Dr Chit Saing MBBS MMed Sc FRCPE MRCPI

Dr Chit Saing MBBS, MMed. Sc, FRCPE, MRCPI, Dip. GUM, DFSRH, Dip. HIV Consultant in Sexual Health & HIV Medicine Lincolnshire Community Health Services NHS Trust 10/03/2016 Updates on HIV

Outline �Short quiz �Burden of problem �Challenges �Risk assessment �HIV testing in primary care �Indicator conditions �HIV treatment and prognosis �HIV prevention �Future direction

Which of the following from untreated HIV patient are infectious? �Blood/serum √ �Pre-cum √ �Vaginal fluid √ �Saliva Χ* �Urine Χ �Rectal fluid √ �Faeces Χ* �Joint (synovial) fluid Χ* �CSF (Cerebro-Spinal Fluid) √ �Tear Χ �Sweat Χ �Breast milk√ *infectious if mixed with blood

HIV can be acquired through � Receptive vaginal sex with untreated patient High risk � Unprotected insertive anal sex with known HIV positive patient with undetectable HIV viral load on treatment Negligeble risk � Oral sex (unprotected) Low risk � Lesbian sex Negligeble risk � Human bites Negligeble risk � Pre-chewed food Negligeble risk � Kissing Negligeble to Low risk � Tattooing/body piercing Low to medium risk � Semen splash to eye Low risk � Needle stick from a discarded needle in the community Negligeble risk
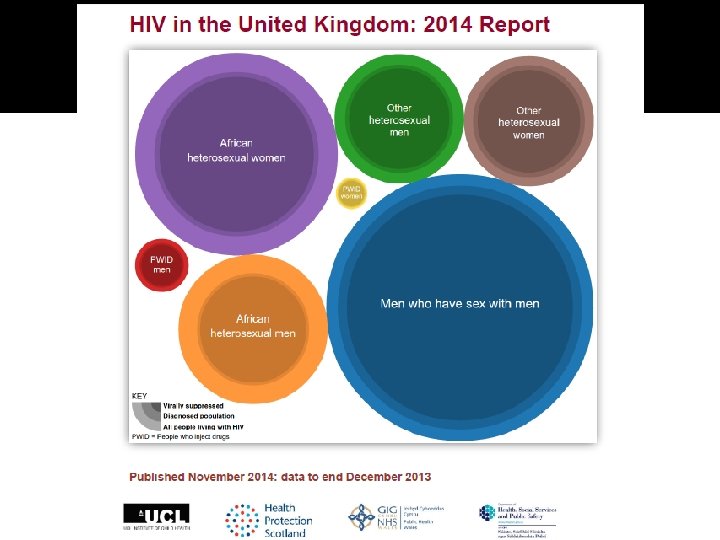

HIV in Lincolnshire �~ 200 registered patients �Boston, Lincoln, Grantham, Skegness �male>female �Mostly UK (NB Boston) �Many undisclosed MSM �Women diagnosed late �Most on antiretroviral therapy �Most good adherence
 �Late diagnosis (≈ 55% among heterosexuals")
Challenges �Undiagnosed (≈ 17% in UK - 2014) �Late diagnosis (≈ 55% among heterosexuals in UK – 2014) �Stepping up treatment HIV care continuum target – ‘ 90 -90 -90’ in 2020 (UNAIDS) �HIV prevention �HIV stigma reduction

https: //www. gov. uk/government/uploads/system/uploads/attachment_data/file/477702/HIV_in_the_UK_ 2015_report. pdf

