Diverticular Disease Firas Obeidat MD Introduction Acquired herniations

Diverticular Disease Firas Obeidat, MD

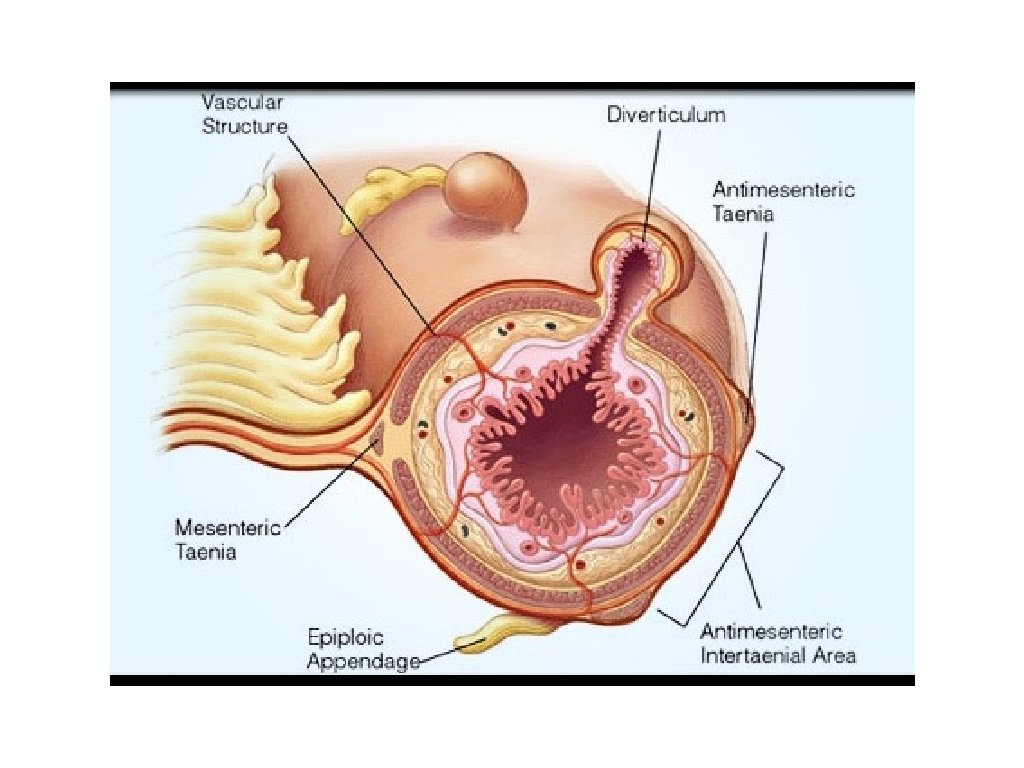
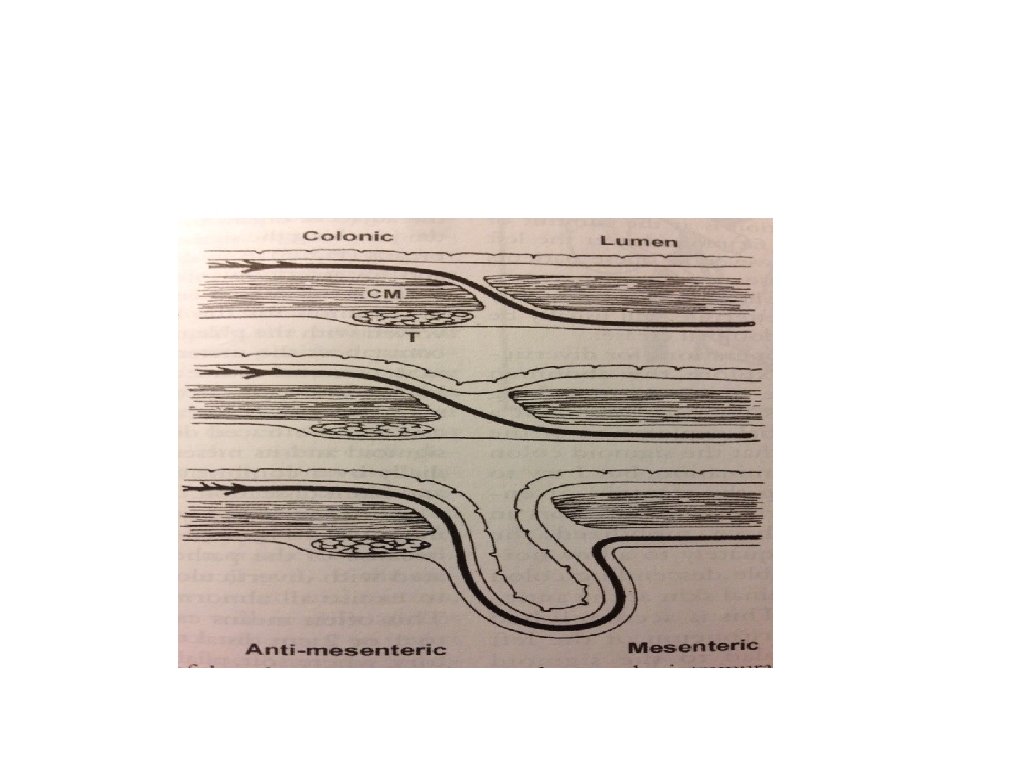
Introduction • Acquired herniations of mucosa through the muscle wall between the mesenteric and antimesenteric taenia. • Most common structural abnormality of the bowel. • In developed countries the prevalence of diverticular disease has increased during the last century: - detection - diet - aging

