DRUG TABLET OVERDOSAGE Drug Overdosage What is it

DRUG / TABLET OVERDOSAGE

Drug Overdosage What is it that is not a poison? All things are poison and nothing is without poison. Solely, the dose determines that a thing is not a poison Paracelsus (1493 – 1541)

Drug overdosage Poisoning – development of harmful effects following exposure to chemicals Overdosage – exposure to excessive amounts of a substance normally intended for consumption and does not necessarily imply poisoning Harrison

General approach Poisoned patient Treatment Airway Breathing Circulation “DONT”/Decontamination Enhanced elimination Focused therapy Get Tox help Diagnosis History Physical examination Toxidrome recognition Diagnostic tests
 Propranolol, poppies, propoxyphene, physostigmine Anticholinesterase drugs, antiarrhythmics Clonidine, CCBs Ethanol")
Vital signs Bradycardia (PACED) Propranolol, poppies, propoxyphene, physostigmine Anticholinesterase drugs, antiarrhythmics Clonidine, CCBs Ethanol or other alcohols Digoxin, digitalis
 Free base or other forms of cocaine, freon Anticholinergics, antihistamines,")
Vital signs Tachycardia (FAST) Free base or other forms of cocaine, freon Anticholinergics, antihistamines, antipsychotics, amphetamines, alcohol – withdrawal Sympathomimetics, solvent abuse, strychnine Theophylline, TCAs, thyroid hormones
 Carbon monoxide Opioids Oral hypoglycemics, insulins Liquor (alcohol) Sedative-hypnotics")
Vital signs Hypothermia (COOLS) Carbon monoxide Opioids Oral hypoglycemics, insulins Liquor (alcohol) Sedative-hypnotics
 Neuroleptic malignant, nicotine Antihistamines, alcohol withdrawal Salicylates, sympathomimetics, serotonins Anticholinergics,")
Vital signs Hyperthermia (NASA) Neuroleptic malignant, nicotine Antihistamines, alcohol withdrawal Salicylates, sympathomimetics, serotonins Anticholinergics, antidepressants, antipsychotics
 Clonidine, CCBs Rodenticides (arsenic, cyanide) Antidepressants, aminophylline, antihypertensives Sedative- hypnotics")
Vital signs Hypotension (CRASH) Clonidine, CCBs Rodenticides (arsenic, cyanide) Antidepressants, aminophylline, antihypertensives Sedative- hypnotics Heroin or other opiates
 Cocaine Thyroid supplements Sympathomimetics Caffeine Anticholinergics, amphetamines")
Vital signs Hypertension ( CT SCAN ) Cocaine Thyroid supplements Sympathomimetics Caffeine Anticholinergics, amphetamines Nicotine
 PCP, paraquat, pneumonitis(chem. ), phosgene ASA, and")
Vital signs Rapid respiration ( PANT ) PCP, paraquat, pneumonitis(chem. ), phosgene ASA, and other salicylates NCPE, nerve agents Toxin-induced metabolic acidosis
 Sedative-hypnotics ( Barb’s & Benzodiaz) Liquor (")
Vital signs Slow respiration ( SLOW ) Sedative-hypnotics ( Barb’s & Benzodiaz) Liquor ( alcohols ) Opioids Weed ( marijuana )
 Lead, lithium Ethanol, ethylene glycol, ethchlorvynol TCAs, thallium,")
Vital signs Coma ( LETHARGIC ) Lead, lithium Ethanol, ethylene glycol, ethchlorvynol TCAs, thallium, toluene Heroin, hemlock, HE, heavy metals, hydrogen sulphide, hypoglycemics Arsenic, antidepressants, anticonvulsants, antipsychotics, antihistamines GHB – gamma hydroxybutyrate Isoniazid, insulin Carbon monoxide, cyanide, clonidine
 OPCs, OHAs TCAs Isoniazid, insulin Sympathomimetics, strychnine, salicylates Camphor, cocaine,")
Seizures ( OTIS CAMPBELL) OPCs, OHAs TCAs Isoniazid, insulin Sympathomimetics, strychnine, salicylates Camphor, cocaine, CO, cyanide, chlorine-HC Amphetamines, anticholinergics Methyl xanthines, methanol Phencyclidine, propranolol BNZ-withdrawal, botanicals(nicotine), bupropion Ethanol withdrawal, ethylene glycol Lithium, lidocaine
 Cholinergics, clonidine, carbamates Opiates, OPCs Phenothiazines, pilocarpine, pontine HE")
Pupils/Eye Miosis ( COPS ) Cholinergics, clonidine, carbamates Opiates, OPCs Phenothiazines, pilocarpine, pontine HE Sedative-hypnotics Mydriasis ( SAW ) Sympathomimetics Anticholinergics Withdrawal Nystagmus – phenytoin, barbiturates