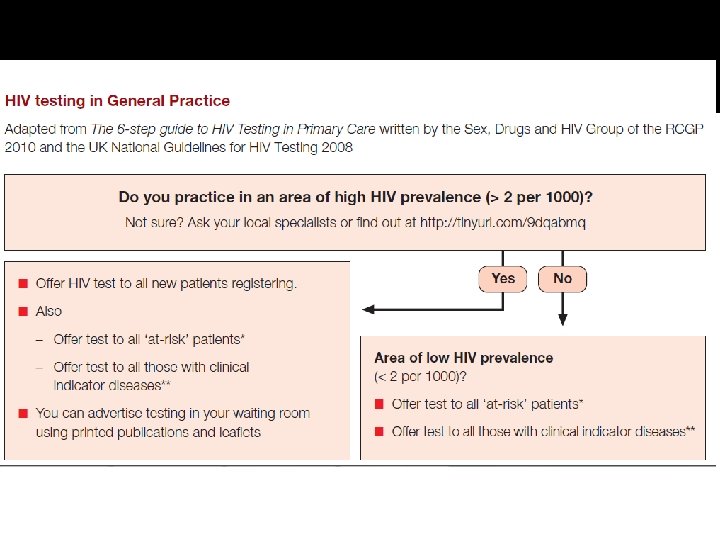
What is the single most important intervention to tackle the HIV epidemic? HIV TESTING

 has transformed treatment of HIV infection Eviplera Atripla")
Why HIV testing? �Antiretroviral therapy (ART) has transformed treatment of HIV infection Eviplera Atripla Genvoya Stribild Triumeq

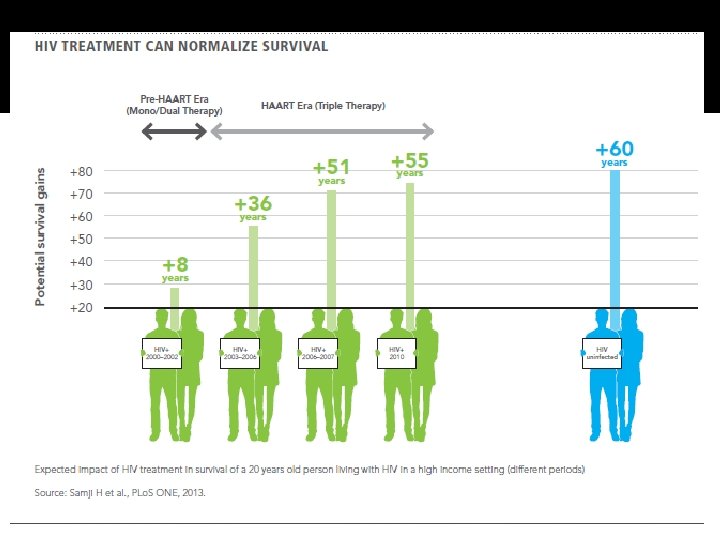
Why HIV testing? �The benefits of early diagnosis of HIV are well recognized – not offering HIV testing represents a missed opportunity Earlier treatment ▪ Reduced AIDS and non-AIDS morbidities and mortalities ▪ Reduced HIV transmission Earlier institution of preventative measures ▪ Reduced HIV transmission ▪ Public health benefits Improved QOL Cost-effectiveness and economical gain in the longer term

Why HIV testing? � Over 25% of HIV-positive individuals remain undiagnosed, accounting for 54 – 70% of transmission

