Drug dosing safety in obese children Workshop aims

Drug dosing safety in obese children

Workshop aims 1. Drug dose adjustment for children with obesity: Methods to improve safety and cost. 2. The crucial role of obesity screening on admission to hospital.

Child obesity: What are the problems?

Child obesity: What are the problems? §Obesity in children quadrupled between 1974 and 2004 § 26% obesity rate in inner city areas §Surgical admissions: twice as likely to be obese?

BMI distribution: Year 6 children National Child Measurement Programme 2010/11 © NOO 2012

Child obesity: What are the problems? § Multiple co-morbidity ▪ OSA/ asthma/breathing difficulties ▪ Diabetes ▪ Orthopaedic problems ▪ Fatty liver infiltration § Shortened life expectancy in child obesity, independent of other factors

NEJM 2010 13 § 1. 5 million adult non smokers, median age 58 § 10 year follow up § 160, 000 deaths §mortality lowest for BMI 20 -25 §obese 1. 5 x mortality §morbidly obese 2. 5 x mortality

Lancet 2009 16 §Life expectancy 8 -10 years shorter if morbid obesity develops in middle age 16

Child obesity: What are the problems? ▪ High rate of tracking of obesity in children into adulthood ▪ Double the risk of airway and respiratory complications during anaesthesia 1 -7

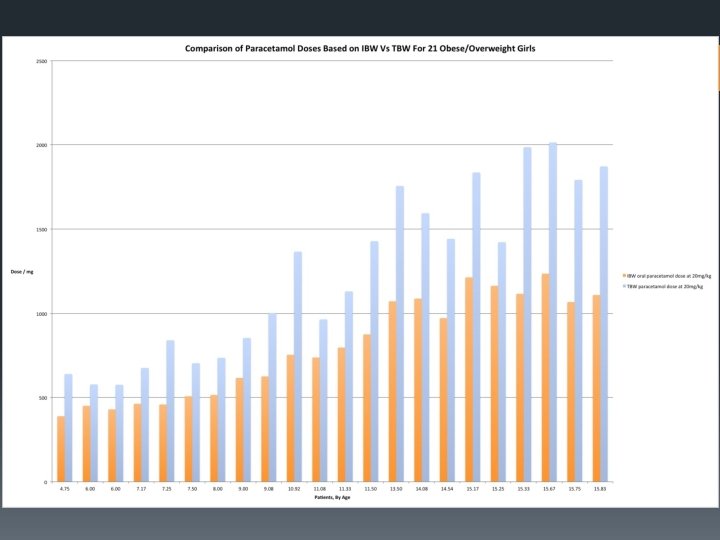
Child obesity: What are the problems? ▪ Risk of drug overdose if total body weight used to calculate doses 8 -11 ▪ Lean body mass (LBM) and ideal body weight (IBW) recommended as alternatives, depending on drug 8, 9 ▪ Deaths and morbidity attributed to overdose

Child obesity: What are the problems? § How should we calculate drug dosage in obese children? § total body weight (TBW) and potential for over-dosing 11 § ideal body weight (IBW) and potential for under-dosing 11 § BNF for children: “Use an ideal weight for height”

Using known problems to guide safety improvement §How to detect cases of obesity § Visual inspection vs BMI screening § Benefits: § Alerting systems § Drug error monitoring §How to prevent drug dosing confusion and overdose risk § Calculating IBW and LBM § Nomogram: Simplicity and accuracy

Obesity Definitions • UK healthcare Cut-offs: 91 st centile/ 98 th centile • UK Epidemiological Cut-offs: 85 th/95 th centiles) • Morbid or Very Severe Obesity: 3. 5 SD • IOTF Cut-offs: bold curves

Childhood Obesity Definitions Very severe/ morbid obesity: 3. 5 SD Origins: Cole et al Obesity =98 th centile 2 SD Ideal BMI =50 th centile, longest life expectancy

BMI Screening §Why is it necessary? § gross underestimation of weight status by carers §how do we prevent and audit dosing errors unless we screen?

Visual Assessment of obesity is a grossly inadequate screening tool

Approximate ideal BMI between age 2 -11 yrs is 16 kg/m 2 (vs 22 in adults)

Hospital Admissions: Are we screening for obesity? §Audits in 3 hospitals: total of 6 months worth of admissions §Zero rate of obesity screening Reasons? §Time, complexity § 82% lacked height measurement

Screening allows us to: §Alert the wider care team of presence of obesity as a risk factor for overdose §Review prescribing practises and monitor drug dosing errors §Avoid disasters

Using known problems to guide safety improvement §How to detect cases of obesity § Visual inspection vs BMI screening § Benefits: § Alerting systems § Drug error monitoring §How to prevent drug dosing confusion and overdose risk § Calculating IBW and LBM § Nomogram: Simplicity and accuracy

Dose adjustment §Kendrick et al 2010, 2015 §Ingrande and Lemmens 2010, 2013 §Dose adjustment is necessary. HOW? §TBW, IBW, LBM, ABW, BSA