EXAMINATION OF SKIN DRY SKIN -belladona, datura HEAVY PRESPIRATION - organophosphates PINK - carbon monoxide BULLAE - barbiturates VASCULITIS - propylthiouracil, hyadantoin RAYNAUDS - betablockers, ergot SERUM SICKNESS - betalactams, betablockers

BASIC LAB WORK UP GLYCEMIC STATUS ABG SERUM ELECTROLYTES RFT& LFT HEMOGRAM PREGNANCY TESTS – CHILD BEARING AGES DRUG LEVELS IF POSSIBLE – BLOOD, URINE
![ANION GAP Normal anion gap [Na – (Cl – HCO 3)] -12 meq/l An](http://slidetodoc.com/presentation_image/97a30fd5faef5596a2b1f5d0ce3ba6f6/image-18.jpg "ANION GAP Normal anion gap [Na – (Cl – HCO 3)] -12 meq/l An")
ANION GAP Normal anion gap [Na – (Cl – HCO 3)] -12 meq/l An increase>20 m. Eq/l indicates organic acidosis Increased anion gap – lactic acidosis, uremia & sepsis and Toxins like ethylene glycol, methanol, paraldehyde & salicylate Decreased AG — lithium, hyperkalemia hypercalcemia , hypermagnesemia

Hypoglycemia β – blockers Ethanol Insulin Oral hypoglycemics Quinine Salicylates

Hyperglycemia Acetone β – agonists CCB’s Iron Theophylline Vacor

ELECTROLYTE DISTURBANCES Hyperkalemia ---potassium sparing diuretics Hypokalemia---ampho. B, cyclosporine, diuretics Hyponatremia---diuretics, naso gastric losses Hypomagnesemia---cisplatin, cyclosporin, diuretics

DRUGS CAUSING HIGH ANION GAP or METABOLIC ACIDOSIS ACETAMINOPHEN>75 gm AMILORIDE INH DAPSONE CYANIDE IRON KETAMINE METFORMIN NSAIDS NITROPRUSSIDE TERBUTALINE OUT DATED TETRACYCLINE

ACUTE HEPATO TOXICITY ACUTE CYTOLYTIC HEPATITS— acetaminophen ACUTE CHOLESTATIC HEPATITS or MIXED —macrolides, phenothiazines ACUTE BLAND CHOLESTASIS—anabolic steroids, estrogens.
 Chloral hydrate, cocaine packets, calcium")
Abdominal radiographs Agents visible on ABR’s ( COINS ) Chloral hydrate, cocaine packets, calcium Opium packets Iron, lead, arsenic, mercury (H. metals) Neuroleptic agents Sustained – release or EC agents
 Meprobamate, methadone Opioids Phenobarbital, propoxyphene, paraquat, phosgene Salicylates")
Chest Radiographs NCPE ( MOPS ) Meprobamate, methadone Opioids Phenobarbital, propoxyphene, paraquat, phosgene Salicylates
 Diarrhoea, diaphoresis Urination Miosis Bradycardia, bronchorrhoea Emesis")
Toxidromes Cholinergics – OPCs, carbamates, pilocarpine (DUMBELLS) Diarrhoea, diaphoresis Urination Miosis Bradycardia, bronchorrhoea Emesis Lacrimation Lethargic Salivation

Toxidromes Nicotinic – days of the week Monday – mydriasis Tuesday – tachycardia Wednesday – weakness Thursday – tremors Friday – fasciculations Saturday – seizures Sunday - somnolence

Toxidromes Anticholinergic – antihistamines, TCAs, atropine, benztropine, phenothiazines Hyperthermia Flushing Dry skin Dilated pupils Delirium, hallucinations Tachycardia Urinary urgency and retention Traditional description Hot as a hare Dry as a bone Red as a beet Blind as a bat Mad as a hatter

Toxidromes Sympathomimetics – cocaine, amphetamines, ephedrine, phencyclidine Mydriasis Tachycardia Hypertension Hyperthermia Seizures

Toxidromes Opioid – heroin, morphine, codeine, methadone, fentanyl, oxycodone Miosis Hypotension Hypoventilation Coma

Toxidromes Drug Withdrawal Diarrhoea Mydriasis Goose flesh Tachycardia Lacrimation Hypertension Yawning Cramps Hallucinations Seizures

CRITERIA FOR ICU ADMISSION Respiratory depression - Pa. CO 2>45 mm. Hg Emergency intubation Seizure Cardiac arrhythmia Systolic BP<80 mm. Hg Glasgow score <12 Need for emergency HD, HP. Hypothermia, Hyperthermia & neuroleptic malignant syndrome TCA toxicity with QRS>0. 12 secs/QT>0. 5 secs Pulmonary edema

