Diving Medicine LCdr Peter Hatfield Objectives Barotrauma Decompression

Diving Medicine LCdr Peter Hatfield

Objectives Barotrauma Decompression Illness Gas Problems Putting it together

1. pre-existing medical condition 2. trauma/drowning/hypothermia 3. Barotrauma 4. Decompression Illness 5. Gas Problems eg myocardial infarction

Barotrauma Boyles Law Volume inversely proportional to pressure
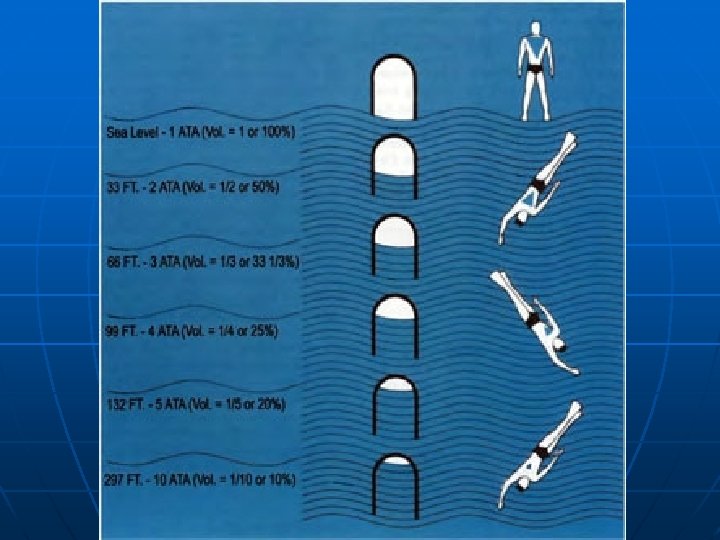

Gas attempts to contract or expand IAW Boyle’s Law In closed spaces, gas cannot enter or escape Therefore, a pressure differential will develop Squeese or reverse squeese

1. Non pulmonary barotrauma suit/mask squeeze sinuses ears teeth bowel 2. Pulmonary barotrauma arterial gas embolism mediastinal emphysema pneumothorax subcutaneous emphysema

Suit/mask squeeze

Ears/Sinuses

Ears Barotrauma Teeds 0 -5 Alternobaric vertigo Draeger Ear Perilymphatic fistula Facial Baroparesis
 24 to 72")
Barotrauma Treatment Middle Ear Restrict diving until resolved; Mild (0 -1) 24 to 72 hours Moderate (2 -3) 1 to 8 days Severe (4 -5) may take up to six weeks decongestant , +/- antibiotic Perilymphatic fistula ENT referral – may need surgery Facial Baroparesis need to reverse due to ischemia -myringotomy

Dental- fractured tooth/abcess Bowel- possible surgical consult On ascent or descent
 water depth")
Pulmonary Barotrauma Potential alveolar rupture from 1 msw (3 fsw) water depth

Pulmonary Barotrauma 1. 2. 3. 4. Arterial Gas Embolism Pneumothorax Mediastinal Emphysema Subcutaneous Emphysema

Breath-hold on ascent Panic, buddy breathing, laryngospasm Local air trapping in lungs Obstructive lung disease, scarring/fibrosis Frequent Change in Pressure
 Likely on ascent Conscious/LOC Any neurological symptom/sign")
Symptoms Rapid onset (less than 5 min) Likely on ascent Conscious/LOC Any neurological symptom/sign Hemoptysis Shortness of breath High pitched cry Pleuritic type Chest pain Subcutaneous emphysema (internal carotid most likely) Can co-exist with pneumothorax or mediastinal/subcutaneous emphysema

Treatment ABC s Lie down, on side if unconscious Head down only for short time if at all Catheterization if unconscious 100% oxygen Transport to nearest RCC Maintain 1 ATA ambient pressure if possible
 5")
Treatment Table 6 4 Hours 46 Minutes 0 30 09 m (30 ft) 5 20 5 20 30 18 m (60 ft) ASCENT RATE: 0. 3 m/min (1 ft/min) 20 5 DESCENT RATE: 18 m/min (60 ft/min) O 2 periods 3 at 18 msw (60 fsw) 6 at 09 msw (30 fsw)

