Drugs acting on Cholinergic System By Ms Sindhu

Drugs acting on Cholinergic System By Ms. Sindhu Priya E S Assistant Professor Dept. of Pharmacology YPCRC
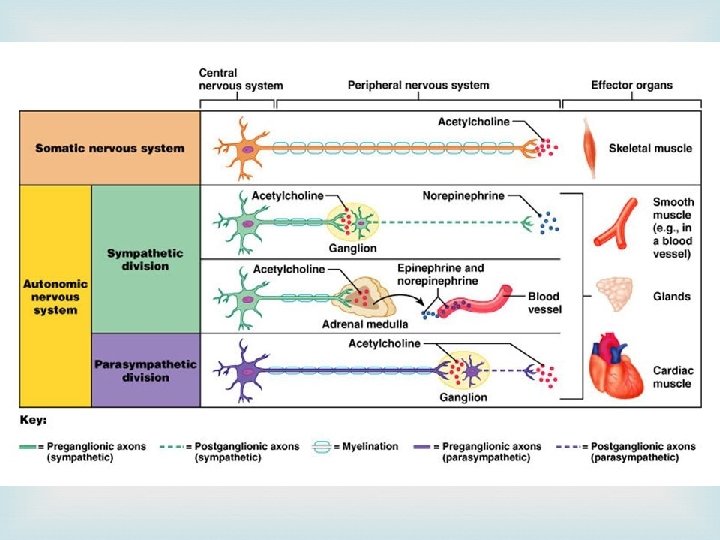

Sites of cholinergic transmission
 is a major neurohumoral transmitter at autonomic, somatic as")
Cholinergic transmission Acetyl Choline (Ach) is a major neurohumoral transmitter at autonomic, somatic as well as central sites

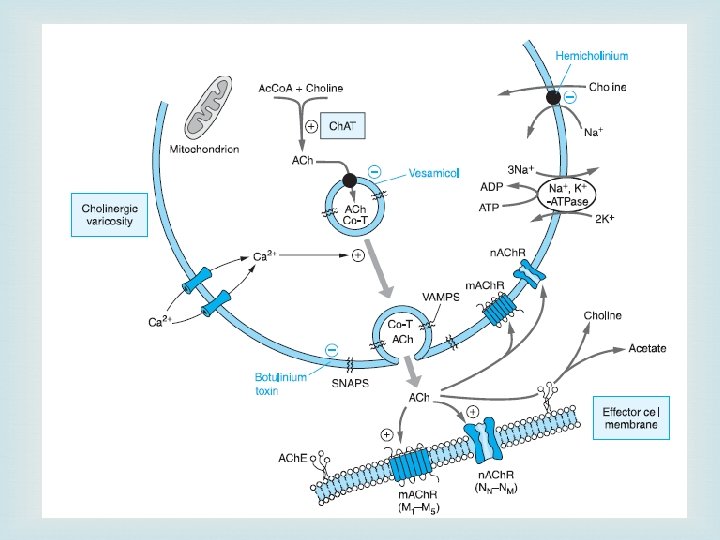
Synthesis, storage and destruction of Ach

ACh. E and BCh. E
 -GPCR Nicotinic (N) – Ligand")
Cholinoceptors Two classes of receptors for Ach Muscarinic (M) -GPCR Nicotinic (N) – Ligand gated cation channels

Muscarinic receptors They are selectively stimulated by muscarine and blocked by atropine. They are located primarily on autonomic effector cells in heart, blood vessels, eye, smooth muscles and glands of gastrointestinal, respiratory and urinary tracts, sweat glands, etc. and in the CNS. Subsidiary muscarinic receptors are also present in autonomic ganglia where they appear to play a modulatory role by inducing a long-lasting late EPSP.