Goals of Therapy Support of vital signs Prevention of further absorption Enhancement of elimination Administration of specific antidotes Prevention of re-exposure

Multi-dose Activated Charcoal 1 g/kg; 4 th hourly, for drugs with enteral circulation Carbamazepine Dapsone, Diazepam, Digoxin Glutethimide Meprobamate, Methotrexate Phenobarbitol, phenytoin Salicylate Theophylline Valproic acid

Scenario An under graduate student of our college with ingestion of 20 pills and admitted in our toxicology with vomiting and deranged LFT later….
 ~ 5% NAPQI")
Acetaminophen Metabolism ~ 50% ~ 45% P 450 Glucuronidation (non toxic) ~ 5% NAPQI Glutathione + NAPQI = nontoxic product Sulfation (non toxic) N-acetylcysteine (NAC) Liver cell damage

Paracetamol Toxicity 90% Conjugation P 4 50 NAPQI Glutathione NAPQI

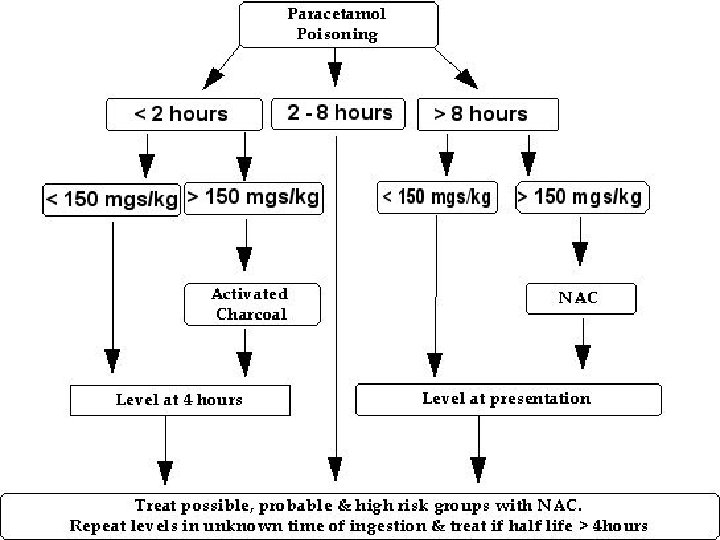
PARACETAMOL Hepatic toxicity – depletion of hepatic glutathione and accumulation of toxic metabolite – N-acetyl-p-benzo quinonimine Toxic dose – >140 mg/kg or >7. 5 g Toxicity increased with alcohol intake, INH intake Acetaminophen levels >10 mcg/ml Hepatic enzymes – rise in 24 hrs and peak at 72 -96 hrs and recovery follows
 and hepatotoxicity (%) Smilkstein MJ et al. Efficacy of oral")
Time to N-acetylcysteine (hours) and hepatotoxicity (%) Smilkstein MJ et al. Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose: Analysis of the national multicenter study (1976 to 1985). N Engl J Med 1988; 319: 1557 -1562

PARACETAMOL Activated charcoal – hepatoprotective N-acetylcysteine – specific antidote 140 mg/kg stat and 70 mg/kg for 17 doses every 4 hrs – orally IV-Acetadote 150 mg/kg in 1 hr in 200 ml D 5 and 50 mg/kg in 500 ml in 4 hrs followed by 100 mg/kg in 500 ml over 16 hrs Alternate medication: oral methionine

Paracetamol - summary Ingestion < 140 mg/kg is probably not toxic If no serum level available treat based on dose IV acetylcysteine or oral methionine Start antidote within 8 hours Liver or kidney damage delayed 24 -48 hrs

Scenario A 45 year old man, known RHD patient on treatment presented to our emergency department with unconsciousness. He developed VT and was stabilized at cardiology with defibrillation. He was later shifted to our toxicology? ? ?

Cyclic Antidepressants Amitryptilline, imipramine, desipramine, nortriptyline, doxepin and protriptyline Central and peripheral anticholinergic activity, block reuptake of norepinephrine & serotonin, alpha blocking (depression of myocardial contractility), quinidine like (conduction defects), and CNS effects >50 mg/kg is lethal Anti-Cholinergic, Cardiovascular and CNS

Cyclic Antidepressants Gastric lavage regardless of time of presentation and repetitive activated charcoal Continuous cardiac monitoring Maintain alkaline p. H 7. 45 -7. 55 – Na. HCo 3 / p. CO 2 Arrhythmia management – lidocaine/phenytoin, magnesium, atrial overdrive pacing / V. pacing CNS – Physostigmine – 2 mg IV over 1 min or barbiturates, diazepam Respiratory - ventilation
 citalopram escitalopram fluoxetine fluvoxamine paroxetine sertraline RIMA")
Newer antidepressants SSRIs (specific serotonin reuptake inhibitors) citalopram escitalopram fluoxetine fluvoxamine paroxetine sertraline RIMA (reversible inhibitor of monoamine oxidase A) moclobemide
 Na. SSA (noradrenergic and specific serotonergic antidepressant)")
Newest antidepressants SNRI (serotonin noradrenergic reuptake inhibitors) Na. SSA (noradrenergic and specific serotonergic antidepressant) venlafaxine mirtazapine Na. RI (selective noradrenaline reuptake inhibitor ) reboxetine

