Doppler of the Uterine And Umbilical Arteries Clinical

Doppler of the Uterine And Umbilical Arteries: Clinical Significance Greggory R. De. Vore MD

Part I: The Use of the Umbilical Artery Doppler in High- and Low-Risk Patients

Historical Perspective First use of Doppler ultrasonography to study flow velocity in the fetal umbilical artery was reported in 1977 Fitzgerald and Drumm. Non-invasive measurement of human circulation using ultrasound: a new method. BMJ 1977, 2: 1450


Historical Perspective Observational Studies: 4 Association between reduced enddiastolic umbilical artery velocities and increased vascular resistance in the fetoplacental circulation

Historical Perspective Observational Studies: 4 Complications of pregnancy associated with placental pathologic mechanisms 4 Adverse pregnancy outcome including perinatal death

Historical Perspective Other Doppler Studies: 4 Uterine arteries 4 Middle Cerebral arteries 4 Venous system

Historical Perspective Benefit of Umbilical Artery Evaluation 4 Less experienced operators can achieve highly reproducible results with simple, inexpensive continuous-wave equipment

Historical Perspective Problem With Observational Studies 4 Observations are often rushed into clinical practice only to find later that they are either ineffective or even harmful

Historical Perspective Randomized Controlled Trials 4 “Gold Standard” for evaluating the effectiveness of clinical investigations in the human population 4 “Meta Analysis” combines the results from smaller trials of similar structure and purpose.

Historical Perspective Randomized Controlled Studies 4 Doppler ultrasonography has been subjected to more rigorous and extensive assessment by randomized controlled trials than any previous test of fetal health or fetalplacental function

Meta-Analysis In High-Risk Pregnancies Doppler Ultrasonography in High-Risk Pregnancies: Systematic Review With Meta-Analysis Alfirevic Z and Neilson JP Doppler ultrasonography in high-risk pregnancies: Systematic review with meta-analysis Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis Studies Included In Analysis n n n Trudinger et al 1987 Mc. Pharland et al 1988 Hofmeyr et al 1991 Newham et al 1991 Burke et al 1992 Almstrom et al 1992 n n n Biljan et al 1992 Johnstone et al 1993 Pattison et al 1994 Neales et al (Unpublished) Nienhuis (Unpublished) Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis Number Evaluated 7, 474 Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis Absent End-Diastolic Flow 5. 6% Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis: Results Perinatal Deaths 4 Clinical action guided by Doppler ultrasonography reduced the odds of perinatal death by 38%, with a 95% confidence interval of 15% to 55% 4 10 of 12 studies demonstrated a reduction in death compared to controls Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis: Results Antenatal Care and Labor 4 Reduction in antenatal admissions 4 Reduction in inductions of labor 4 Reduction of cesarean section for fetal distress during labor Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis: Results Neonatal Outcome 4 No effect on perinatal morbidity 4 No difference in birth weight Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis: Results Other Outcomes 4 Reduction of 16% in the number of elective deliveries 4 Reduction of 31% of fetal distress during labor 4 Reduction of 87% of hypoxic encephalopathy Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis: Conclusions Should additional studies be ethically done in light of the current results? Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

High-Risk Meta-Analysis: Conclusions It is likely that, on the basis of available information, parents with high-risk pregnancies may not wish to enter their babies in further trials and deny them the possibility of investigation by a test that clearly increases their chance of survival. Alfirevic Z and Neilson JP Am J Obstet Gynecol 1995, 172: 1379