Time to Tx of A. G. E. and Response

Decompression Illness Compressed air 79% nitrogen 20% oxygen

Venous bubbles unlike AGE Left/right shunt could become arterial eg patent foramen ovale 1929 Clark infused 2, 000 ml air at 50 ml/hour into a dog with no signs of DCI Asymptomatic Military divers can be shown to have bubbles (on doppler) after experimental dives

Deeper/longer dives Inadequate decompression Age Fatigue before diving Cold during decompression Heavy exercise before during or after diving Dehydration (alcohol consumption) Infection, medication Flying after diving Rapid decompression at altitude

Bubbles cause Blood / bubble interface activates blood components Body treats the bubble as a foreign object and coats it in protein RBC agglutination, platelet consumption, vascular permeability, leukocyte activation, etc. Endothelial injury. Bubbles activate complement system in some individuals.

Decompression sickness/stress Continuum Decompression Mild DCS Severe DCS stress without stress with Type II symptoms No dive No stress Deat h
 Skin itch and erythema Joint pain Lymphatic")
Mild Symptoms Fatigue Fleeting joint discomfort (niggles) Skin itch and erythema Joint pain Lymphatic Skin (cutis marmorata) Severe Symptoms CNS/ Spinal Labyrinthine (staggers) Pulmonary (chokes)

Time to symptoms During decompression 0 -30 min 30 -60 min 1 -6 hours 6 -12 hours 12 -24 hours Rare 50% 75% 90% 95% 99%
 IV Ringers/normal saline")
Treatment 100 % oxygen delivers oxygen to tissues nitrogen gradient (elimination) IV Ringers/normal saline RCC even if symptoms have resolved

Gas Problems SYMPTOMS AT DEPTH Nitrogen Oxygen Carbon Dioxide Impurities Partial pressure at 1 ATA At 30 m 4 ATA At 60 m 7 ATA O 2 =. 21 =. 84 =1. 47 CO 0. 01 % 0. 04 0. 07

Oxygen Toxicity Pulmonary CNS occurs at partial pressure 1. 6 ATA O 2 70 m on air 6 m on 100% O 2 CON – Convulsion V – Visual aberrations E – Ears, ringing, bells, etc. N – Nausea T – Twitching of facial muscles I – Irritability, behavior changes D – Dizziness

Nitrogen narcosis Martini’s law - 1 martini per every 10 m after 20 m depth Carbon dioxide 1 -10 % symptoms Headache, nausea, fatigue, sweating, tachycardia SOB, confusion

Putting it Together History Where most important dive buddy did the symptoms start and descent bottom surface Type of dive Prexisiting conditions When 1) immediately 2) delayed

Physical exam- ABC s neuro exam Signs- resolving, static, progressing AGE or DCS treatment is the same “ 4 min neuro”

Case 1 Vertigo examples 21 year old diver with cold symptoms, pain in ear on descent. Forced valsalva- sudden ( in water) onset of vertigo, tinnitus, hearing loss Barotrauma to ear alternobaric vertigo perilymphatic fistula Did he get better on the surface Compare Diver on air 30 m for 25 minutes -no decompression stops. Develops vertigo tinnitus hearing loss 30 mins after surface Diver on air 10 m for 120 minutes

Case 2 Diver on air 15 m after 10 mins at depth feels dizzy, headache, nausea Surfaces feels fine after 5 mins O 2 CO 2, CO, anxiety, non diving medical condition

Case 3 24 yr old diver feels unwell at 30 m after 20 mins. On surface anxious tingling in the face and arms feels fatigued, rapid breathing Physical normal Unsure – trial of pressure?

Trial of Pressure/Treatment Table 5 2 Hours 16 Minutes 0 30 09 m (30 ft) 5 30 20 ASCENT RATE: 0. 3 m/min (1 ft/min) 18 m (60 ft) 20 DESCENT RATE: 18 m/min (60 ft/min) 5 20 5 O 2 periods 2 at 18 msw (60 fsw) 1 at 09 msw (30 fsw)

Case 4 Diver on vacation several consecutive days diving. Flying home develops pain in shoulder. Can calculate “repat” group or wait 24 hours. Do not dive on a travel day

Case 5 Diver 40 m for 30 mins returns to surface within 5 mins develops weakness in left arm, CN VI palsy and ataxia ? AGE or DCI
- Slides: 41