NAselective Nonselective 5 -HTselective Ratio NA: 5 -HT uptake inhibition Selectivity of antidepressants 1000 Nisoxetine 100 Nomifensine Maprotiline (approx) 10 1 0. 01 0. 001 Desipramine Imipramine Nortriptyline Amitriptyline Clomipramine Trazodone Zimelidine Fluoxetine Citalopram (approx)

RIMA Na. SSA Na. RI SSRI Na. SSA
 mental status agitation/delirium motor system clonus/myoclonus tremor/shivering")
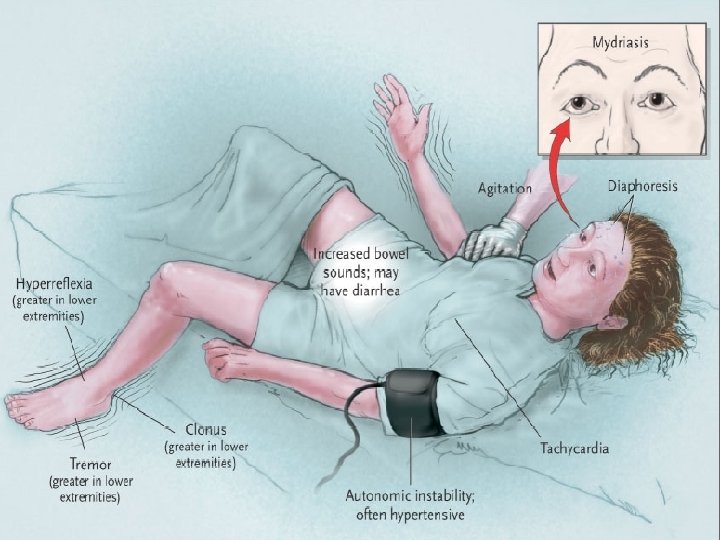
Serotonin excess Primary neuroexcitation (5–HT 2 A) mental status agitation/delirium motor system clonus/myoclonus tremor/shivering hyperreflexia/hypertonia autonomic system inducible/spontaneous/ocular diaphoresis/tachycardia/mydriasis Other responses to neuroexcitation fever rhabdomyolysis
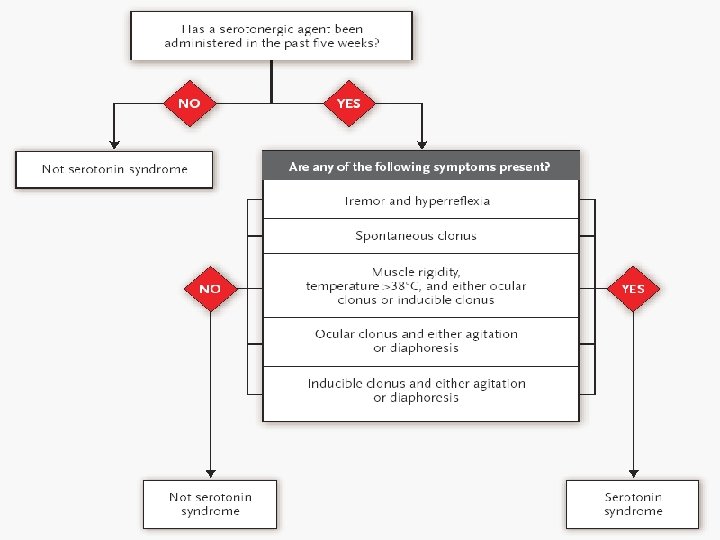
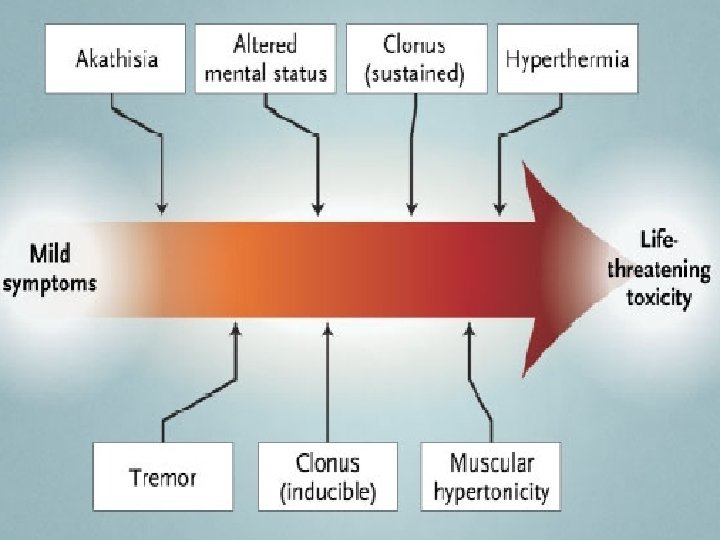

