Done by Thaer Omar Alqatish What is Hypertension

Done by: Thaer Omar Al-qatish

What is Hypertension ? ? • AHA/ACC 2017 definition: persistent systolic blood pressure of ≥ 130 mm Hg and/or diastolic blood pressure ≥ 80 mm Hg • JNC 8 definition: persistent systolic blood pressure of ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg • Definition of hypertension in children < 13 years: blood pressure ≥ 95 th percentile to < 95 th percentile + 12 mm Hg OR systolic blood pressure ≥ 130 mm Hg and/or diastolic blood pressure ≥ 80 mm Hg (whichever is lower) [1][2]

Epidemiology • Prevalence • One in three adults in the US is affected. • Prevalence increases with age (∼ 65% among those ≥ 60 years of age). * However, the prevalence of hypertension among school-aged children and adolescents is increasing (particularly in those who are obese). • African Americans are more commonly affected than Asian American or white individuals. • 60– 75% of obese and overweight patients are affected. • Sex: ♂ > ♀ below age of 45; the sex ratio is almost balanced at > 45 years of age (i. e. , after menopause) • Most common risk factor for cardiovascular disease
 (i. e. , there is no identifiable")
Types of HTN 1. Essential hypertension (HTN) (i. e. , there is no identifiable cause) *Accounts for 85– 95% of cases of hypertension in adults *Age at onset: 25– 55 years (prevalence is increasing in adolescents) 2. Secondary HTN has many identifiable causes. *Accounts for 5– 15% of cases of hypertension in adults *Age at onset < 25 years or > 55 years
: most common cause")
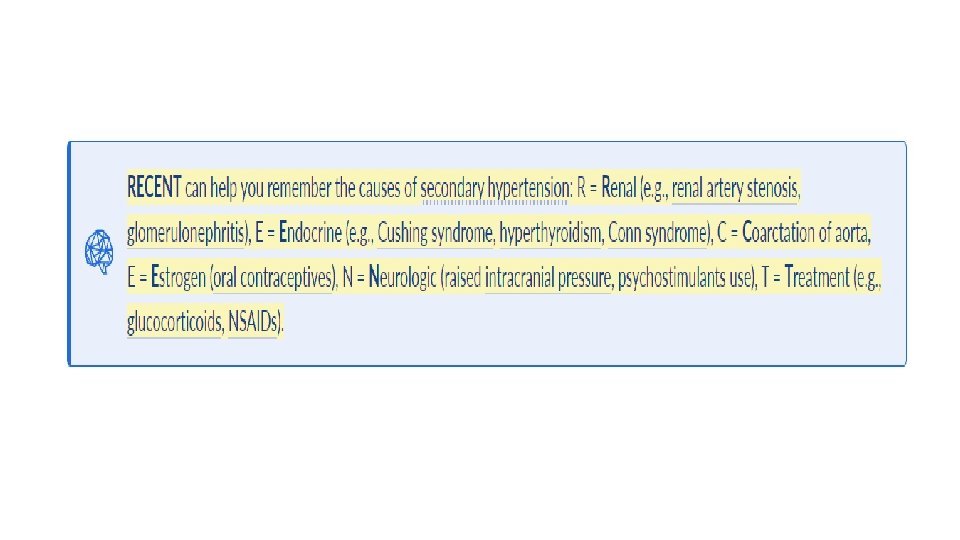
Secondary HTN Causes • Endocrine hypertension • Primary hyperaldosteronism (Conn syndrome): most common cause of secondary hypertension in adults • Hypercortisolism (Cushing syndrome) • Hyperthyroidism • Pheochromocytoma • Primary hyperparathyroidism • Acromegaly • Congenital adrenal hyperplasia • Renal hypertension • • • Renovascular hypertension (e. g. , due to renal artery stenosis) Polycystic kidney disease (ADPKD) Renal failure (renal parenchymal hypertension) Glomerulonephritis Systemic lupus erythematosus Renal tumors Coarctation of the aorta Obstructive sleep apnea Medication: sympathomimetic drugs, corticosteroids, NSAIDs, oral contraceptives Recreational drug use: amphetamines, cocaine, phencyclidine

Risk factors For HTN • Nonmodifiable risk factors • Positive family history • Ethnicity • Advanced age • Modifiable risk factors • • • Obesity Diabetes Smoking, excessive alcohol or caffeine intake Diet high in sodium, low in potassium Physical inactivity Psychological stress

