Doing Research in Behavior Analysis 4 Phases of

Doing Research in Behavior Analysis

4 Phases of a program 1. 2. 3. 4. • Screening Baseline Treatment Follow-up How do we know if the treatment actually caused the change in behavior?

ANALYZING DATA

FREQUENCY GRAPH
")
BAR GRAPH (FREQUENCY)

CUMMULATIVE GRAPH

CUMMULATIVE GRAPH

INTERVENTION DESIGNS • TO RULE OUT ALTERNATIVE EXPLANATIONS ________ FOR CHANGE • BASELINE ( MEASURE BEFORE INTERVENTION 1. VERIFY BEHAVIOR _____ STATE MEASURE 2. VERIFY YOUR _______ INTERVENTION 3. COMPARRISON FOR _______ 4. BEHAVIOR MAY CHANGE

Training/Treatment-Designs • TO RULE OUT ALTERNATIVE EXPLANATIONS • Reversal design • Multiple Baseline – Across behavior, settings, or people • Alternating treatments(multi-element) • Changing criterion
 • Dependent variable behavior to change – The measure of the ______ •")
Reversal-replication(ABAB) • Dependent variable behavior to change – The measure of the ______ • Independent variable – The treatment • • “A” is the baseline; “B” is the treatment Conditions are “reversed” to baseline replicated Treatment is “________ ” Also called the “withdrawal” design

ABAB REVERSAL DESIGN

Some questions • Assuming response definition, observer accuracy, & data recording are OK… 1. How long a baseline? 1. Stability, 2. Trends 3. How representative of the actual behavior

VISUAL ANALYSIS • Immediacy of effects OVERLAP • ______ OF VALUES FROM BASELINE TO INTERVENTION STABILITY • ______ OF DATA IN BASELINE • TREND IN BASELINE IN THE DIRECTION EXPECTED _______ OF INTERVENTION

EFFECTIVE TRAINING

LESS EFFECTIVE

WEAK EFFECT

INCREASED VARIATION

CLEAR EFFECT

TREND IN BASELINE

CLEAR EFFECT

CLEAR EFFECT

NUMBER EFFECTIVE TREATMENT

NUMBER NOT EFFECTIVE

NUMBER TREND IN BASELINE

Why?

WHY? DRO PRAISE

WHAT HAPPENED?

WHY?

Other considerations • Scientific—is this phenomenon new? longer – Yes—perhaps a ______ baseline • Practical -how much time do we have? What resources are available? dangerous • Ethical – How _______ is the behavior?

Other questions • How many reversals & replications? – If the phenomenon is well researched & the treatment effect is large perhaps one is OK. – If the effect is small and / or the phenomenon is new perhaps several

Other questions ethical ? • Is reversing effective treatment _______ • What if the behavior change is irreversible _________ ? – Behavior traps ( e. g. , social interaction, physical restrictions[ golf driving]))

MULTIPLE BASELINE two behaviors concurrently • Baseline _____ • Baseline one behavior in two situations _____ concurrently people • Baseline a treatment across ____ • Baseline different behaviors across situations different ______ • Assumes behaviors are independent

MULTIPLE BASELINE

Potential problems • If behavior changes on both situations ( due to stimulus generalization across situations for example) no conclusion can be drawn regarding the independent variable • The behavior may not occur in more than one situation • One treated person may influence the next to be treated person • Not enough observers
 • How to compare two different treatments for the same behavior?")
ALTERNATING Rx (multi-element) • How to compare two different treatments for the same behavior? • A multiple baseline is not well suited to do this • So…we rapidly alter RX back and forth and watch for effects under each condition

ALTERNATING Rx

Multi-element used in Functional Analyses

Potential Problems interact • Two conditions may _____ (extinction burst in play condition after attention condition) or due to stimulus generalization across conditions

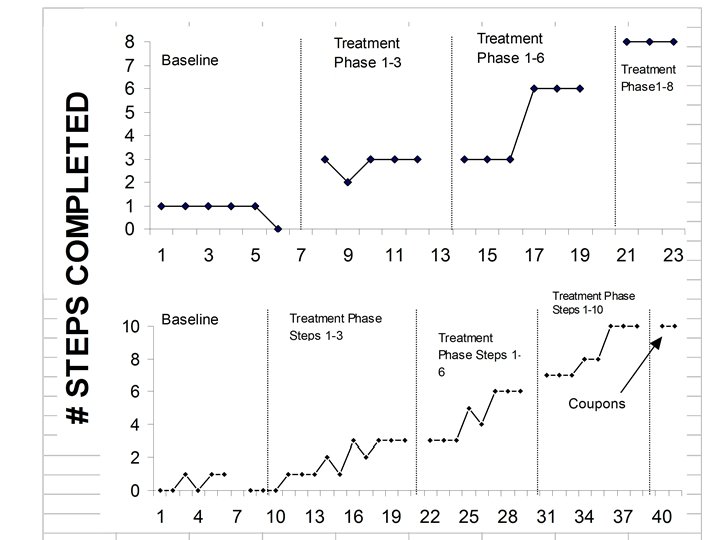
Changing Criterion values of the independent • Specific _______ variable are introduced in order • E. G. number of steps that are required for reinforcement • Different values of the reinforcement schedule

Issues Scientific effectiveness 1. 2. 3. 4. 5. 6. 7. > # of replications = > effect < overlapping points > effect The sooner the effect The larger the effect The more precisely defined procedures The more reliable the measures The more consistent with the literature

Issues • Clinical effectiveness • Social Validity – How important was the problem to the person? – How acceptable were the procedures – How satisfied is the person with the outcome
 • If we don’t do research on clinical effectiveness and only provide")
Issues (Larry’s) • If we don’t do research on clinical effectiveness and only provide “clinical service” where does better treatment come from? • Just because we provide only “clinical” service and don’t do research can we afford not to take reliability measures?
- Slides: 43