Randomized Controlled Trial In Low-Risk Pregnancies A Randomized Controlled Trial of Doppler Ultrasound Velocimetry of the Umbilical Artery in Low-Risk Pregnancies Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Historical Perspective Studies in unselected low-risk patients have not been conclusive. Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Historical Perspective In France the use of the umbilical artery Doppler in high -risk pregnancies is accepted and widespread. Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Historical Perspective There has been a trend toward the extension of its indications, especially at the time of early third trimester ultrasonography Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Historical Perspective For this reason, a multicenter randomized trial to evaluate the benefits of umbilical Doppler performed between 28 and 34 weeks of gestation in a population of low risk women Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods All normal women between 28 and 34 weeks of gestation were asked to participate in the study Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods Women Excluded For: 4 Medical history of hypertension 4 Medical history of diabetes 4 Obstetric history of fetal death 4 History of IUGR 4 Women who had undergone umbilical artery Doppler before 28 weeks Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods Study Design: 4 Time of the Study: 1988 -1990 420 Antenatal Clinics throughout France 4 Control group: No Doppler studies 4 Doppler group: Results of Doppler conveyed to physicians Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods Assessment of Pregnancy Care 4 Number of antenatal visits 4 Days of antenatal hospitalization 4 Cardiotocography measurements 4 Rate of pregnancy induced hypertension Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods Assessment of Pregnancy Care 4 Rate of pre-eclampsia 4 Rate of uterine bleeding 4 Rate of oligiohydramnios 4 Rate of IUGR Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods Neonatal Assessment 4 Peri- and neonatal death 4 Rate of fetal distress 4 APGAR scores 4 Neonatal resuscitation 4 Neonatal transfer 4 Birthweight Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Methods Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Results Effects of Umbilical Artery Doppler 4 No increase in antenatal hospitalizations 4 No effect on the incidence of obstetrical complications 4 Did not influence preterm delivery 4 Did not influence mode of delivery Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Results Effects of Umbilical Artery Doppler 4 No difference in fetal distress during labor 4 THERE WERE THREE TIMES FEWER FETAL DEATHS IN THE DOPPLER GROUP (Larger study size would have resulted in statistical significance) Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Conclusions Effects of Umbilical Artery Doppler 4 No benefit to umbilical artery in low -risk patients Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Low-Risk Suggestions If Doppler is available, I would suggest using it for the following reasons: 4 It may identify a fetus with IUGR who registers later and you are uncertain of the gestational age Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Suggestions Low-Risk Population 4 May result in the discovery of high -risk patients who are unsuspected clinically 4 May identify patients at risk for toxemia Doppler French Study Group Br J Obstet Gynecol 1997, 104: 419

Part II: The Use of Uterine Artery Doppler

Review Anatomy n n n Blood supply provided by the ovarian and uterine arteries Uterine Arteries: main branches of the internal iliac arteries Uterine Arteries: Ascend through the lateral wall and anastomose with the ovarian arteries

Review Anatomy n n n Arcuate Arteries: Run Circumferentially around the uterus Uterus: Blood supply to anterior and posterior walls provided by the Arcuate arteries Radial Arteries: Extend from the arcuate arteries and enter the endometrium

Review Anatomy n n Spiral Arteries: 100 connect the maternal circulation to the endometrium Responsible for a 10 fold increase in blood flow

Review Anatomy n. Two waves of trophoblastic invasion: First trimester and second trimester n. Conversion of small muscular spiral arteries into large vascular channels transforms the uteroplacental circulation into a low-resistance-to-flow system

Review Waveform n Component 1: Pulsatile Waveform n Component II: Steady Waveform

Review Waveform n Pulsatile Component: Formed by the interaction of an outgoing and reflected wave, which bounces back to the heart upon reaching the uteroplacental vascular bed