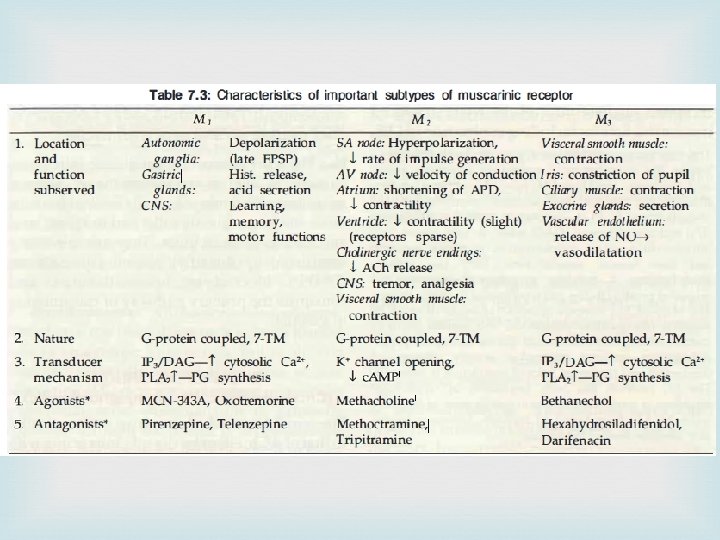
Subtypes of M receptors M 1, M 2, M 3, M 4 and M 5 receptors M 1 receptors Location: autonomic ganglia, CNS, gastric glands Functions: Depolarization (late EPSP), learning, memory and motor function, Hist release, acid secretion

M 2 receptors Location 1. SA node 2. A V node 3. Atrium 4. Ventricle 5. Cholinergic nerve endings 6. CNS 7. Visceral smooth muscle Function 1. Hyperpolarization & rate of impulse generation 2. velocity of conduction 3. Shortening of APD, contractility 4. contractility (slight)(receptors sparse) 5. ACh release 6. tremor, analgesia 7. contraction

M 3 receptors Location Functions Visceral smooth Contraction muscles Exocrine glands Secretion Vascular endothelium Release of NO leading to vasodilation

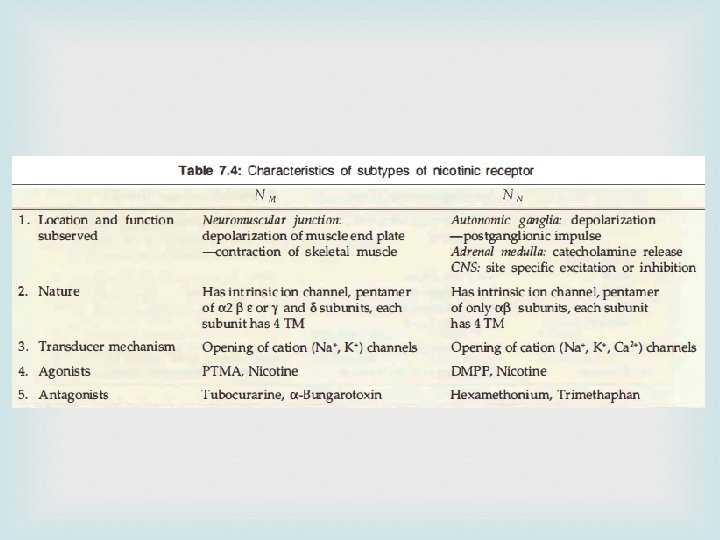
Nicotinic receptors They are selectively activated by nicotine and blocked by tubocurarine or hexamethonium. They are rosette-like pentameric structures which enclose a ligand gated cation channel: their activation causes opening of the channel and rapid flow of cations resulting in depolarization and an action potential. On the basis of location and selective agonists and antagonists two subtypes NM and NN are recognized

NM receptors These are present at skeletal muscle end plate are selectively stimulated by phenyl trimethyl ammonium (PTMA) and blocked by tubocurarine. They mediate skeletal muscle contraction.
, adrenal")
NN receptors These are present on ganglionic cells (sympathetic as well as parasympathetic), adrenal medullary cells and in spinal cord and certain areas of brain. They are selectively stimulated by dimethyl phenyl piperazinium (DMPP), blocked by hexamethonium, and constitute the primary pathway of transmission in ganglia.