Clinical Findings • Hypertension is usually asymptomatic until: • Complications of end-organ damage arise • Or an acute increase in blood pressure occurs (Hypertensive crises ; urgency & emergency ) • Secondary hypertension usually manifests with symptoms of the underlying disease (e. g. , abdominal bruit in renovascular disease, edema in CKD, daytime sleepiness in obstructive sleep apnea). • Nonspecific symptoms of hypertension • • Headaches, esp. early morning or waking headache Dizziness, tinnitus, blurred vision Flushed appearance Epistaxis Chest discomfort, palpitations; strong, bounding pulse on palpation Nervousness Fatigue, sleep disturbances

Classification of HTN

When to establish the diagnosis ? ? • Establish the diagnosis on the basis of at least two readings over 4 or more weeks apart. • Diagnose HTN on the basis of one BP reading, if the patient has severe HTN or evidence of end-organ damage. (Hypertensive crises)

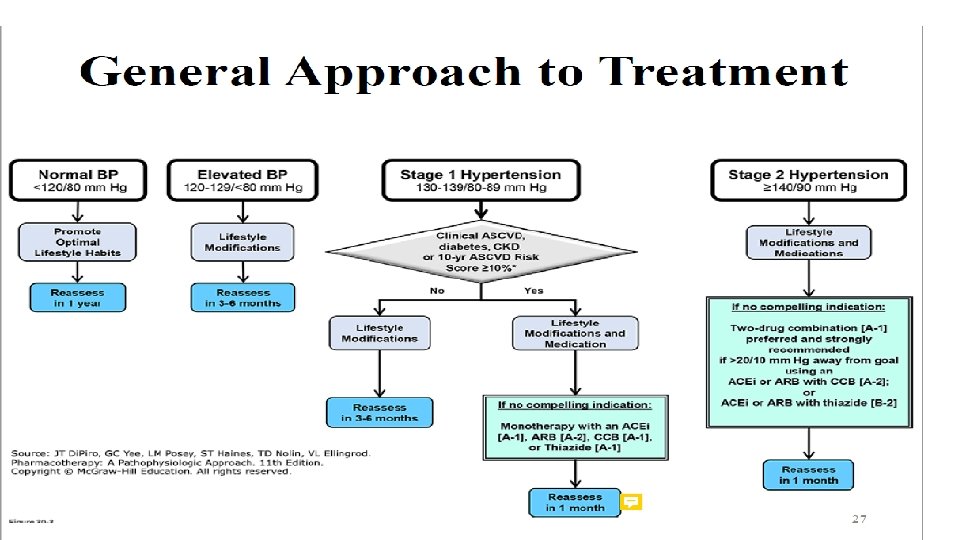
• Overall Goal of Treatment : • Reduce morbidity and mortality from CV events (eg, coronary events, cerebrovascular events, HF) and kidney disease. • Prevent damage to target organs (heart, kidneys, eyes, CNS). • Most patients (including patients with clinical ASCVD [secondary prevention], diabetes, or CKD; primary prevention patients regardless of 10 -year ASCVD risk score): <130/80 mm Hg • Institutionalized older patients, those with high disease burden and comorbidities, or limited life-expectancy: Consider a relaxed SBP goal of at least <150 mm Hg; <140 mm Hg in some patients if tolerated.

Initial evaluation of newly diagnosed hypertensive patients • Stratification of cardiovascular risk: fasting blood glucose, lipid profile (HDL, LDL, and triglycerides levels) + calculate ASCVD risk. • Evaluation of end-organ damage and underlying causes • • • Complete blood count Renal function tests: serum creatinine and e. GFR Serum Na+, K+, and Ca 2+ Urinalysis TSH Electrocardiogram (ECG)

http: //www. cvriskcalculator. com/

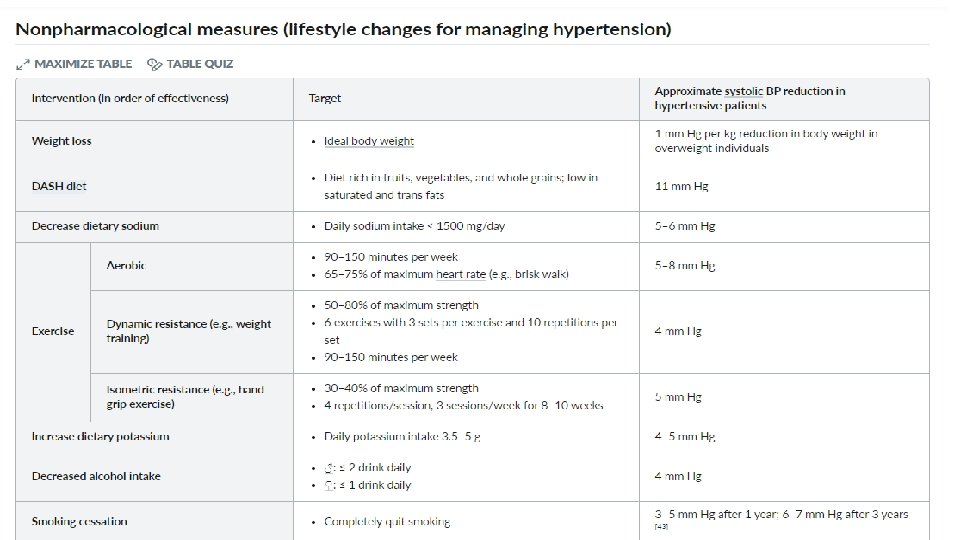
Treatment 1 - Nonpharmacological measures 2 - Pharmacologic treatment

