.
Nitrous oxide is very insoluble in blood and other tissues; as a result it provides rapid equilibration between delivered and alveolar anesthetic concentration, rapid induction of anesthesia and rapid anesthesia recovery. Nitrous oxide is eliminated in unchanged form by the lungs and with minimal diffusion through the skin. Nitrous oxide can oxidize cobalt form of vitamin B 12 to cobalt, thereby inhibiting methionine synthetase and synthesis of methionine, DNA, RNA, myelin, and it can produce vitamin B 12 deficiency, megaloblastic anemia, and peripheral neuropathy. That's why nitrous oxide is not used in patients with vitamin B 12 deficiency, anemia, chronic alcoholism, malnutrition, and it is not used as chronic analgesic although nitrous oxide has a significant analgesic effect or as a sedative agent. Side effects of nitrous oxide: stimulatory effects on sympathetic nervous system; the cardiovascular effects of nitrous oxide are dependent on concomitant administration with other anesthetic agents, an increase in venous tone of both the peripheral and pulmonary vasculature; an increase in respiratory rate and a decrease in tidal volume, depression in ventilatory response to hypoxia; an increase in cerebral blood flow and intracranial pressure.
Nitrous oxide has two “problems”: Firstly: on discontinuation of nitrous oxide administration, nitrous oxide gas can diffuse from blood to the alveoli, diluting oxygen in the lungs and provoke an effect called diffusional hypoxia. In order to prevent diffusional hypoxia, 100% oxygen rather than air should be administered after the cessation of supply of nitrous oxide for 4 -5 minutes. Secondly: nitrous oxide can exchange with nitrogen in any air-containing cavity in the human body. Furthermore, nitrous oxide can enter the cavity faster than nitrogen escapes, and therefore increasing the volume and pressure in this cavity. Thereby, nitrous oxide can expande a Pneumothorax, an obstructed middle ear, an aire embolus, an obstructed loop of bowel, an intraocular air bubble, a pulmonary bulla, and intracranial air. As a result, nitrous oxide cannot be used in these clinical setting.
Xenon is an inert gas. It has minimal cardiorespiratory side effects, has analgesic and anesthetic effects due to influences on receptors and potassium channels in the CNS. At the same time, xenon is a rare gas and must be extracted from air and cannot be manufactured. This renders xenon very expensive. Its use is limited. Xenon is extremely insoluble in blood and other tissues, provides rapid induction of anesthesia and rapid anesthesia recovery. Xenon is well tolerated in the patients of advanced age. Side effects of xenon: a slight decrease in respiratory rate, an increase in tidal volume, minimal respiratory depression; reduction in cerebral metabolism and cerebral blood flow.
Ethyl alcohol at the local application gives a pronounced antiseptic, as well as irritating and astringent effect. The absorption of the drug is manifested by the inhibition of the central nervous system, which is the cause of acute and chronic poisoning when using alcoholic beverages. Ethyl alcohol, when used internally, is rapidly absorbed (especially onset) mainly in the small intestine and about 20% in the stomach. In the body, 90% of ethyl alcohol is biotransformed to carbon dioxide and water. Oxidized in the liver with energy release (7. 1 kcal / g). The ethyl alcohol in the unchanged form is excreted by the lungs, kidneys and sweat glands. The suppressive effect of ethyl alcohol, depending on the concentration in the blood and brain tissues, has 3 stages: - excitation; - anesthesia; - agonal.
Application of resorptive action of ethyl alcohol: - parenteral feeding of patients with cachexia, which are in critical condition. A 5% solution of ethanol is added to antishock liquids; - when poisoned with methyl alcohol injected intravenously in the form of 10% solution; - termination of preterm labor. As a result of prolonged use, you can get used to and addiction (mental and physical). Acute alcohol poisoning with ethyl alcohol occurs at its concentration of 3 -4 g / l and is characterized by signs of profound inhibition of CNS function. The stage of euphoria and agitation changes the coma. Victims lose consciousness, body temperature decreases, skin becomes wet, cold to the touch, frequent pulse, weakness, asphyxia, cyanosis, cardiac activity, possible seizures, delusions, involuntary urine and feces. Death comes from paralysis of the respiratory center and a decrease in cardiac activity
During the treatment of acute poisoning with ethyl alcohol: - to prevent the cessation of breathing and aspiration by emesis; - to prescribe the function of the cardiovascular system to prescribe cardiac glycosides; - if preserved renal function, carry out forced diuresis with furosemide; - inject drugs: sodium bicarbonate (to eliminate acidosis), glucose with insulin (for oxidation of alcohol), etc. Chronic poisoning (alcoholism) is characterized by addiction, mental and physical dependence, syndrome of abstinence. Among the pharmacological agents for the treatment of patients with alcohol, teturetics (disulfiram, antabus) are effective. The essence of the treatment is that in the case of the appointment of tetrama together with 20 -30 ml of vodka disturbed oxidation of alcohol at the level of acetaldehyde, the patient observed hyperemia of the face, arterial hypotension, tachycardia, increased sweating, respiratory failure, vomiting, fear of death. This can take from 30 minutes to several hours. Thus, the patient is disgusted with alcohol.