Why HIV testing? � 39% of HIV-positive heterosexuals are not diagnosed until their CD 4 cell count falls below 200
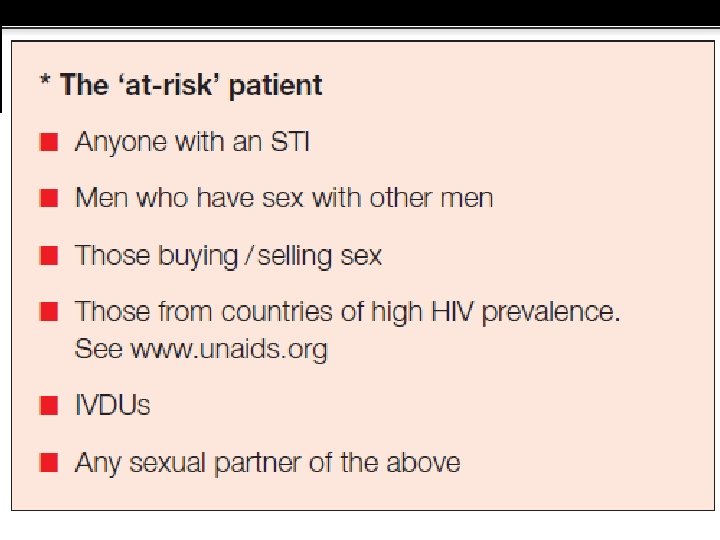
 Benefits of testing �Risk assessment, prepare")
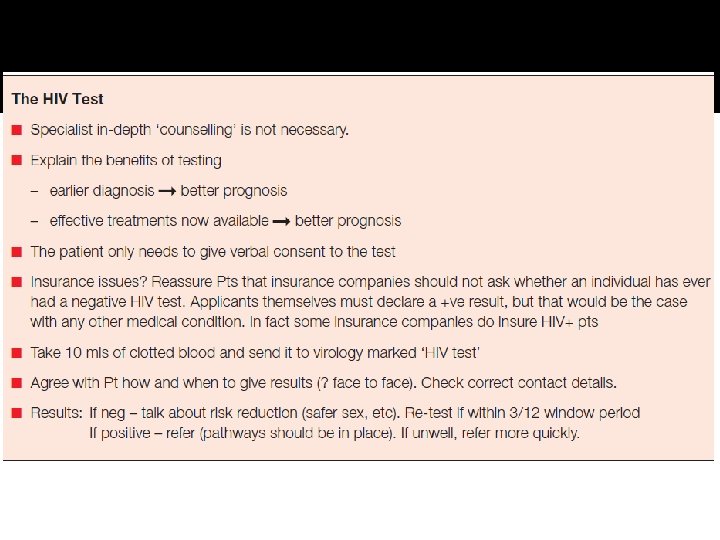
Pre-Test Discussion �Informed consent (written consent not required) Benefits of testing �Risk assessment, prepare for positive diagnosis, health promotion, partner notification �Explain confidentiality Explore attitudes, how to get result
 �Reducing future risks Risk reduction/behavioral changes Other preventive measures (Pr. EP,")
Post-Test Discussion (negative) �Reducing future risks Risk reduction/behavioral changes Other preventive measures (Pr. EP, PEP) �Future testing Window periods �Equivocal results ? seroconvertion/? false positive results
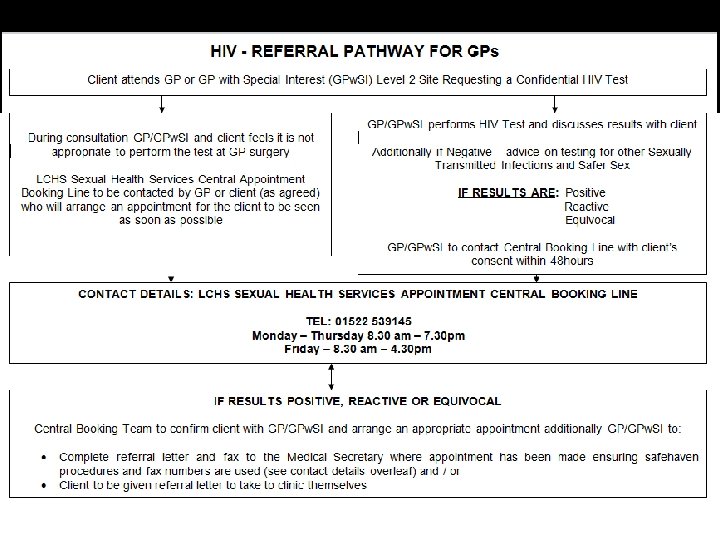
 �Face-to-face confidential environment Non-judgemental �Confirmatory testing �Appropriate, timely ongoing referral Ensure")
Post-Test Discussion (positive) �Face-to-face confidential environment Non-judgemental �Confirmatory testing �Appropriate, timely ongoing referral Ensure all confirmed positive cases are seen urgently by HIV specialist team
 � Key issues HIV vs. AIDS Good prognosis Availability and effectiveness")
Post-Test Discussion (positive) � Key issues HIV vs. AIDS Good prognosis Availability and effectiveness of ART Can lead normal life with appropriate care Support available for patients and families (including counseling services) Specialist HIV care team Better off knowing that their HIV status than not knowing � Formal HIV partner notification Better addressed by HIV clinic � Other concerns/issues (as raised in pre-test discussion)