Cholinergic drugs Cholinomimetics or Parasympathomimetics Drugs which produce actions similar to that of ACh either by directly interacting with cholinergic receptors or by increasing the availability of ACh at these sites Eg: 1. Cholinergic agonists 2. Anticholinesterases

1. Cholinergic agonists A. Choline esters B. Alkaloids Acetyl choline Methacholine Carbachol Bethanechol Muscarine Pilocarpine Arecoline

Pharmacological actions of Choline esters a. Muscarinic actions b. Nicotinic actions c. CNS actions
 Site of action Function Effect SA node")
a. Muscarinic actions 1. Heart (M 2) Site of action Function Effect SA node Decreases rate of diastolic depolarization, Reduced rate of impulse generation Bradycardia, cardiac arrest A-V node Purkinjee fibres Increased refractory period Conduction is slowed Atrium and ventricles Decreased contractility Atrial fibrillation and flutter
 Vasodilation by")
Sl. No Site of action Function Effect 2 Blood vessels (M 3) Vasodilation by NO release fall in BP and flushing 3 Smooth muscle (M 3) • GIT- contraction, increased peristalsis, sphincters relax • Ureter-peristalsis increases • Bronchial musclesconstrict • Evacuation of bowel • Voiding of bladder • Bronchospasm, dyspnoea, precipitation of asthma 4 Glands (M 2) Increased secretions Increased sweating, salivation, lacrimation, gastric secretion 5 Eye (M 3) • Contraction of circular muscle of iris • Contraction of ciliary muscle • Miosis • Spasm of accomodation, reduced intraocular pressure

b. Nicotinic actions Sl. No Site of action Function Effect 1 Autonomic ganglia Stimulation of sympathetic and parasympathetic ganglia Tachycardia and rise in BP 2 Skeletal muscle • Contraction of muscle • Muscle twiching and fasciculations c. CNS actions Direct injection into brain causes arousal and later depression

2. Cholinomimetic alkaloids Pilocarpine Obtained from leaves of Pilocarpus microphyllus Has muscarinic and ganglionic actions Actions Sweating, salivation Cardiovascular effects: low dose causes fall in BP, high dose causes rise in BP Eye: Miosis and fall in intraocular tension Uses Eye drops in Glaucoma

Therapeutic uses Gastrointestinal disorders: Bethanechol 10 -20 mg 3 or 4 times a day orally used in cases of postoperative abdominal distention and in gastric atony Urinary bladder disorders: Bethanechol may be useful in treating urinary retention Xerostomia: Pilocarpine is administered orally in 5– 10 mg doses Glaucoma: Pilocarpine is used in the treatment of glaucoma, where it is instilled into the eye usually as a 0. 5– 4% solution Ach is available as an olphthalmic surgical aid used to produce rapid miosis

Contraindications Muscarinic agonists are contraindicated in Asthma Hyperthyroidism Coronary insufficiency or hypotensive patients Acid-peptic disease
 Muscarine intoxication (salivation, lacrimation, nausea, vomiting, headache, visual disturbances, abdominal colic,")
Mushroom poisoning (Mycetism) Muscarine intoxication (salivation, lacrimation, nausea, vomiting, headache, visual disturbances, abdominal colic, diarrhea, bronchospasm, bradycardia, hypotension, shock) develop within 30– 60 minutes of ingestion Treatment with atropine (1– 2 mg intramuscularly every 30 minutes) effectively blocks these effects
 are agents which inhibit Ch. E, protect ACh from hydrolysis-produce cholinergic")
Anticholinesterases (anti-Ch. Es) are agents which inhibit Ch. E, protect ACh from hydrolysis-produce cholinergic effects in vivo and potentiate Ach both in vivo and in vitro. Some anti Ch. Es have additional direct action on cholinergic receptors
, Neostigmine, Pyridostigmine, Edrophonium, Rivastigmine, Donepezil, Galantamine Acridine: Tacrine")
Classification 1. Reversible Carbamates: Physostigmine (Eserine), Neostigmine, Pyridostigmine, Edrophonium, Rivastigmine, Donepezil, Galantamine Acridine: Tacrine 2. Irreversible Organophosphates: Dyflos (DFP), Echothiophate, Parathion*, Malathion*, Diazinon*, Tabun£, Sarin£, Soman£ Carbamates: Carbaryl*, Propoxur* (BAYGON), Insecticides and Nerve gas
, Neostigmine Pyridostigmine Rivastigmine Edrophonium Tacrine Donepezil")
Anticholinesterases Reversible Irreversible Organophosphates Noncarbamates Carbamates Physostigmine (Eserine), Neostigmine Pyridostigmine Rivastigmine Edrophonium Tacrine Donepezil Galantamine Carbamates Carbaryl*, Propoxur* (BAYGON), Dyflos (DFP), Echothiophate, Parathion*, Malathion*, Diazinon*, Tabun£, Sarin£, Soman£