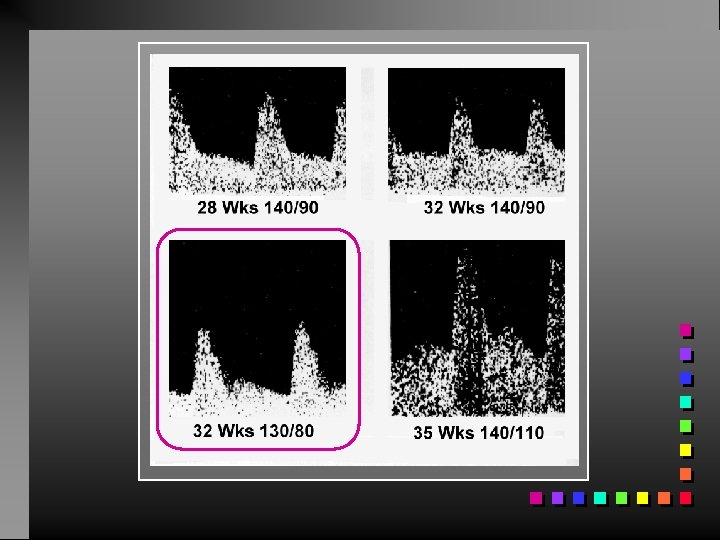
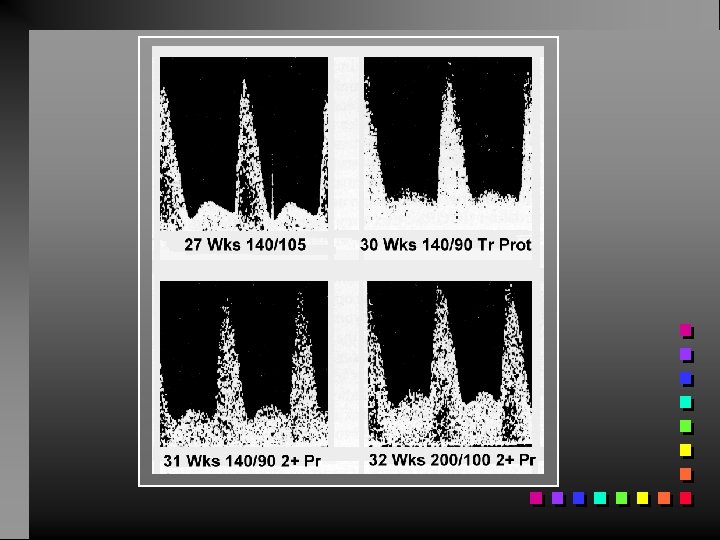
Review Waveform Analysis n Increased Resistance n n n Decrease Mean Velocity Elevated PI Development of a notch in the early diastolic portion of the velocity waveforem caused by destructive interaction between outgoing and reflected waves

Review Waveform Analysis n Decrease Uterine Artery Radius n n n Increase Mean Velocity Elevated PI and S/D NO DIASTOLIC NOTCH

Review Waveform Analysis n Increase Mean Arterial Pressure n n n Elevation in mean velocity NO change in RI or S/D NO DIASTOLIC NOTCH

Review Preeclampsia and Hypertension n n Abnormal decidual segments of the spiral arteries Minimal or no trophoblastic invasion beyond the decidual-myometrial junction

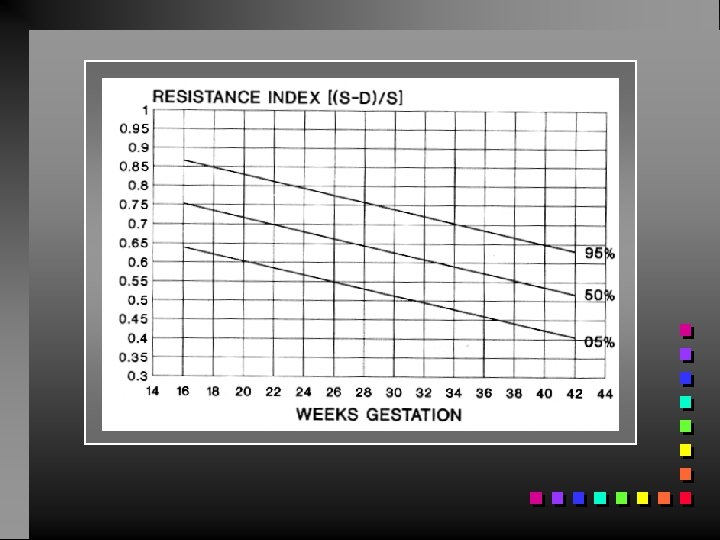
Review Waveform Measurements Resistance Index of > 0. 58 after 18 weeks of gestation RI = (S-D)/S Systole Diastole
")
Review Waveform Measurements Diastolic Notch (irrespective of the RI)

High-Risk Studies Prediction of Preeclampsia n n Arduini 1987 Jacobson 1990 Montenegro 1992 Bower 1993 Total Patients: 563 Prevalence: 11% Sensitivity: 81% Specificity: 82%

High-Risk Studies Prediction of IUGR n Jacobson 1990 Total Patients: 93 Prevalence: 18% Sensitivity: 71% Specificity: -