Incidence • < 40 yr = 5% • > 85 yr = 85% • Sigmoid colon is involved in over 95% of patients affected with diverticulosis • In western countries left-sided diverticulitis predominates with right-sided diverticulitis occuring in only 1. 5% • 10 -25% of pts will develop diverticulitis
")
Etiology • low fiber diet ( high fiber diet protect against diverticulitis not diverticulosis) • structural changes due to aging • decreased physical activity, obesity. • smoking. • constipation from any cause

Morphologic features • Macroscopic appearance: • thickening and shortening of the bowel • decrease in caliber and increase in intra luminal pressure • mesocolon is also foreshortened, possibly as a result of chronic inflammation.

Presentation • High incidence of diverticulosis, but clinical manifestations are relatively infrequent. • • symptomatic but uncomplicated diverticular disease ( chronic symptoms with no history of diverticulitis. complicated diverticulosis
 - accounts for")
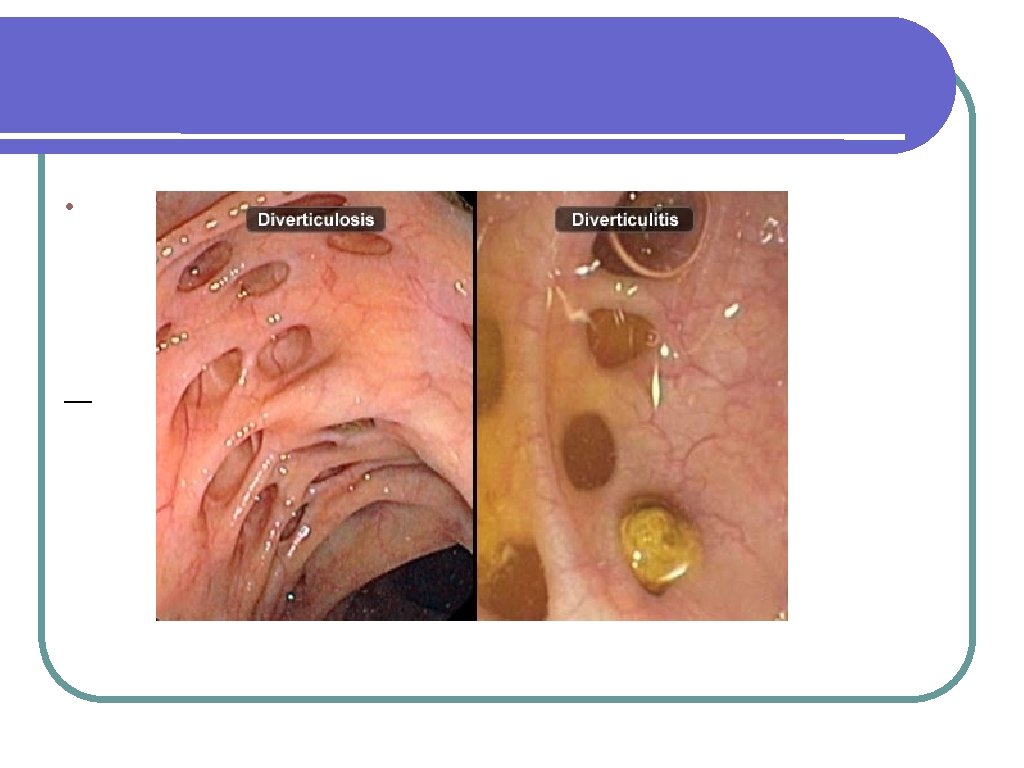
Cont. • diverticulitis: • uncompicated diverticulitis: - local inflammation ( microperforation) - accounts for 75% of cases - classical triad ( localized tenderness, fever and leukocytosis • complicated diverticulitis: - obstruction. - abscess or fistula formation. - free perforation.
 • Types:")