Severe serotonin toxicity Combination therapy Rapidly rising temperature Respiratory failure multiple different mechanisms of serotonin elevation hypertonia/rigidity Spontaneous clonus Seizures – fluoxetine, citalopram Tachycardia, QT - citalopram

Therapy Oral therapy q 4– 6 h PO ( 5–HT 1 A & 5 -HT 2 A antagonist) Oral therapy unsuitable or fails cyproheptadine 12 mg stat then 4– 8 mg chlorpromazine 25– 50 mg IV stat then up to 50 mg orally or IV q 6 h Ventilation impaired and/or fever > 39 o. C anaesthesia, muscle relaxation ± active cooling chlorpromazine 100– 400 mg IM/IV over first two hours

Conclusions Serotonin toxicity is a spectrum disorder not a discrete syndrome Newer agents with little or no risk of serotonin toxicity Reboxetine and mirtazapine First line of treatment is to remove the offending agent(s) Specific inhibitors of 5–HT 2 have a role but paralysis and ventilation may be needed

Scenario An young girl was admitted to our toxicology after ingestion of 100 pills of AMLONG-AT

Beta-blockers Clinical features: CVS – bradycardia & hypotension, Respiratory – bronchospasm & pulmonary edema CNS depression Hypoglycemia Renal Failure ECG, blood sugar, electrolytes

Beta-blockers Brady – atropine 2 mg IV Hypotension – IVF Glucagon- 50 to 150 mcg/kg IV in 1 min and 1 -5 mg/hr in 5 D, (stimulate adenyl cyclase) Isoproterenol, Norepinephrine and Calcium chloride 10%(0. 2 ml/kg). Beta agonists - theophylline IV glucose, ventilation, dialysis for some, diazepam/phenytoin for seizures

Calcium channel Antagonists Bradycardia, AVblock, asystole, hypotension, pulmonary edema, hypocalcemia, hyperglycemia Gastric lavage and activated charcoal For SR tabs. - Gastroscopy/WB irrigation

Calcium channel Antagonists IV saline, dopamine 10% Cacl 10 -20 ml IV or Ca. gluconate drip(0. 6 ml/kg bolus & 0. 6 -1. 5 ml/kg IV infusion) Glucagon for Heart Block or hypotension Atropine/pacemaker Seizure control
 2) An young girl ingested 30 tablets of DAPSONE and presenting in")
Scenario 1) 2) An young girl ingested 30 tablets of DAPSONE and presenting in a stuporous state An young man presented after ingesting CELL OIL ( anti-termite liquid) developed cyanosis

Methemoglobinemia Caused by – nitrites, nitroprusside, NTG, chlorates, sulfonamides, aniline dyes, nitrobenzene, antimalarials and dapsone ---- Cell oil? (oxidation of ferrous hemoglobin to ferric form) Headache, fatigue, dyspnoea, cyanosis, hypotension >50% - CNS depression, arrhythmias. >70% - fatal Normal Pa. O 2 & cyanosis not responding to O 2, “chocolate brown” blood 100% O 2 , Lavage and charcoal Methylene blue 1 -2 mg/kg IV over 5 min repeat in 1 hr and 4 th hrly. To max. of 7 mg/kg (contraindicated G 6 PD deficiency patients) Hyperbaric O 2 and exchange transfusion

Scenario A famous personality was found unconscious after inhaling opioid compound with his friends. Two of them died at the spot. He was saved after shifting him to a famous private hospital.
 Purely synthetic –")
Opioids From poppy – morphine, codeine Semi-synthetic – Heroin (diacetyl morphine) Purely synthetic – meperidine, propoxyphene, diphnoxylate, fentanyl, buprenorphine, tramadol, methadone, pentazocine

Opioids Resp. depression, miosis, CNS , hypotension, brady. , pulmonary edema. No emesis, give lavage and charcoal, WBI Naloxone HCl – 2 mg IV initially or SL / IN / ET Ventilatory support

Scenario A recently married young girl was admitted in our toxicology after ingesting OIL OF WINTERGREEN 15 ml in an obtunded state with respiratory distress

Salicylates Toxicity – severe if >300 -500 mg/kg Nausea, vomiting, tinnitus, fits, coma and NCPE PT prolongation, hypoglycemia ABGs – early respiratory alkalosis and later metabolic acidosis. Fever and acidosis – poor prognosis