First line drugs

Second line drugs

• If the patient’s response to one agent is not adequate, there are two options: • Increase the dose of the first agent to the maximum dose. • Add a second medication (thiazide, calcium channel blocker, ACE inhibitor, or ARB); if target BP not achieved, increase the dose of each as necessary until the maximum dose is achieved. • If a patient’s response is still inadequate with two agents, consider a third agent, look for secondary causes, and referral to an HTN specialist.

• The four classes of drugs that are used for initial monotherapy are thiazide diuretics, long-acting calcium channel blockers (most often a dihydropyridine), and ACE inhibitors/ or ARBs. • β-Blockers are not commonly used as initial monotherapy in the absence of a specific indication because of adverse effects on some cardiovascular outcomes especially in elderly patients. • Most patients eventually need more than one drug to attain goal BP (especially diabetics, obese patients, and those with renal failure). • Always obtain a pregnancy test in reproductive age women before starting an antihypertensive medication. [Thiazides, ACE inhibitors, and ARBs are contraindicated in pregnancy. β-Blockers and hydralazine are safe. ]

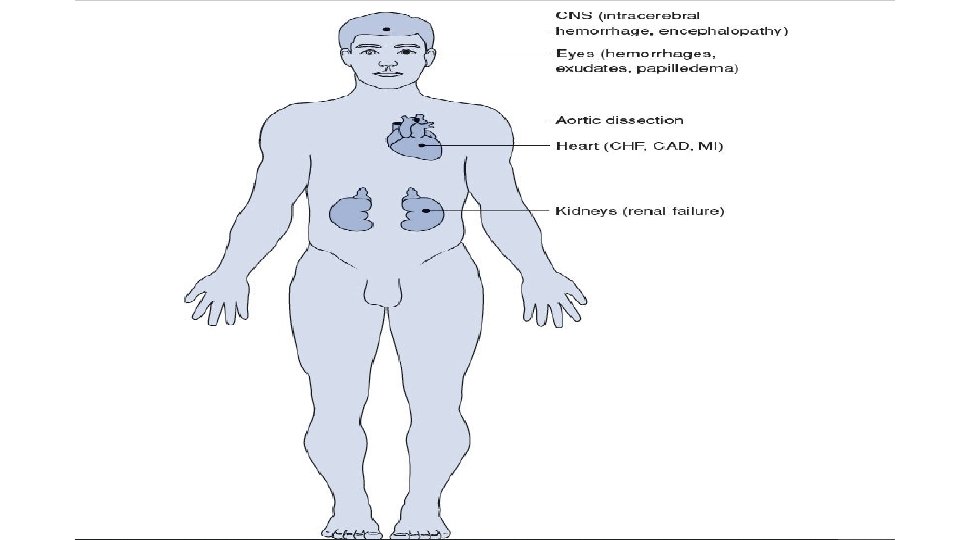
Complications of uncontrolled hypertension • The major complications of HTN are cardiac complications (coronary artery disease [CAD], CHF with left ventricular hypertrophy [LVH]), stroke, and renal failure. These account for the majority of deaths associated with untreated HTN.