Chemistry Anti-Ch. Es are either esters of carbamic acid or derivatives of phosphoric acid. In carbamates, R 1 may be tertiary amino N which is nonpolar or quaternary ammonium N+ which is lipid insoluble (edrophonium) All organophosphates are highly lipid soluble except echothiophate

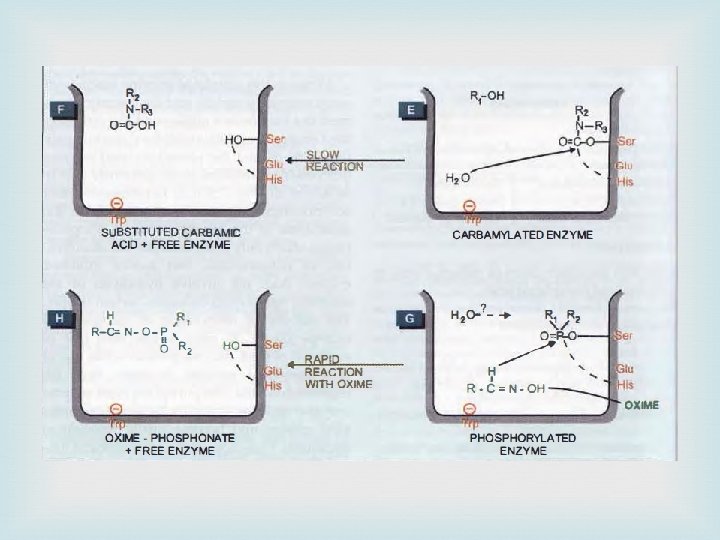
Mechanism of action

Pharmacological actions Ganglia : High doses cause persistent depolarization of the ganglionic nicotinic receptors and blockade of transmission CVS: CVS effects are complex. muscarinic action would produce bradycardia and hypotension, ganglionic stimulation would tend to increase heart rate and BP. Skeletal muscles: Twitching and fasciculations. Higher doses cause persistent depolarization of endplates resulting in blockade of neuromuscular transmission weakness and paralysis. Others : stimulation of smooth muscles and glands of the gastrointestinal, respiratory, urinary tracts and in the eye

Pharmacokinetics Physostigmine: Readily absorbed from GIT and parenteral sites. It penetrates cornea freely. Crosses BBB and hydrolysed by Ch. E Neostigmine and congeners: These are poorly absorbed orally; oral dose is 20 -30 times higher than parenteral dose. They do not effectively penetrate cornea or cross blood-brain barrier Organophosphates: These are absorbed from all sites including intact skin and lungs. They are hydrolyzed as well as oxidized in the body and little is excreted unchanged

Contraindications Peptic ulcer Hypotension Asthma COPD Seizure patients

Therapeutic Uses Miotic a. Glaucoma b. Reverse mydriatic effect Myasthenia gravis Postoperative paralytic ileus/urinary retention Postoperative decurarization Cobra bite Belladonna poisoning Alzheimer's disease

Myasthenia gravis is an autoimmune disorder caused due to development of antibodies directed to nicotinic receptor at the motor endplate (NM) NM receptors are reduced to 1/3 or less and structural damage to NMJ

Affected organs: eyelids, external ocular, facial and pharyngeal muscles are affected first. Later muscles of limbs and respiratory system are affected. Symptoms: fatigue and weakness Diagnosis: a. Ameliorative test: Edrophonium 2 mg i. v. injection/neostigmine with atropine pretreatment b. Provocative test: 0. 5 mg D-tubocurarine i. v. Treatment: Neostigmine 15 mg orally 6 hourly / pyridostigmine Thymectomy Corticosteroids : prednisolone 30 -60 mg/day Immunosuppresants : azathioprine and cyclosporine