Low-Risk Studies Prediction of Preeclampsia n n n Steel 1990 Harrington 1992 Bower 1993 Valensise 1993 North 1994 Total Patients: 6657 Prevalence: 4. 4% Sensitivity: 56% Specificity: 72%

Low-Risk Studies Prediction of IUGR n n n Steel 1990 Newnham 1990 Uzan 1994 Bower 1993 Valensise 1993 North 1994 Total Patients: 4515 Prevalence: 7. 7% Sensitivity: 41% Specificity: 89%

Preeclampsia High-Risk Low-Risk IUGR Total Patients: 563 Prevalence: 11% Sensitivity: 81% Specificity: 82% Total Patients: 93 Prevalence: 18% Sensitivity: 71% Specificity: - Total Patients: 6657 Prevalence: 4. 4% Sensitivity: 56% Specificity: 72% Total Patients: 4515 Prevalence: 7. 7% Sensitivity: 41% Specificity: 89%

Treatment Aspirin Low-Dose Aspirin Can Be Used As A Form Of Therapy Rationale: Imbalance favoring the production of thromboxane A 2 over prostacyclin is thought to play an important role in the pathogenesis of preeclampsia and somes caes of IUGR.

Treatment Aspirin How Does It Work? Rationale: Low-dose aspirin irreversibly inhibits almost all platelet cyclooxygenase activity, thereby blocking the production of thromboane A 2, a potent vacoconstrictor and paltelet-aggregating agent.

Treatment Criteria For Treatment 1. Persistence of a Diastolic Notch after 24 to 26 weeks of gestation. 2. An RI greater than 0. 58 after 24 weeks.

Treatment Dosage of Aspirin 50 to 150 mg/day beginning at 24 weeks. Stuart Campbell has begun aspirin at 20 weeks when bilateral notching is present

High-Risk Studies Incidence of Preeclampsia: Aspirin vs Placebo n n Mac. Parland 1990 Montenegro 1990 Uzan 1994 Bower 1993 Total Patients Tx with Aspirin: 106 Total Patients Tx with Placebo: 108 Preeclampsia Aspirin Group: 7% Preeclampsia Control Group: 41% P < 0. 00001 Relative Risk: 6 times greater for the Placebo Group to develop preeclampsia

High-Risk Studies Incidence of IUGR: Aspirin vs Placebo n n Mac. Parland 1990 Montenegro 1990 Uzan 1994 Bower 1993 Total Patients Tx with Aspirin: 106 Total Patients Tx with Placebo: 108 IUGR Aspirin Group: 15% IUGR Control Group: 26% P < 0. 08

High-Risk Studies Elevated Maternal Serum Alpha-Fetoprotein Increased MSAFP is associated with an increased risk for perinatal death, preterm delivery, and IUGR. Patients with an increased MSAFP and an abnormal uterine artery Doppler velocimetry are at increased risk for adverse perinatal outcome

Studies Elevated Maternal Serum Alpha-Fetoprotein Number of Patients: 98 Criteria: Elevated MSAFP and abnormal uterine artery Doppler velocimetry after 24 weeks Findings: • 14% perinatal death rate • 25% delivered prematurily • 20% had IUGR • Persistent notch after 24 weeks predicted 79% of perinatal deaths (Aristidou A, Van Den Hof M, Campbell S, et al. Uterine artery Doppler in the investigation of pregnancies with raised maternal serum alpha-fetoprotein. Br J Obstet Gynaecol 1990; 97: 431)

Studies Preterm Labor Number of Patients: 92 Criteria: Preterm labor and abnormal uterine artery Doppler velocimetry Findings: • Preterm Delivery: PPV 78. 6%, NPV 69. 2% • Abnormal perinatal outcome: PPV 64. 3%, NPV 82. 1% (Brar HS, Medearis AL, De. Vore GR et al, Maternal and feal blood flow velocity waveforms in patient with preterm labor. Relationship to outcome. Am J Obstet Gynecol 1989; 161: 1519)

Conclusions Uterine Artery Doppler Velocimetry 4 This screening test identifies patients at increased risk for adverse perinatal outcome 4 This test should be done at 18 to 22 weeks during the anatomical survey 4 If abnormal at 24 weeks, lowdose aspirin should be initiated
- Slides: 72