Analgesics
Opioid analgesic ● ● Alkaloids of opium - morphine, codeine, omniphone. Synthetic substitutes for morphine: ethylmorphine hydrochloride, promedol, fentanyl, sufentanil, methadone, dipidolor (pyrithamide), estocin, pentazocine, tramadol (tramal), butorphanol (modalol), buprenorphine, thilidine (valoron). Non-opioid analgesics (non steroid anti-inflammatory drugs – NSAIDs) ● Salicylates - acetylsalicylic acid, acelysin (aspirin), sodium salicylate. ● Derivatives of pyrazolone and indoleacetic acid - indomethacin (metinodole), butadione, analgin (metamizole sodium) ● Derivatives of paraaminophenol paracetamol (panadol, lecadol) ● Derivatives of alkanic acids - ibuprofen, diclofenac sodium (voltran, ortofen), naproxen (naproxin) ● Combined drugs - reopyrin, sedalgin, tempalgin, baralgin, tsitramon, tsitropak, tsilopak, akstrin, paravit.
Types of pain • Surface epicritic pain, short-term and acute (occurs in the case of irritation of nuciceptors of the skin, mucous membranes). • Pelvic pain that has different durations and ability to spread to other areas (occurs when irritation of the nociceptors located in the muscles, joints, periosteum). • Visceral pain occurs during irritation of the painful receptors of the internal organs - the abdominal cavity, pleura, vascular endothelium, and the membranes of the brain. The antinociceptive system violates the perception of pain, pain and impulse formation. The structure of this system includes endorphins, which are produced in the pituitary gland, the hypothalamus, and enter the bloodstream. their allocation increases with stress, during pregnancy, during labor, under the influence of diazate, oxide, fluorothane, ethanol and depends on the state of the higher nervous system (positive emotions). In the case of a nociceptive system failure (with excessive pronounced and prolonged damage), pain is suppressed by analgesics.
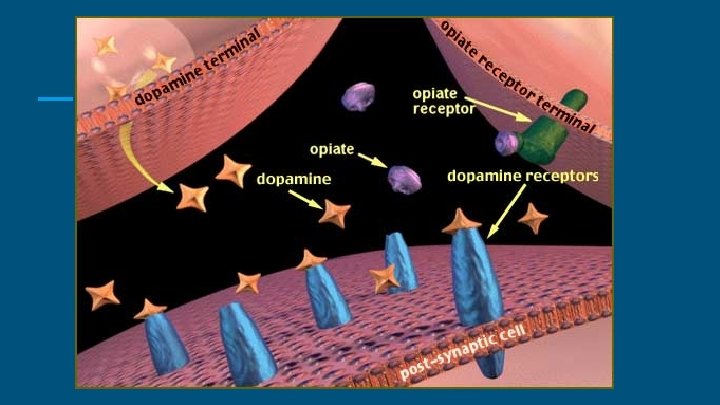
Opioid receptors: ● μ-OR (OPRM 1) ● ● ● μ-OR of the central nervous system is predominantly involved in the modulation of pain sensitivity, their activation causes respiratory depression and the development of bradycardia. δ-OR (OPRD 1) δ-OR mainly regulate the psycho-emotional sphere, their agonists can cause antidepressant and anxiolytic effects. κ-OR (OPRK 1) With the activation of κ-OR linked a sedative effect. In 1995, two independent groups of scientists discovered that there was a special fourth class of opioid receptors involved in the regulation of pain sensitivity, as well as their specific agonist. Some researchers called it nociceptum, while others were dubbed "orphanin. FQ" as an "orphan". These names are still preserved, and the receptor is called the nociceptin-orphan (NOR) receptor. Thus, at present, several subtypes of opiate receptors involved in anti-nociception mechanisms are known. With the activation of these receptors, the mechanism of the soothing effect of opiates is associated.