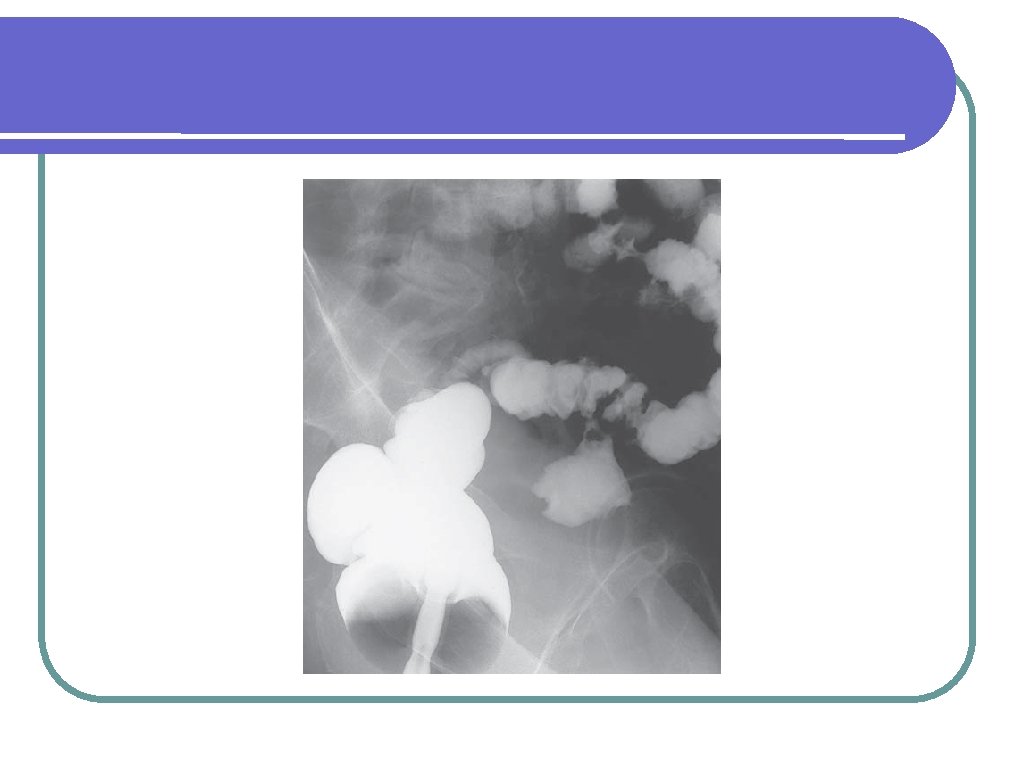
Complications • Fistula ( 5% of • Spontaneous • iatrogenic complicated diverticulitis) • Types: • colocutaneous: - spontaneous. - post abscess drainage. - postoperative • colovesical: - most common. - more in males. - recurrent urinary sepsis, urgency, pneumaturia. - cystoscopy, CT, barium enema

Cont. • coloenteric: - abscess discharge through the small bowel. - diarrhea. - may be asymptomatic. • colovaginal: - passage of flatus and feces through the vagina. - recurrent vaginal infection. - more common after hysterectomy.

Cont. • Bleeding: • pathogenesis. with angiodysplasia are the most common cause of massive lower GI bleeding ( usually associated with diverticulosis rather than diverticulitis. colonoscopy is mandatory to exclude malignany. diagnosis stops spontaneously in most cases rebleeding rate is high treatment: colectomy, embolization • •

Cont. • Obstruction: • luminal stenosis or extrensic compression from an abscess. • small bowel obstrucion or colonic obstruction • treatment: Hartman‘s, tubular resection, stent. • DD with malignancy!!!!

Cont. • Abscess: • most common complication of acute diverticulitis. • Symptoms. • signs: palpable mass. • treatment: small pericolic with antibiotics and bowel rest, CT or U/S guided drainage for larger or un resolving abscesses.