ANTICHOLINESTERASE POISONING Anticholinesterases are easily available & extensively used as agricultural and household insecticides; accidental homicidal poisoning is common. Symptoms are: • Irritation of eye, lacrimation, salivation, sweating, copious tracheobronchial secretions, miosis, blurring of vision, breathlessness, colic, bronchospasm, involuntary defecation and urination. • Fall in BP, bradycardia or tachycardia, cardiac arrythmias, vascular collapse. • Muscular fasciculations, weakness, respiratory paralysis (central as well as peripheral). • Excitement, tremor, ataxia, convulsions, coma and death. • Death is generally due to respiratory failure

Treatment Termination of further exposure to poison Maintain patent airway Supportive measures-maintain BP, hydration, control of convulsions with judicious use of diazepam Specific antidotes( a) Atropine (b) Cholinesterase reactivators: Oximes

Anticholinergic drugs Also called as Muscarinic receptor antagonists, Atropinic, Parasympatholytic drugs Anticholinergic drugs are those which block actions of ACh on autonomic effectors and in the CNS exerted through muscarinic receptors Nicotinic antagonists also block certain actions of ACh, they are generally referred to as 'ganglion blockers (NN)' and 'neuromuscular blockers (NM)
. 2. Semisynthetic derivatives: Homatropine, Atropine methonitrate, Hyoscine")
Classification 1. Natural alkaloids: Atropine, Hyoscine (Scopolamine). 2. Semisynthetic derivatives: Homatropine, Atropine methonitrate, Hyoscine butyl bromide, Ipratropium bromide, Tiotropiumbromide. 3. Synthetic compounds (a) Mydriatics: Cyclopentolate, Tropicamide (b) Antisecretory-antispasmodics: (i) Quaternary compounds: Propanthelin, Oxyphenonium, Clidinium, Pipenzolate, methylbromide, Isopropamide, Glycopyrrolate. (ii) Tertiary amines: Dicyclomine, Valethamate, Pirenzepine. (c) Vasicoselective: Oxybutynin, Flavoxate, Tolterodine. (d) Antiparkinsonian: Trihexyphenidyl (Benzhexol), Procyclidine, Biperiden.

Pharmacological actions 1. CNS actions Site of action Function Effect Medullary centers Stimulation of vagal, respiratory and vasomotor centers Bradycardia, cardiac arrest Vestibular excitation depressed Antimotion sickness property Basal ganglia Block Cholinergic over reactivity Suppresses tremor & rigidity of parkinsonism High doses cause cortical excitation, disorientation, hallucinations and delirium respiratory depression and coma. restlessness, followed by

Sl. No Site of action Function Effect 2 Heart Block M 2 receptors on SA node and shortened refractory period of A-V node Tachycardia & increased A-V conduction 3 Smooth muscle (M 3) • GIT- reduced contraction, decreased peristalsis, • Ureter-peristalsis decreases • Bronchodilation • Constipation • Urinary retension • Reduces airway resistance 4 Glands (M 2) decreased secretions Drying of mouth, difficulty in swallowing and raised body temperature 5 Eye (M 3) • Block of M receptors in constrictor papillae • Relaxation of ciliary muscle • Mydriasis • cycloplegia • Increased IOP • Loss of light reflex • Local anesthetic action on cornea

Pharmacokinetics Parameter Atropine Hyoscine Absortion Rapid from GIT Cornea Freely penetrates BBB Cannot cross BBB freely Better BBB penetration Metabolism 50 % in liver Completely metabolized Excretion Urine

Therapeutic uses 1. Antisecretory Preanaesthetic medication Peptic ulcer Pulmonary embolism 2. 3. 4. 5. Antispasmodic Bronchial asthma, asthmatic bronchitis COPD As mydriatic and cycloplegic Central actions Parkinsons disease Motion sickness 6. Used in the treatment of muscarinic poisoning

Side effects and toxicity Belladonna poisoning may occur due to drug overdose or consumption of seeds and berries of belladonna/ datura plant. Dry mouth, difficulty in swallowing, fever, difficulty in micturition, decreased bowel sounds, Dilated pupil, photophobia, blurring of near vision, Excitement, psychotic behaviour, dreadful visual hallucinations. weak and rapid pulse, cardiovascular collapse with respiratory depression. Convulsions and coma occur only in severe poisoning. Treatment: gastric lavage and Physostigmine 1 -3 mg s. c. or i. v.