Opioid analgesics III. Synthetic compounds: I. Natural alkaloids: ● ● Morphine (as sulphate; MORCONTIN) Codeine (as phosphate) II. Semisynthetic compounds: ● ● Pholcodeine (ETHNINE) Diacetyl morphine (HEROIN) Other semisynthetic agents are hydromorphone, oxycodone, hydrocodone, dihydrocodeine etc. ● ● ● Pethidine (as hydrochloride) Fentanyl (as citrate; FENDROP) IM/IV Methadone (PYSEPTONE) Dextropropoxyphene (DEXOVON) Tramadol (TRANDOL) Ethoheptazine (EQUAGESIC)
Opioid analgesics I. Agonists ● ● ● Morphine Fentanyl Omnoponum (Papaveretum) – is the mixture of hydrochloride salts of opium alkaloids Trimeperidine (Promedolum) Codeine II. Agonists-antagonists ● ● Buprenorphine Butorphanol Nalbuphine Nalorphine III. Antagonists ● ● Naloxone Naltrexone
Pharmacological effects: central: ● ● ● ● ● analgesia; respiratory depression (degree depends on the dose of opioids); Inhibition of cough reflex; sedative effect; hypnotic effect; euphoria - the disappearance of unpleasant emotions, a sense of fear and tension; nausea and vomiting as a consequence of the activation of the d opamine receptor trigger-zone (occurring in 20 -40% of patients in response to the first injection of opioids); increase of spinal reflexes (knee, etc. ); myositis (narrowing of the pupils) - as a result of increased tonus of the nucleus of the oculomotor center; peripheral: ● ● obturational effect associated with spastic contractions of sphincter, restriction of peristalsis; bradycardia and arterial hypotension caused by increased tone of the nucleus of the vagus nerve; increased tonus of smooth muscle of the bladder and ureter sphincter (there may be renal colic and urinary retention, which are undesirable in the postoperative period); hypothermia (therefore the patient should be warmed up and often change the position of the body in bed).
MORPHINI HYDROCHLORIDUM
MORPHINI HYDROCHLORIDUM Morphine is rapidly absorbed when used internally and with subcutaneous administration. The action comes 10 -15 minutes after (subcutaneous administration) and after 20 -30 minutes after (oral administration) and lasts 3 -5 hours. Well penetrates through the GEB and the placenta. Biotransformation occurs in the liver, excreted in the urine. Indications for use: as an analgesic for myocardial infarction, in the pre-and postoperative period, in traumas, oncological diseases. Appoint subcutaneously, as well as inwards in powders or drops. Can’t be prescribed for children under the age of 2 years.
● ● ● Acute OA poisoning: euphoria; anxiety; dry mouth; a feeling of heat; dizziness, headache; drowsiness; urges to urinate; comatose condition; myosum, which is replaced by mydriasis; rare (up to five respiratory movements per minute), superficial breathing; blood pressure dropped. ● ● ● HELP: gastric lavage irrespective of the method of administration of 0. 050. 1% solution of potassium permanganate; 20 -30 g activated charcoal; salt washing; intravenous and intramuscular administration of antagonist naloxone. The drug acts quickly (1 min), but shortlived (2 -4 hours). For prolonged action, intravenous must be administered nalmefen (10 hours); there may be a need for artificial respiration; warm the patient.
Tolerance is detected in 2 -3 weeks (sometimes earlier) when the drug is administered in therapeutic doses. After stopping the use of opioid analgesics, euphoric tolerance and respiratory depression decrease after several days. Mental dependence - the euphoria that occurs when using narcotic analgesics and is the root cause of uncontrolled use of drugs, especially in adolescents. Physical dependence is associated with abstinence syndrome (withdrawal syndrome): tearing, hyperthermia, sudden changes in blood pressure, muscle and joint pain, nausea, diarrhea, insomnia, hallucinations. Constant use of opioids leads to chronic poisoning, which reduces mental and physical performance, there is exhaustion, thirst, sting, hair loss, etc.