What if patient doesn’t attend for result? �Proper procedure should be in place to maximise follow-ups to collect results �Do your best to contact the patient using all available means (particularly for positive results) �If all your means to contact the patient are exhausted, seek advice from your local HIV specialist team
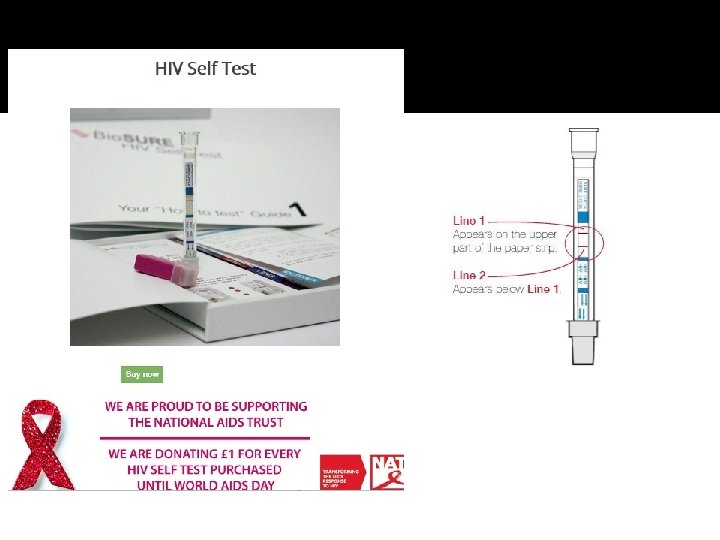
 Tests (POCTs) Alere Combo HIV-1/2 Rapid POCT System Oraquick In-Home")
Point of Care (Rapid) Tests (POCTs) Alere Combo HIV-1/2 Rapid POCT System Oraquick In-Home HIV Test Pasante Insti HIV-1 and HIV 2 POC Rapid Antibody Test

HIV POCT � Indications Rapid turn around of results desirable Community testing (high prevalence areas) Urgent source testing (exposure incidents) Refusal of/difficult venepunctures � Advantages Quick to get results; ease of use (finger prick, oral swab) � Disadvantages Reduced sensitivity and specificity Reactive results needs confirmation using standard lab assays Quality assurance essential
 tests Enzyme Immunoassay (EIA) – 3 rd and 4")
Clinic-based HIV testing �Screening (initial) tests Enzyme Immunoassay (EIA) – 3 rd and 4 th generations Chemiluminescent Immunoassay (CIA) �Confirmatory (supplemental) tests Western blot Indirect immunofluorescence assay (IFA) Qualitative HIV-1 RNA HIV pro-viral DNA

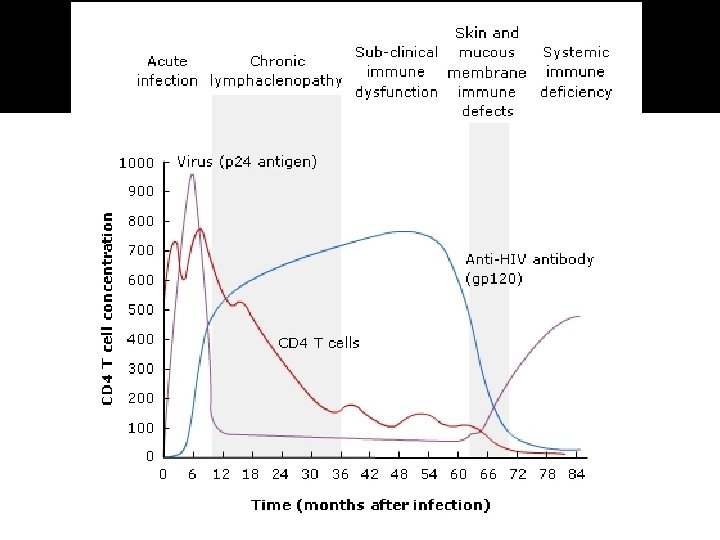
Goal of anti-retroviral therapy � The clinical goal Extend life expectancy and QOL in HIV-positive individuals � The virological goal Reduce HIV viral load to the lowest level possible for as long as possible to prevent disease progression, as well as limiting resistance to ARV drugs � The immunological goal Restore and preserve immunological function, by maintaining CD 4 cell counts and resisting infection by opportunistic pathogens � The epidemiological goal To reduce transmission of HIV to others