Cardiovascular system • Effects on the heart are most important. HTN is a major risk factor for CAD, with resultant angina and MI. • CHF is a common end-result of untreated HTN as LVH occurs. • Most deaths due to HTN are ultimately due to MI or CHF. • HTN predisposes the patient to peripheral artery disease (PAD). • HTN is associated with increased incidence of abdominal aortic aneurysm • (AAA) and aortic dissection.
 • Early changes—arteriovenous nicking (discontinuity in the retinal vein secondary to")
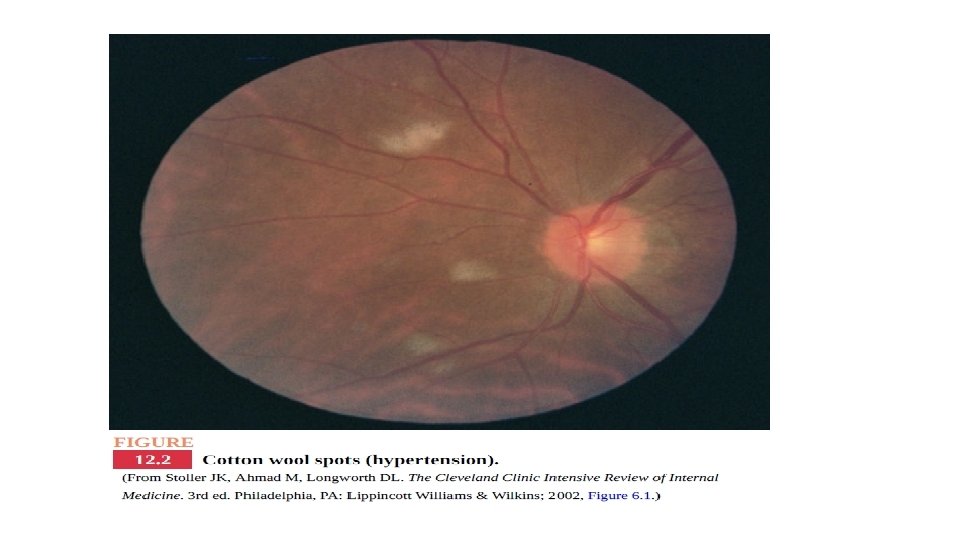
Eyes (retinal changes) • Early changes—arteriovenous nicking (discontinuity in the retinal vein secondary to thickened arterial walls) and cotton wool spots (infarction of the nerve fiber layer in the retina) can cause visual disturbances and scotomata • More serious disease—hemorrhages and exudates. • Papilledema—an ominous finding seen with severely elevated BP.

CNS • Increased incidence of intracerebral hemorrhage. • Increased incidence of other stroke subtypes as well (transient ischemic attacks • [TIAs], ischemic stroke, and lacunar stroke). • Hypertensive encephalopathy when BP is severely elevated (uncommon).

Kidney • Arteriosclerosis of afferent and efferent arterioles and glomerulus— called nephrosclerosis. • Decreased GFR and dysfunction of tubules—with eventual renal failure.
 • Since hypertension is often asymptomatic, regular screening is")
Screening For HTN (USPSTF recommendations) • Since hypertension is often asymptomatic, regular screening is necessary to prevent end-organ damage. • Individuals 18– 39 years of age with normal blood pressure (< 130/85 mm Hg) and without other risk factors: Screen every 3– 5 years. • Individuals > 40 years of age or who are at increased risk for high blood pressure : Screen every year.
 • Definition: arterial")
Subtypes and variants 1 - White coat hypertension (white coat effect) • Definition: arterial hypertension detected only in clinical settings or during blood pressure measurement at a physician's practice • Etiology: anxiety experienced by the patient • Diagnostics: 24 -hour blood pressure monitoring 2 - Isolated systolic hypertension (ISH) • Definition: increase in systolic blood pressure (≥ 140 mm Hg) with diastolic BP within normal limits (≤ 90 mm Hg) • Etiology : -decreased arterial elasticity and increased stiffness → decreased arterial compliance -Or secondary to increased cardiac output Anemia, Hyperthyroidism, …. • Treatment: thiazide diuretics or dihydropyridine calcium antagonists.
")
Hypertensive crises • Hypertensive urgency—severe HTN (typically systolic BP >180 and/or diastolic BP >120) in an asymptomatic patient ( no end organ damage) • Hypertensive emergency—severe HTN with end-organ damage (e. g. , neurologic changes, myocardial ischemia, aortic dissection) • Malignant hypertension: severe hypertension that occurs with retinopathy (flame hemorrhages, papilledema) [This term is no longer used by the AHA. ]