Salicylates Multidose charcoal / WBI FAD – watch for fluid overload Cerebral edema – hyperventilation and osmotic diuresis Seizures – diazepam, phenobarbital HD – refractory acidosis, CNS, PE, RF Mechanical ventilation – high Fi. O 2 and PEEP

Scenario A young boy was admitted after ingesting 40 tablets of GARDENAL which he was taking for his seizure control

ANTICONVULSANT POISONING Carbamazepine Phenytoin Barbiturates

Carbamazepine - Toxicokinetics Absorption Slow absorption Pharmacobezoar formation is common Carbamazepine decreases gastrointestinal motility Metabolised by inducible P 450 enzymes Enterohepatic circulation Half life 20 -65 hours normal adults 5 -17 hours epileptics

Carbamazepine - Clinical effects CNS disorientation, confusion ataxia dystonia athetosis drowsiness, stupor coma hyperreflexia hyporeflexia tremor seizures
 Nausea,")
Carbamazepine - Clinical effects Cardiovascular bradycardia hypotension heart block QRS prolongation (quinidine like) Nausea, vomiting Decreased bowel sounds Hypothermia

Carbamazepine - Treatment Supportive Lavage and charcoal Repeat doses of activated charcoal ECG monitoring (if ECG abnormal) Serial levels until falling level demonstrated No antidotes No effective elimination enhancement

Phenytoin - Toxicokinetics Delayed absorption Peak concentrations as late as 24 hours Protein binding 90% Ph dependent protein binding Metabolism zero autokinetics Saturable metabolism by P 450 enzymes Therapeutic half life 20 -30 hours Overdose half life 24 -230 hours

Phenytoin - Drug interactions that increase half life ethanol disulfiram imipramine diazepam cimetidine thioridazine valproate proproxyphene chlorpromazine ethosuximide

Phenytoin - Clinical effects CNS dilated pupils nystagmus - horizontal and vertical ataxia drowsiness coarse tremor clonus myoclonus hyperreflexia seizures (paradoxical intoxication)

Phenytoin - Clinical effects Cardiovascular bradycardia AV block direct myocardial depression VF asystole Nausea & vomiting Hyperglycaemia Hepatitis
 Hypotension - IV fluids Seizures - diazepam")
Phenytoin - Treatment Respiratory support (avoid acidosis) Hypotension - IV fluids Seizures - diazepam Heart block - atropine + pacemaker GI decontamination up to 12 hours post ingestion Elimination enhancement not usually helpful Serial levels required until falling

Barbiturates primidone phenobarbitone pentobarbitone

Barbiturates - toxicokinetics Rapid absorption Rapid onset of action Hepatic metabolism is predominant though phenobarbitone has significant renal elimination Many drug interactions Induces p 450 enzymes Synergistic CNS depression
 respiratory")
Barbiturates - Clinical effects CNS ataxia nystagmus dysarthria lethargy, confusion Areflexia (except pupillary) respiratory & cardiac depression Vasodilation, hypothermia Skin – ‘Barb bullae’ EEG may be iso-electric

Barbiturates - Treatment Respiratory support Intravenous fluids GI decontamination Serial doses of activated charcoal Forced Alkaline Diuresis (FAD) Haemodialysis Haemoperfusion Beware barbiturate withdrawal syndrome

Scenario An young male was working in a rehabilitation centre as a drug dispenser. He was found unconscious inside the pharmacy with diazepam tablets strewn around. He was suspected to have consumed >100 tablets.

Benzodiazepines

Benzodiazepines Fatalities rare Drowsy, dysarthrytic, ataxic, miosis, coma, resp. Lavage, activated charcoal Intubation – resp. depression Hypotension, bradycardia Flumazenil – reverse toxicity without Resp. depression, use with caution (during coingestion) 0. 2 mg(2 ml) IV in 30 secs, 0. 3 mg in 1 min interval for total dose of 3 mg or 0. 1 -

Scenario A 30 year old man presented after ingesting 40 tabs of chlorpromazine with severe hypotension, seizures and EPS

Antipsychotic Phenothiazines Chlorpromazine, fluphenazine, flupenthixol, Pimozide, thioridazine, trifluoperazine, zuclopenthixol Butyrophenones droperidol haloperidol

Newer Antipsychotics Atypical agents aripiprazole clozapine risperidone quetiapine amisulpride olanzapine

Antipsychotics Modes of action All anti-psychotic drugs have inhibitory effects on the D 2 receptor Some have actions against the D 4 receptor All have other effects - to varying degrees Serotonin 5 HT 2 blockade (may improve negative symptoms) Histamine H 1 blockade (drowsiness) Alpha adrenoceptor blockade (postural hypotension)