HIV lifecycle
 Tenofovir, Abacavir, Zidovudine, Lamivudine, Emtricitabine")
Anti-retroviral drug classes � Nucleoside Reverse Transcriptase Inhibitors (NRTI) Tenofovir, Abacavir, Zidovudine, Lamivudine, Emtricitabine � Non-nucleoside Reverse Transcriptase Inhibitors (NNRTI) Efavirenz, Nevirapine, Etravirine � Protease Inhibitors (PI) Darunavir, Atazanavir, Lopinavir, Ritonavir � Integrase Inhibitors (INSTI) Raltigravir, Elvitegravir, Dolutegravir � Entry Inhibitors Maraviroc (CCR 5 antagonist) Enfuvirtide (Fusion inhibitor)
 � Risk reduction measures Condoms provision OST, needle and syringe")
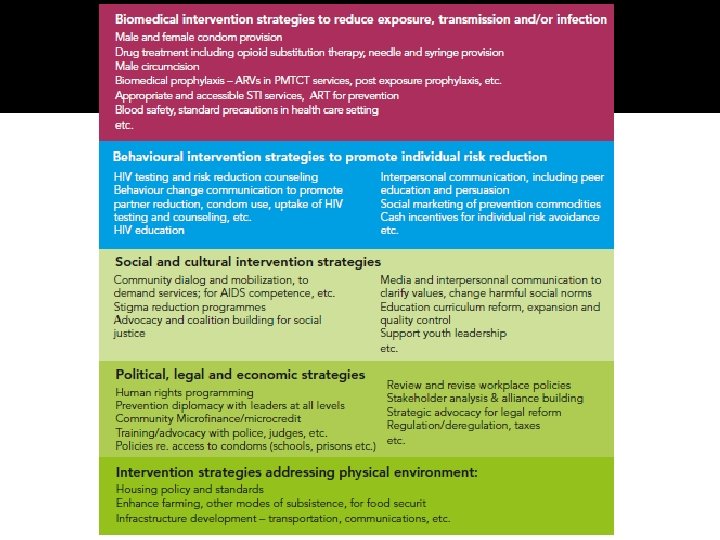
HIV prevention (biomedical interventions) � Risk reduction measures Condoms provision OST, needle and syringe provision Male circumcision � STI diagnosis and treatment � ART as prevention Early diagnosis and treatment of HIV ▪ Tas. P (Treatment as Prevention) ▪ HPTN 052 – 93% reduction in HIV transmission with early ART ▪ Partner study – no transmission with undetectable viral load (gay or heterosexual) PEP (Post-exposure Prophylaxis) Pr. EP (Pre-exposure Prophylaxis) ▪ PROUD (UK) and IPERGAY (France) – 86% reduction in HIV acquisition with Truvada ▪ Caprisa 004 (SA) – 39% reduction in HIV and 51% reduction in HSV transmission

Future direction �Newer agents/classes and formulations Newer agents from existing classes Maturation inhibitors (Bevirimat, BMS-955176) Long-acting injectables (Rilpivirine + Carbotegravir) �HIV vaccines/immunologicals HVTN and RV 144 (Thailand) Therapeutic vaccines Broadly neutralising Mab Adoptive immunotherapy

Future direction �HIV cure research Berlin patient!!/Mississippi child? ? Stem cell transplantation LRAs/TLR 7 agonists and HIV eradication (shock- and-kill) Gene therapies �Combination approaches HIV managed in primary care!!!

Summary �Wary the undiagnosed �Multidisciplinary approach to HIV testing and prevention Primary care Secondary care Community/outreach �Stepping up HIV treatment UNAIDS targets to end HIV epidemic �HIV stigma and discrimination shared responsibility Crucial intervention to achieve AIDS-free generation

Useful Websites �www. bashh. org �www. bhiva. org �https: //www. gov. uk/government/organisatio ns/public-health-england �www. medfash. org. uk �www. clinicaloptions. com �www. aidsmap. com �www. hivinsite. com �www. stif. org. uk
- Slides: 43