Dose adjustment §Problems: • Widespread guesswork • Confusion over terminology: IBW, LBM, ABW • Ignorance and use of TBW • Small minority say they use ideal weight or lean weight • How are they deriving these?
 body weight (TBW) § Lean body mass (LBM)")
Drug Dosing Scalars § Total (actual) body weight (TBW) § Lean body mass (LBM) § Measurable concept § Fat free mass § Ideal body weight (IBW) § Non-measureable concept § Longest life expectancy § Adjusted body weight (ABW)

Which dosing scalar? §Lack of studies in obese children: some data is extrapolated from adults §Constantly needs updating §Many more studies needed

Drug Loading/ induction dose Maintenance /infusion dose Propofol 8 ? LBM TBW Thiopentone 8 LBM Fentanyl 8 LBM Remifentanil 8 ? LBM Suxamethonium 8 TBW Non depolarising muscle relaxants 8 IBW Lignocaine ? TBW LBM

Drug Loading/ induction dose Etomidate 8 LBM Sugammadex 12 TBW Morphine 12 ? LBM IBW Phenytoin 10 IBW Vancomycin 11, 18 TBW (monitor) Paracetamol ? LBM Gentamicin 19 ABW * *adjusted body weight: ABW=IBW+0. 4(TBW-IBW) Maintenance/in fusion dose

Lean body mass §LBM is child minus the adipose tissue §Measureable §No nationally agreed method §LBM is always > IBW in obesity

Lean tissue gain in obesity Obese children taller than non obese More muscle/ lean/ bone Increased organ size 25 -40% of excess weight, above IBW, is lean tissue • Mean 29% • Increased cardiac output • Lean tissue reaches limit (severe obesity limits mobility) • •
 5 §MRI §Hydrodensiometry 5 §Whole body 40")
LBM measurement §Dual energy X-ray absorptiometry (DXA) 5 §MRI §Hydrodensiometry 5 §Whole body 40 K spectrometry 5 §Multiple skinfold anthropometry (MSA) §Bioelectrical impedance analysis (BIA) §Extracellular volume method 17 e. ECV = 0. 0215 weight(kg)0. 6469 height(cm)0. 7236 e. LBM = 3. 8 e. ECV

Lean body mass §Obese children are not just lean children with extra fat § 20 -40% (mean 29%) of an obese child’s increase in weight is lean tissue 2, 6, 21, 22 §LBM= IBW + 0. 29 (TBW-IBW) 1, 2, 3, 6, 12

Ideal Body Weight Calculation §IBW is the weight associated with longest life expectancy, corrected for height § 50 th centile age/gender specific from pre-1990 data §BMI chart method: 1, 2, 3, 12 (BMI at 50 th centile for age) x (height)2

IBW Outdated methods: • • 50 th centile on weight vs age growth chart Moore method Mclaren method (Age +4) x 2

Ideal body weight: BMI chart method 1. Obtain appropriate BMI chart 2. Take BMI at 50 th centile for child’s age This is the ‘Ideal’ BMI 3. Convert Ideal BMI to IBW: IBW (kg)= ideal BMI x height (m)2
 x 2 underestimates IBW")
Ideal Body Weight (Age +4) x 2 underestimates IBW

Example 12 years 96 kg 1. 6 m BMI 37 TBW 96 kg LBM 61 kg Ideal BMI x height 2 LBM= IBW+0. 29(TBW-IBW) IBW 46 kg
 § Height")
Example: Boy age 4 § Weight 32 kg (paracetamol dose 640 mg) § Height 1. 12 m § +4 SD § IBW 19 kg (paracetamol dose 380 mg) § LBM 23 kg (paracetamol dose 460 mg)
= ideal BMI x height (m)2 §LBM (kg)= IBW + 0. 29 (TBW-IBW)")
§IBW (kg)= ideal BMI x height (m)2 §LBM (kg)= IBW + 0. 29 (TBW-IBW)

50 th BMI centile plot and fitted curve. Courtesy of Child Growth Foundation
 x height")
Ideal BMI=ideal weight/height 2 So: IBW=Ideal BMI x height 2 Or IBW=f(age) x height 2

IBW/ LBM calculator: The Callaghan- Walker Nomogram

Callaghan LC and Walker JD. An aid to drug dosing safety in obese children: development of a new nomogram and comparison with existing methods for estimation of ideal body weight and lean body mass. Anaesthesia 2015; 70: 176– 182. doi: 10. 1111/anae. 12860

Nomogram Validation Results § The nomogram was: • as accurate as the current recommended calculation method (nomogram bias = -0. 04 kg, reverse BMI bias 0. 04 kg) • quicker to use (P = 0. 003) • Nomogram less likely to yield a calculation mistake (3 mistakes vs 18, P= 0. 001).