Antipsychotics Control the ‘positive’ features of the disease, but little effect on the ‘negative’ features clozapine may be superior in this regard The main side-effects are on the extrapyramidal motor system Akathisia (hours) Dystonias (hours to days) Parkinsonism (weeks to months) rigidity, tremor, and loss of mobility Tardive dyskinesia (months to years) Repetitive abnormal movements of face and upper limbs Thought to be due to proliferation of D 2 receptors in the striatum

Clinical effects - antipsychotics

Clinical effects - differences All effective antipsychotic drugs block D 2 receptors Chlorpromazine and thioridazine block α 1 adrenoceptors more potently than D 2 receptors block serotonin 5 -HT 2 receptors relatively strongly affinity for D 1 receptors is relatively weak Haloperidol acts mainly on D 2 receptors some effect on 5 -HT 2 and α 1 receptors negligible effects on D 1 receptors Pimozide and amisulpride

Toxic effects

Atypical antipsychotics Atypical antipsychotics have serotonin blocking effects as well as dopamine blockade As a group have less chance of extrapyramidal side effects Most have weight gain and insulin resistance as a side effect (except perhaps aripiprazole and maybe amisulpride) May be associated with stroke when used for behavioural control in dementia Many have idiosyncratic toxicities

Antipsychotics Pill concretions in stomach by radiographs Lavage, WBI. Lidocaine, phenytoin, noradrenaline, seizure control, dystonias – benztropine, benadryl – diphenhydramine Neuroleptic malignant syndrome Acidosis correction

Neuroleptic malignant syndrome Adverse, idiosyncratic drug reaction Mortality – 4 to 30% “akinetic hypertonic syndrome” Hyperthermia, tachycardia, muscle rigidity, altered mental status, akinesia Tachypnoea, diaphoresis, incontinence, sialorrhea, flushing Disruption of central dopamine neurotransmitter in nigrostriatal & hypothalamic thermoregulation Lab: leukocytosis, elevated creatine kinase Rx: heparin, dantrolene, bromocriptine, IV levodopa, benzodiazepines

Scenario A nursing student of our college was admitted after ingesting 45 tablets of deriphylline to our toxicology

Theophylline PDI’s, degradation of cyclic. AMP, enhance endogenous catecholeamine actions Nausea, vomiting, tachycardia, arrhythmias, tremors and agitation >90 mg/ml – severe intoxication cause hallucination, seizures and hypotension, rarely rhabdomyolysis-ARF ABGs, ECG, hypokalemia, hypophosphatemia, hypocalcemia, hyperglycemia

Theophylline Multidose charcoal, WBI – for SR preparations. Perinorm/ondansetron, dopamine/IVF Phenobarbital, diazepam is for seizures(No phenytoin) IV esmolal / propranolol – arrhythmias

ROLE OF NEPHROLOGIST IN POISIONING Drug removal Fluid & Electrolyte balance Acid - base disturbance Rx of ARF due to nephrotoxins

NEPHROLOGIC INTERVENTIONS Forced Alkaline diuresis Forced acid diuresis Peritoneal dialysis Hemoperfusion Exchange transfusion

FORCED ALKALINE DIURESIS PRINCIPLE Urine PH modulation causes ion trapping and decreases the renal reabsorbtion GOAL Maintain the urine PH around 7. 5 to 8. 5 urine flow rate of 300 to 500 ml

INDICATIONS FOR FAD Copper sulphate poisoning Phenobarbital >10 mg/dl Salicylate >50 mg/dl Chloropropamide Sulphonamides
 of Na. HCo 3 in 1000 ml D")
FAD Administer 100 meq (2 amps) of Na. HCo 3 in 1000 ml D 5/0. 45 saline at 10 -15 ml/kg/hr Maintain alkalinization – 2 -3 ml/kg/hr Monitor urine output(3 -6 ml/kg/hr), urine p. H(7 -8), K+ 20 meq of KCl is simultaneously administered Avoid vigorous correction in elderly

COMPLICATIONS of FAD Hyponatremia Water intoxication Pulmonary edema Alkalosis SECOND HOURLY MONITORING OF URINE p. H IS A MUST

ROLE OF DIALYSIS Clinical deterioration despite supportive care Severe intoxication presenting in the form of severe hypotension, hypothermia, hypoventilation Development of unconsciousness Development of cardiac, renal, hepatic dysfunction Toxins above critical blood levels
 across a semipermeable membrane (MW 500 D)")
Haemodialysis Blood is pumped (150 -300 ml/min) across a semipermeable membrane (MW 500 D) performed for 4 -8 hrs at a time (intermittent) Dialysis fluid infused countercurrent on the other side of the membrane establishing a concentration gradient Solutes diffuse across the membrane into the dialysate corrects uraemia and electrolyte / acid-base disturbances Anticoagulation is required (either systemic or of the circuit)