Codeine phosphate Anesthetizing activity is due to the excitation of opiate receptors in various departments of the central nervous system and peripheral tissues, leading to stimulation of antinociceptive system and changes in emotional perception of pain. The central antitussive effect is associated with suppression of the cough center at the "bridge" level. The activation of opiate receptors in the intestine causes relaxation of smooth muscles, reduction of peristalsis and spasm of all sphincters. After ingestion, it is rapidly absorbed. Binding to plasma proteins is insignificant. It undergoes biotransformation in the liver, with 10% by demethylation being converted into morphine. T 1 / 2 is 2. 5 -4 hours. Excreted by the kidneys: 5 -15% in the form of codeine and 10% in the form of morphine and its metabolites. The analgesic effect develops after 10 -30 minutes after v / m and n / k and 30 -60 minutes after the enteral administration. The maximum effect is achieved 30 -60 minutes after intravenous administration and 1 -2 hours after enteral administration. The duration of analgesia is 4 hours, the blockade of the cough reflex is 4 -6 hours.
Omnopon contains a mixture of opium alkaloids, including 48 -50% morphine and 32 -35% other alkaloids. The drug inferior to the analgesic effect of morphine and gives an antispasmodic effect (contains papaverine). Apply in such cases as morphine, but Omnopon is more effective in spastic pain. Introduce subcutaneously. Promedol - a synthetic analgesic. By analgesic action inferior to morphine in 2 -4 times. Duration is 3 -4 hours. Rarely than morphine, causes nausea and vomiting, to a lesser extent suppresses the center of respiration. Reduces the tonus of smooth muscles of the urinary tract and bronchi, increases the tone of the intestines and bile ducts. Strengthens the rhythmic contractions of myometrium. Fentanyl is a synthetic drug that surpasses the analgesic action of morphine in 100 -400 times. After intravenous administration, the maximum effect is observed in 1 -3 minutes, which lasts 15 -30 minutes. Fentanyl causes pronounced (up to the stopping of breathing), but prolonged inhibition of the respiratory center. Increases the tone of skeletal muscle. Often there is bradycardia.
Tramadol is centrally acting synthetic analgesic compound. It acts via opioid receptors in CNS to produce analgesia and has no abuse potential. It also inhibits the reuptake of noradrenaline and serotonin. It causes less respiratory depression, sedation, constipation and urinary retention than morphine. Its hemodynamic effects are minimal. Side effects include nausea, vomiting and dizziness. It is indicated in moderate to severe, acute or chronic pain and in painful diagnostic procedures and surgery; arthralgia, dental pain, musculoskeletal pain, pain associated with fractures, dislocation and other related type of pain. Pentazocine agonist-antagonist of morphine and is used as an analgesic. It exerts morphine like action. It is a partial agonist at opioid receptors and is effective in mild to moderate type of pain associated with surgery, trauma, burns, colics, toothache, cancer, in labour and as preanaesthetic medication. It is kappa receptor agonist with weak mu antagonist or partial antagonist properties. It causes tachycardia and rise in BP due to sympathetic stimulation. Tolerance and dependence develops on repeated use. It is effective orally. It is oxidized and glucuronide conjugation occurs in liver and excreted in urine.
Nalorphine an N-allylnormorphine, semisynthetic congener of morphine. The agonistic actions are produced by kappa receptor activation and antagonistic properties are due to action on mu receptor which antagonizes all morphine actions (mainly reverses the analgesia and respiratory depression). It is used mainly in the treatment of acute morphine poisoning. Nalbuphine is a strong kappa receptor agonist and mu receptor antagonist. Its agonistic property is approximately three to four times more than pentazocine and its antagonistic property is approximately 10 times more than pentazocine. It has less abuse liability in comparison to pentazocine. It is useful in postoperative pain, myocardial infarction and labour. Buprenorphine It is a potent and long acting opioid with partial mu receptor agonist property. 25 times more potent than morphine. Effects are similar to morphine but constipation is less marked. It undergoes extensive presystemic elimination and therefore is given by parenteral route. It is excreted unchanged in urine. Side effects include dizziness, sedation, miosis, respiratory depression, sweating and vomiting. It is indicated in moderate to severe pain, premedication to surgery, pain due to myocardial infarction and in postoperative pain.