Reverse BMI method o Nomogram method Errors and mistakes compared using Bland-Altman plot

Errors and mistakes compared using Bland-Altman plot

IBW/ LBM calculator: under fives

Potential Cost savings §Growth hormone § 54 patients >+2 SD §£ 23 per mg §£ 700, 000 per year at TBW §£ 483, 000 per year at IBW §£ 217, 000 saved

Workshop summary Safety risks and barriers to drug dosing safety for obese children: § Overdose risk § morphine, fentanyl, paracetamol, gentamicin § Dosing scalars and dose adjustment § Confusion, ignorance and guesswork § Lack of screening

Conclusions: improving safety in the perioperative care of obese children ▪ Implement Screening by BMI: ▪ which children are obese? ▪ calculate BMI centile for all admissions (height necessary!) ▪ Design and implement an alerting system ▪ Pass the information on during the perioperative journey ▪ standard alerting system e. g. drug chart warnings ▪ Staff fore-warned of risks ▪ perioperative airway obstruction/ respiratory incidents ▪ cautious dosing of harmful drugs.

Conclusions: improving safety in the perioperative care of obese children ▪ Prevent overdose and underdose: ▪ the body mass nomogram: ▪ safer alternative to guesswork for prescribers which is a quick, easy and accurate way to modify doses in obesity ▪ Begin with drugs which cause respiratory side effects and organ damage: § E. g. opioids, paracetamol and gentamicin ▪ Quantify outcomes, dosing errors and costs attributable to obesity

The next steps: § Bariatric surgery in children? § Apps/ electronic prescribing § BNFc § More individual drug research in paediatric obesity

References 1. 2. 3. 4. 5. 6. 7. Veyckemans F. Childhood obesity and anaesthetic morbidity. Current Opinion in Anaesthesiology 2008; 21: 308 -312. Smith HL, Meldrum. DJ, Brennan LJ. Childhood obesity: a challenge for the anaesthetist? Paediatric Anaesthesia 2002; 12: 750 -761. Brenn BR. Anaesthesia for paediatric obesity. Anaesthesiology Clin N Am 2005; 23: 745 -764. Binks A, Pike M. Anaesthesia in the obese patient. Anaesthesia and Intensive Care Medicine 2008; 9(7): 299 -302. Campannozzi A, Dabbas M, Ruiz JC, Ricour C, Goulet O. Evaluation of lean body mass in obese children. European Journal of Pediatrics 2008; 167: 533 -540. Boer P. Estimated lean body mass as an index of normalisation of body fluid volumes in humans. Am J Physiol Renal Physiol. 1984; 247: 632 -636 Tait AR, Voepel-Lewis T, Burke C, Kostrzewa A, Lewis, I. Incidence and risk factors for perioperative adverse respiratory events in children who are obese. Anesthesiology 2008 ; 108(3): 375 -80

References 8. 9. 10. 11. 12. 13. 14. Ingrande J, Lemmens HJM. Dose adjustments of anaesthetics in the morbidly obese. Br J Anaesth 2010; 105(suppl): i 16 -i 23. Green B & Duffell SB. What is the best size descriptor to use for pharmacokinetic studies in the obese? Br J Clin Pharmacol 2004; 58(2): 119 – 133 Dosing dilemmas in obese children. Mulla H, Johnson TN. Arch Dis Child Educ Pract Ed 2010; 95: 112 -117 Pharmacokinetics and drug dosing in obese children. Kendrick JG, Carr RR, Ensom MHH. J Paediatr Pharmacol Ther 2010; 15(2): 94 -109 Anesthetizing the obese child. Mortensen A, Lenz K, Abildstrom H. Paediatr Anaesth 2011; 21: 623 -629 Berrington de Gonzalez B, Hartge P, Cerhan JR et al. Body-Mass Index and Mortality — Prospective Analysis of 1. 46 Million White Adults. Dec. 2, 2010, NEJM, Vol. 362, No. 23. Cole TJ, Freeman JV, Preece MA. Body mass index reference curves for the UK, 1990. Arch Dis Child 1995; 73(1): 25 -29. Assessment of childhood obesity in secondary care: OSCA consensus statement Arch Dis Child Educ Pract Ed 2012; 97: 3 98 -105

References 15. Prospective Studies Collaboration. Body-mass index and causespecific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet 2009; 373: 1083– 96. 16. Peters AM, Snelling HLR, Glass DM, Bird NJ. Estimation of lean body mass in children. British Journal of Anaesthesia 2011; 06(5): 719 -23. 17. Eiland LS, Kalyani BS. Vancomycin dosing in healthy weight, overweight and obese pediatric patients. J Pediatr Pharmacol Ther 2014; 19(3): 182 -188 18. Sampson MR, cohen-Wolkowiez M, Benjamin JR, Caparelli EV, Watt KM. Pharmacokinetics of antimicrobials in obese children. Ga. BI J 2013; 2(2): 76 -81 19. Kendrick JG, Carr RR, Ensom MHH. Pediatric obesity: Pharmacokinetics and implications for drug dosing. Clin Ther 2015; 37(9): 1897 -1923 20. Forbes GB, Welle. Int J Obesity 1983; 7(2): 99 -107 21. Wells JCK, Fewtrell MS, Williams JE, Haroun D, Lawson MS and Cole TJ. Body composition in normal weight, overweight and obese children. Int J Obesity 2006; 30: 1506 -1513

Thank you
- Slides: 55