Approach to management 1 - Confirm blood pressure manually and on bilateral upper extremities. (Make sure the cuff is the appropriate size. ) 2 - Determine if there are signs of end-organ damage. • Focused history/physical • Select screening tests 3 - For hypertensive emergencies • ABCDE approach • Admit patients (ideally to ICU). • Lower the blood pressure acutely using IV agents and aim for targets based on the affected end-organs • Evaluate and treat underlying disorders. 4 - For hypertensive urgency • Select, reinstitute, or modify oral antihypertensive therapy. • In patients with a new diagnosis, evaluate for secondary causes of hypertension. • Arrange follow-up, monitoring, and counseling.
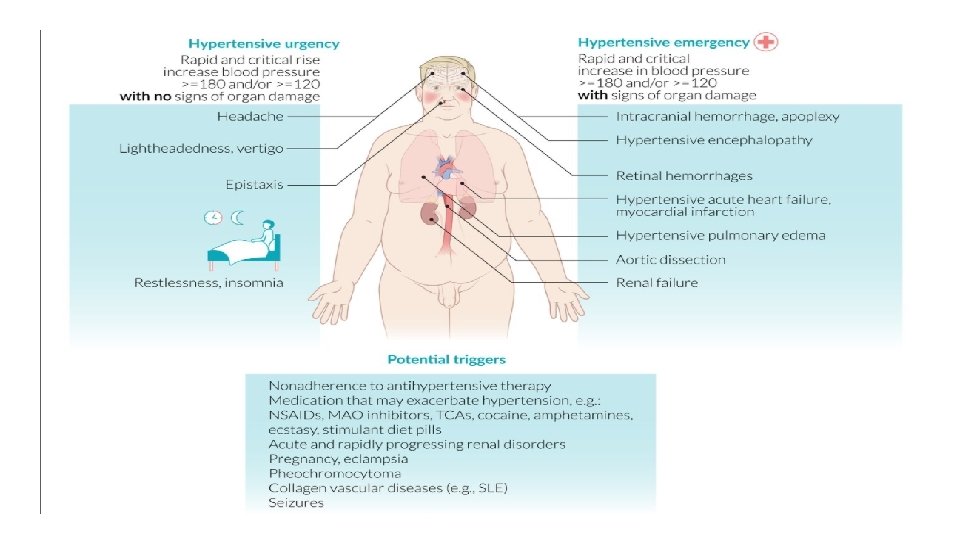

Signs and symptoms of end-organ dysfunction • Cardiac • Heart failure exacerbation, pulmonary edema: dyspnea, crackles on examination • Myocardial infarction: chest pain, diaphoresis • Aortic dissection: chest pain, asymmetric pulses • Neurologic • Hypertensive encephalopathy: headache, vomiting, confusion, seizure, blurry vision, papilledema • Ischemic or hemorrhagic stroke: focal neurological deficits, altered mental status • Renal • Acute renal failure: azotemia and/or oliguria, edema • Ophthalmic • Acute hypertensive retinopathy: blurry vision, decrease in visual acuity, retinal flame hemorrhages, papilledema • Other • Microangiopathic hemolytic anemia: fatigue, pallor

Diagnostics • Evaluate for signs of end-organ damage • Laboratory studies • CBC: signs of microangiopathic hemolytic anemia • BMP: altered electrolytes and/or elevated creatinine and urea, which suggest kidney failure • BNP: elevated in heart failure • Troponin: elevated in myocardial ischemia • Urinalysis: signs of glomerular injury (e. g. , proteinuria, hematuria) • ECG: left ventricular hypertrophy, signs of cardiac ischemia (e. g. , ST depressions or elevations) • Chest x-ray: cardiomegaly, pulmonary edema

Additional evaluation to consider • Urine pregnancy test • Toxicology screen • CT chest with IV contrast if chest pain is concerning for aortic dissection • Consider TTE if clinical features suggest pulmonary edema. Consider CT head if neurological symptoms are present.

Treatment For Hypertensive urgency • Outpatient treatment is recommended. • Move patient to a quiet room for 30 minutes. • Reinstitute or increase the dosage of existing oral antihypertensive therapy. • Reassess the patient within 4 -7 days at most.

Treatment For Hypertensive Emergency • ICU admission and immediate initiation of intravenous antihypertensive therapy • Rate and target of blood pressure reduction: • General goal • Reduce BP by max. 25% within the first hour to prevent coronary insufficiency and to ensure adequate cerebral perfusion pressure. • Reduce BP to ∼ 160/100– 110 mm Hg over the next 2– 6 hours. • Reduce BP to patients baseline over 24– 48 hours.

Special cases • Indications for the rapid lowering of systolic BP (usually to < 140 mm Hg) in the first hour of treatment include severe pre- eclampsia or eclampsia, aortic dissection, and pheochromocytoma with hypertensive crisis.

Choice of intravenous antihypertensive drug • Calcium channel blocker: • Nicardipine • Clevidipine • Nitric-oxide dependent vasodilators: • Sodium nitroprusside • Nitroglycerin • Direct arterial vasodilators: hydralazine • Antiadrenergic drugs • Selective beta-1 antagonist: esmolol • Nonselective beta blocker with alpha-1 antagonism: labetalol • Nonselective alpha antagonist: phentolamine • D 1 agonist: fenoldopam • ACE inhibitor: enalaprilat

- Slides: 41