Butorphanol is a kappa agonist. It produces analgesia equivalent to nalbuphine and buprenorphine but produces more sedation. It is used in postoperative pain and renal colic pain. Naloxone is N-allyl analogue of oxymorphone, have a high affinity for mu receptor and lower affinity at delta and kappa sites. It selectively antagonizes the respiratory depression produced by opioids. After intravenous administration, it antagonizes all actions of morphine. It also blocks the actions of endogenous opioid peptides. It is inactive orally because of high first pass metabolism in liver. Metabolised by glucuronidation in liver. The main use of naloxone is in the treatment of acute opioid overdose (acute morphine poisoning). The constricted pupils of addicts dilate after administration of naloxone. This has been used as a diagnostic tool for opioid addiction. Naltrexone is a pure antagonist and chemically related to naloxone. It is more potent than naloxone and because of its longer duration of action, it can be used as maintenance drug for morphine addicts. It has no euphoric effect and no physical dependence liability. It is effective orally. It is also claimed to be beneficial in decreasing craving for alcohol in alcoholics. Side effects include gastrointestinal disturbances and muscular pain.
Pharmacosafety: ● narcotic analgesics are poisonous drugs in List A, they should be prescribed on special forms, they are subject to quantitative accounting. Issue and storage of regulated; ● for misuse, misuse of purpose - criminal liability; ● morphine is not compatible in one syringe with aminazine; ● promedol is not compatible with antihistamines; ● the injection form of tramadol is incompatible with solutions diazepam, flunitrosenam, nitroglycerin; ● pentazocine with barbiturates can not be administered in one syringe; ● drugs opium inhibit peristalsis of the intestines and may delay the absorption of other drugs that are prescribed inside; ● codeine as a part of complex drugs practically does not cause euphoria and addiction.
Non-opioid analgesics (nonsteroid anti- inflammatory drugs – NSAIDs) Non-narcotic analgesics block COX and inhibit the formation of prostaglandins, which causes anti-inflammatory, antipyretic and analgesic effects. The anti-inflammatory effect is that the exudative and proliferative phases of inflammation are limited. The effect is observed in a few days. The analgesic effect is observed after several hours. Drugs affect mainly on pain in inflammatory processes. The antipyretic effect is manifested in hyperpyrexia in a few hours. At the same time, heat transfer is increased due to the expansion of peripheral vessels and increased sweating. Reducing body temperature to 38 ° C is not feasible because subfebrile temperature is a protective reaction of the organism (increased activity of phagocytes and products of interferon, etc. ).
Salicylates Acid acetylsalicylic (aspirin) -the first representative of non-narcotic analgesics. The drug is used since 1889. It’s available in tablets, is a part of such combined preparations, as citramon, sedalgin, koficil, alka-zeltser, aspirin, tomapyrin. Indications for use: as analgesic and antipyretic (for fever, migraine, neuralgia) and as an anti-inflammatory agent (for rheumatism, rheumatoid arthritis); the drug has an antiaggregation effect, it’s prescribed for the prevention of thrombotic complications in patients with myocardial infarction, cerebrovascular disorders and other cardiovascular diseases. Side effects: irritation of the mucous membrane of the stomach, stomach ache, heartburn, ulcerogenic effect (stomach ulcers), Ray's syndrome. The soluble form of aspirin - acelizine. Administered intramuscularly and intravenously as an analgesic in the postoperative period, with rheumatic pain, oncological diseases.
Derivatives of pyrazolone and indoleacetic acid Analgin (metamizole-sodium) shows a pronounced analgesic, anti-inflammatory and antipyretic effect. Indications for use: with pain of different origin (head, dental, pain in trauma, neuralgia, radiculitis, myositis, fever, rheumatism). Assign inwards after eating to adults, as well as administer intramuscularly and intravenously. Side effects: edema, increased blood pressure, toxic effects on hematopoiesis (blood formula changes). Indomethacin (metinodal) exhibits pronounced analgesic, anti-inflammatory and antipyretic effect. Assign patients with rheumatoid arthritis, osteoarthritis, gout, thrombophlebitis. Apply inside, and indometacin ointment rubbed with acute and chronic polyarthritis, radiculitis.