Contraindications In narrow iridocorneal angle-may precipitate acute congestive glaucoma Elderly males with prostatic hypertrophy Interactions slower absorption and peripheral degradation of levodopa Antacids interfere with absorption of anticholinergics Antihistaminics, tricyclic antidepressants, phenothiazines, disopyramide, pethidine have anticholinergic property

Ganglion blocking agents Drugs blocking NN receptors in the ganglia are called as ganglion blocking agents Classification A. Competitive blockers Quaternary ammonium compounds: Hexamethonium, Pentolinium Amines (secondary/tertiary): Mecamylamine, Pempidine Monosulfonium compound: Trimethaphan camforsulfonate B. Persistent depolarising blockers Nicotine (large dose) Anticholinesterases (large dose)

Pharmacological actions

Neuomuscular blocking agents Skeletal muscle relaxants are drugs that act peripherally at neuromuscular junction/ muscle itself or centrally in the cerebrospinal axis to reduce muscle tone and/ or cause paralysis.
 blockers")
Classification of peripherally acting muscle relaxants I. Neuromuscular blocking agents a. Non-depolarizing (Competitive) blockers Long acting: d-Tubocurarine, Pancuronium, Doxacurium, Pipecuronium Intermediate acting: Vecuronium, Atracurium, Cistracurium, Rocuronium, Rapacuronium Shortacting : Mivacurium b. Depolarizing blockers Succinylcholine (SCh. , Suxamethonium), Decamethonium (C-10) I I. Directly acting agents Dantrolene sodium and Quinine

Curare Extract of plants used as arrow poison for hunting by tribal people Natural sources of curare Strychnos toxifera, Chondrodendron tomentosum The animals got paralysed even if not killed by the arrow.

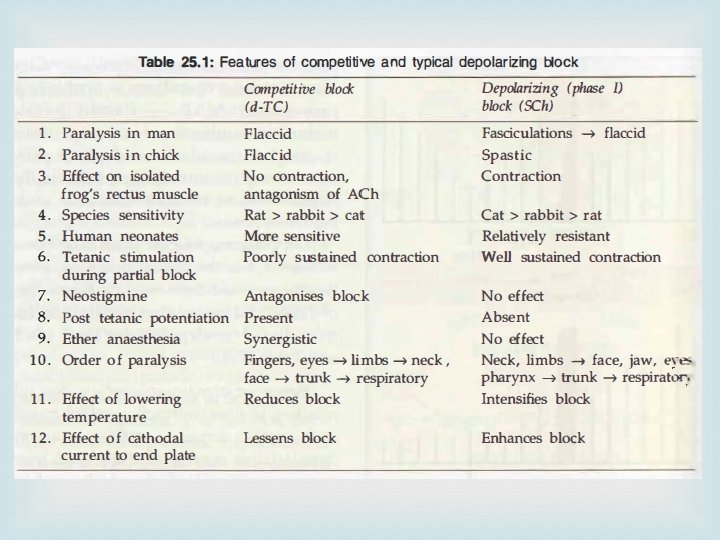
Mechanism of action Non depolarizing or Competitive blockers: They block NM receptors on motor-end plate competitively. They have affinity, but no intrinsic activity. Depolarizing blockers: They have affinity and also submaximal intrinsic activity. They cause phase I and phase II block.