COMMON POISONS AMENABLE TO DIALYSIS Barbiturates Theophylline >40 mg/dl Paraqat 0. 1 mg/dl Trichloroethyelene >500 mg/dl Carbamazepine, valproic acid Primidone, ethosuximide Amphetamines, MAOI s Ethanol, ethyleneglycol, methanol Salicylates, paracetamol Amikacin, gentamicin, streptomycin INH, ethambutal, cycloserine Ranitidine Lithium

COMMON NON DIALYSABLE POISON Secobarbital Diazepam, Heroin TCAs, Amitryptylline Vancomycin Erythromycin, Chloramphenicol Chloroquine Azathioprine, Methotrexate Digoxin, Quinidine Organophosphates CCL 4, Eucalyptus oil

COMPLICATIONS OF HD Hypophosphatemia Alkalosis is disequilibrium syndrome Dialys
 through a column containing")
Haemoperfusion: Technique Blood is pumped (150 - 250 m. L/min) through a column containing an adsorbent, usually activated charcoal, coated with a biocompatible ultrathin® membrane

POISONS AMENABLE TO HEMOPERFUSON Carbamazepine Phenobarbitone Theophylline Meprobomate Phenytoin Sodium Valproate Salicylates

COMPLICATIONS OF HEMOPERFUSION Thrombocytopenia Hypocalcaemia Leucopenia Hypoglycemia Hypothermia Hypotension Bleeding

Hemoperfusion The limited data available suggests that: - there is a continuing role for c. HPF in severe theophylline & carbamazepine poisoning particularly in patients who are deteriorating despite MDAC or in those in whom MDAC use is limited by ileus Future developments in carbon technologies may allow an expansion in the indications for c. HPF in toxicology & increased efficacy

ROLE OF HEMOFILTRATION AV—pressure difference induces convective transport of solutes through hollow fiber / flat sheet Removes molecules </= to 40, 000 Blood is pumped through the filter Can be done intermittently at 6 L/hr OR continuously at 100 ml/hr
 Haemodiafiltration can be achieved by infusing dialysis fluid countercurrent to")
Haemofiltration & haemodiafiltration (CVVHF) Haemodiafiltration can be achieved by infusing dialysis fluid countercurrent to the membrane allowing diffusive solute removal by dialysis in addition to the convective removal by filtration CVVHF (CVVHDF) CVVHDF allows greater removal of smaller molecules (<500 D) and also better control of hyperkalaemia and other metabolic disturbances (CUPID = combination of CVVHF and intermittent

DRUGS AMENABLE TO HEMOFILTRATION AMINOGLYCOSIDE antibiotics METAL CHELATE complexes of ALUMINUM or IRON DESFEROXAMINE

ADVANTAGES OF HF Consistent homeostasis No hypotension---no disequilibrium No need to restrict fluid administration Less amount of extracorporeal blood No effect on complement or leukocytes USEFUL in clearance of mid –molecular weight substances

DISVANTAGES OF HEMOFILTRATION Anticoagulation is needed Vascular access complication LOWER clearance of LOW MOLECULAR Wt. solutes

PLASMAPHERESIS SEPERATES CELLULAR BLOOD COMPONENTS FROM PLASMA EFFICACY DEPENDS ON NUMBER OF CYCLES SACRIFICES PATIENTS OWN PLASMA

DRUGS AMENABLE TO PLASMAPHERESIS Vincristine Inorganic mercury Amanita Theophylline ATG Digoxin antibody complexes Phenytoin Dapsone Carbmazepine

PLASMA EXCHANGE & EXCHANGE TRANSFUSION Highly protein bound drugs Exchange transfusion is useful in poisons with intense hemolysis HD+HP +Chelation is useful in metal poison like mercury, thallium

ROLE PERITONEAL DIALYSIS Not an acceptable substitute to HD Peritoneal dialysis—slow removal poisons NEVER USED IN DRUG OVERDOSE & POISONING

Conclusions For most severely poisoned patients supportive care is all that is necessary and extracorporeal techniques are indicated in only a limited number of poisonings Haemoperfusion - Carbamazepine, theophylline, phenobarbitone Haemodialysis - Salicylates, alcohols, (theophylline), lithium Haemofiltration - ? Lithium, alcohols - Correction of electrolyte disturbances or lactic acidosis and for renal support - Aminoglycosides, removal of iron-DFO in patients

Antidotes Antidote N-acetyl cysteine Ethanol/Fomepizole Oxygen/hyperbarics Naloxone/nalmefene Physostigmine Nitrates Glucagon Sodium Bicarbonate Calcium/insulin/dextrose Dextrose/glucagon Indication Acetaminophen Methanol/Ethylene glycol Carbon monoxide Opioids Anticholinergics Cyanide Beta-blockers TCA’s CCB’s Oral hypoglycemics

- Slides: 128