Derivatives of paraaminophenol Paracetamol (panadol, epheralgan, tylenol) in the chemical structure is a metabolite of phenacetin and gives the same effects, but compared with phenacetin is less toxic. Apply as an antipyretic and anesthetic. Overseas paracetamol is manufactured in various dosage forms: tablets, capsules, mixes, syrups, effervescent powders, as well as in combination products such as coldrex, solpadein, panadol extra. Adverse effects include nausea, epigastric distress. Rarely it can cause skin rash. Acute toxicity may result in hepatic failureю
Derivatives of alkanic acids Diclofenac is a NSAID with pronounced antirheumatic, antiinflammatory, analgesic and antipyretic properties. Inhibition of prostaglandin biosynthesis is fundamental mechanism of action. In rheumatic diseases, it leads to marked relief from pain at rest, pain on movement, morning stiffness and swelling of the joints, as well as by an improvement in function. In posttraumatic and postoperative inflammatory conditions, diclofenac rapidly relieves both spontaneous pain and pain on movement and reduces inflammatory swelling and wound oedema. It also exerts a pronounced analgesic effect in moderate and severe pain of nonrheumatic origin. After the passage of the tablet through the stomach, it is completely absorbed. Diclofenac enters the synovial fluid, where maximum concentrations are measured two to four hours after peak plasma values have been attained. Adverse effects include nausea, vomiting, epigastric discomfort, skin rash, peptic ulcer, fluid retention, edema and impairment of hepatic function rarely.
Ibuprofen (brufen) shows a pronounced anti-inflammatory, analgesic and antipyretic effect, caused by blockade of prostaglandin synthesis. In patients with arthritis, it reduces the severity of pain and edema, increases the volume of movement in them. Indications for use: rheumatoid arthritis, osteoarthritis, gout, inflammatory diseases of the musculoskeletal system, pain syndrome.
Drugs of another chemical structure Acid mefenamic inhibits the formation and removes from the fabric depot mediators (serotonin, histamine) inflammation, suppresses the biosynthesis of prostaglandins, etc. The drug enhances cell resistance to damage, eliminates acute and chronic toothache and muscle and joint pain; Finds an antipyretic effect. Unlike other anti-inflammatory drugs, it almost does not detect ulcerogenic action. Sodium mefenaminate - by action is similar to the mefenamic acid. When administered locally, it helps to accelerate the healing of wounds and ulcers. Indications for use: ulcerative stomatitis, parodontosis, toothache, radiculitis.
Side effects of non-narcotic analgesics: ● ● ● ● ● irritation of the mucous membrane of the digestive canal, ulcerogenic effect (especially with the use of acetylsalicylic acid, indomethacin, butadiene); edema, fluid retention and electrolytes. Occur after 4 -5 days after taking the drug (especially butadiene and indomethacin); Ray's syndrome (hepatogenic encephalopathy) is manifested by vomiting, loss of consciousness, and coma. It can occur in children and adolescents due to acid acetylsalicylic teratogenic effect (acid acetylsalicylic and indomethacin should not be prescribed in the first trimester of pregnancy); leukopenia, agranulocytosis (especially in the derivatives of pyrazolone); retinopathy and keratopathy (due to postponement of indomethacin in the retina of the eye); allergic reactions; hepatotoxicity and nephrotoxicity in paracetamol (with long-term use, especially in high doses); hallucinations (indomethacin). With caution, prescribe the drug to patients with mental disorders, with epilepsy and parkinsonism.
Pharmacosafety: ● ● ● ● it is necessary to explain to the patient that uncontrolled use of drugs that are strong-acting substances is harmful to the body; to prevent the damaging effects of drugs on the mucous membranes, it is necessary to instruct the patient to use the medicine (with food, milk or a full glass of water) and to recognize the signs of peptic ulcers of the stomach (non-digesting of food in the stomach, vomiting with a "thick vein", gastric emptying); to prevent the development of agranulocytosis, it is necessary to monitor the blood test, to warn the patient about the need of notifying the doctor in case of symptoms of agranulocytosis (feeling cold, fever, sore throat, malaise); to prevent nephrotoxicity (hematuria, oliguria, crystalluria), it is necessary to control the amount of urine output, to warn the patient about the importance of informing the doctor in case of any symptoms; remind the patient that in case of drowsiness after taking indomethacin it is impossible to sit behind a car and work with dangerous equipment; Non-narcotic analgesics are not compatible with sulfanilamide preparations, antidepressants, anticoagulants; Salicylases should not be prescribed in combination with other non-narcotic analgesics (enhancement of ulcerogenic action) and anticoagulants (increased risk of bleeding).