Mechanism of action
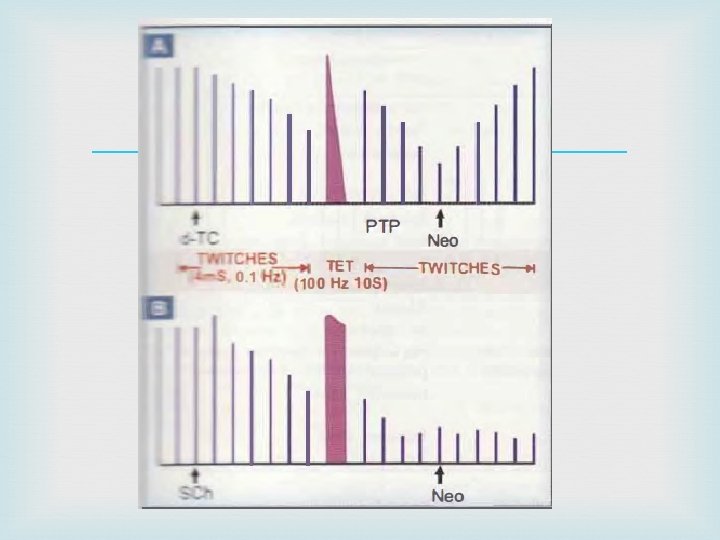

Pharmacological actions 1. Skeletal muscles Nondepolarizing blockers rapidly produces muscle weakness followed by flaccid paralysis. Small fast response muscles (fingers, extraocular) are affected first; paralysis spreads to hands, feet-arm, leg, neck, face-trunk-intercostal muscles-finally diaphragm: respiration stops. Depolarizing blockers typically produce fasciculations lasting a few seconds before inducing flaccid paralysis, but fasciculations are not prominent in wellanaesthetized patients.

2. Autonomic ganglion Little effect on ganglionic blockage by d-TC. Newer drugs devoid of it. 3. Histamine release d-TC releases histamine from mast cells which causes hypotension produced by d-TC; flushing, bronchospasm and increased respiratory secretions are other effects. Intradermal injection of d-TC produces a wheal similar to that produced by injecting histamine

4. C. V. S. d-Tubocurarine produces significant fall in BP. This is due to( a) ganglionic blockade (b) histamine release (c) reduced venous return Heart rate may increase due to vagal ganglionic blockade Pancuronium and vecuronium also tend to cause tachycardia All newer nondepolarizing drugs have negligible effects on BP and HR. Generally SCh causes bradycardia initially due to activation of vagal ganglia followed by tachycardia and rise in BP due to stimulation of sympathetic ganglia.

Pharmacokinetics All neuromuscular blockers are polar quaternary compounds-not absorbed orally They do not cross cell membranes, have low volumes of distribution Do not penetrate placental or blood-brain barrier. They are practically always given i. v. Drugs that are primarily metabolized in the plasma/liver have short half life, by kidneys will have long t 1/2 SCh is rapidly hydrolysed by plasma buteryl cholinesterase to succinylmonocholine and then to succinic acid + choline

Interactions Thiopentone sodium and SCh given together reacts chemically General anaesthetics will potentiate the actions of neuromuscular blocking agents. Malignant hyperthermia is produced by halothane and isoflurane Anticholinesterases reverse the action of competitive blockers. Antibiotics such as Aminoglycoside antibiotics potentiates the action of competitive blockers. Diuretics produce hypokalemia enhances competitive block. Calcium channel blockers Verapamil and others potentiate both competitive and depolarizing neuromuscular blockers.

Toxicity Respiratory paralysis Flushing is common with d-TC Fall in BP and cardiovascular collapse can occur Cardiac arrhythmias especially with SCh Precipitation of asthma with d-TC and histamine releasing drugs Postoperative muscle soreness

Therapeutic uses Adjuvants to anesthetics Assisted ventilation Convulsions and trauma Severe cases of tetanus and status epilepticus, which are not controlled by diazepam or other drugs

Advantages of newer drugs No or minimal ganglionic, cardiac or vascular effects. No or minimal histamine release. Many are short acting: easy reversal. Some are rapid acting: provide alternative to SCh without the attendant complications.
 calcium channels")
Directly acting muscle relaxants Dantrolene acts on the Ry. R (Ryanodine Receptor) calcium channels in the sarcoplasmic reticulum of skeletal muscles and prevents their depolarization triggered opening. Intracellular release of Ca 2+ needed for excitation-contraction coupling is interfered with. Used orally dantrolene (25 -100 mg QID) reduces spasticity in upper motor neurone disorders, hemiplegia, paraplegia, cerebral palsy and multiple sclerosis.
 it is the drug")
Used i. v. ( 1 mg/kg repeated as required) it is the drug of choice for malignant hyperthermia Adverse effects: Muscular weakness is the dose limiting side effect. Sedation, malaise, light headedness and other central effects occur, but
- Slides: 69