Classification of diverticulitis • Hinchey classification: Stage I: diverticulitis with associated pericolic abscess. • Stage II: diverticulitis associated with distant abscess (pelvic) • Stage III: diverticulitis associated with purulent peritonitis. • Stage IV: diverticulitis associated with fecal peritonitis. • • • Stages I and II: antibiotics and drainage. Stages III and IV: occurs in 1 -2% of cases Mortality 20 -30% treatment: surgery
 • Contrast study ( not indicated in")
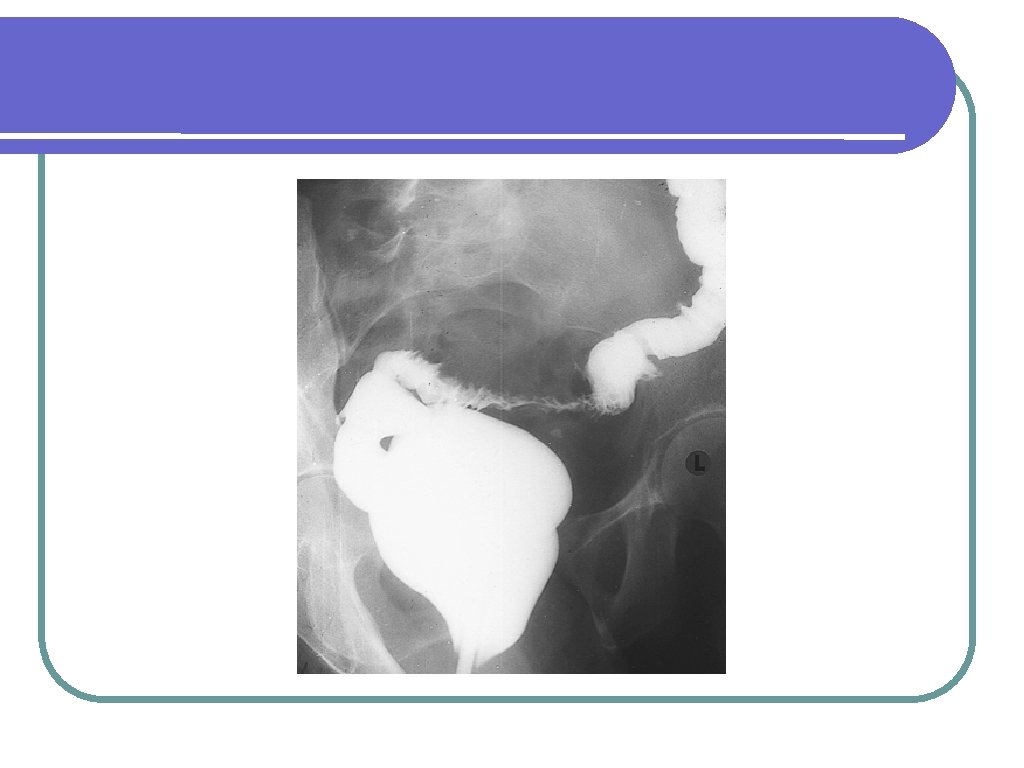
Investigations • CT scan (diagnostic and therapeutic) • Contrast study ( not indicated in acute diverticulitis ) • Colonoscoy (after resolution of acute attack)

Management • The • majority can be managed conservatively 15 -25% will require surgery during the initial complicated attack. • For those who experienced 2 nd attack, 60% of them will have complications. • After recovery from the 3 nd attack, only 10% • Recovery remain asymptomatic after the first attack can be expected in over 70% of patients versus 6% after the third episode.

Cont. • Indications for surgery: * colonic obstruction * fistula * in some cases of bleeding * recurrent diverticulitis. one attack in certain subgroups:

Cont. 1. young, fit patients: ? ? ? ? ? • • • 5% incidence more in male more malignant course. the majority have severe recurrence. more aggressive policy in surgical treatment 2. immunocompromised patients

Cont. -The American Society of Colon and Rectal Surgeons has appropriately recommended consideration of elective sigmoid colectomy after recovery from acute diverticulitis on a case-by-case basis, with the decision based on the: - Age - comorbid disease - the frequency and severity of the attacks - whether symptoms persist after the acute episode

Cont. • Emergent Acute Diverticulitis with Localized Peritonitis: - microperforation - most responded to conservative treatment - patients should have colonoscopy few wks after improvement • Emergent Acute Diverticulitis with Generalized Peritonitis: - macroperforation - Hartmann‘s procedure - primary anastomosis ? ? • Role of MIS:


Thank you
- Slides: 26