Diverticular Disease Done by Hala A Nsour Nomenclature

Diverticular Disease Done by ; Hala A Nsour

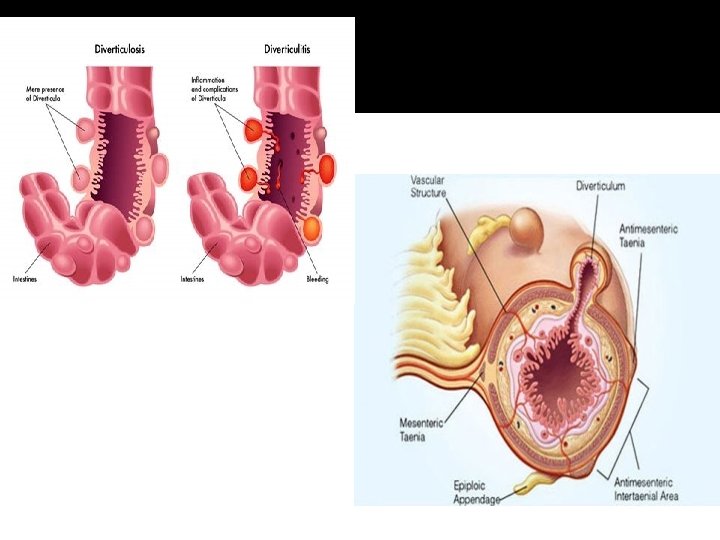
Nomenclature � Diverticulum = sac-like protrusion of the � Diverticulosis = describes the presence of gut wall diverticuli � Diverticulitis = inflammation of diverticuli
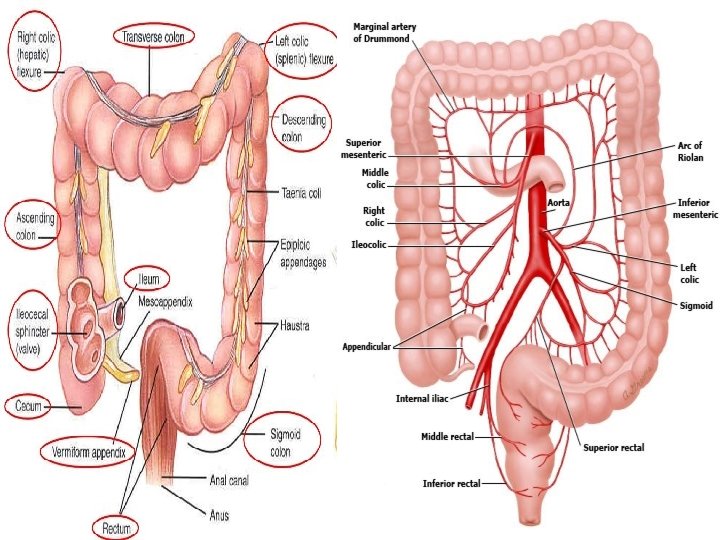

Diverticular Disease � Colonic diverticula are mucosal and sub mucosal out pouching through the muscular layer of the colon. (actually …. . Pseudo-diverticulum ! ) � The most common site for diverticula is the sigmoid colon, in 1 0% of patients they involve the entire colon. but they may develop anywhere � Diverticular disease has two clinical forms, DIVERTICULOSIS and DIVERTICULITIS

Epidemiology Diverticular disease of the colon is an acquired condition. � This condition is a disorder of modern civilization and is associated with consumption of refined food products. � anatomic location of diverticuli varies with the geographic location“Westernized” nations (North America, Europe, Australia) have predominantly left sided diverticulosis 95% diverticuli are in sigmoid colon � It is rare in rural African and Asian populations where dietary fiber is high. And usually right sided �

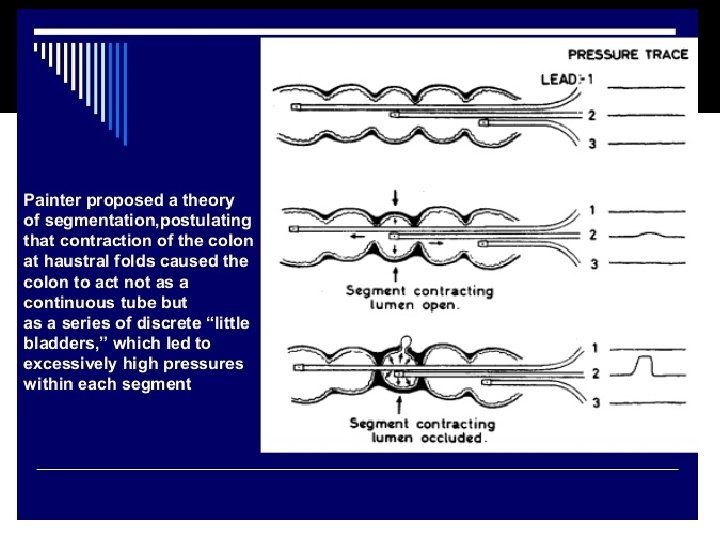
Pathophysiology � Diverticuli develop in ‘weak’ regions of the colon. � Segmentation = motility process in which the segmental muscular contractions separate the lumen into chambers Segmentation >> increased intraluminal pressure >>mucosal herniation >> Diverticulosis May explain why high fiber prevents diverticuli by creating a larger diameter colon and less vigorous segmentation

Risk factors and Lifestyle factors associated with diverticular disease; �Low fiber diet �Obesity �Lack of physical activity �Chronic constipation �Smoking �Family history

Clinical features

DIVERTICULOSIS �Most common cause of lower GI bleeding Clinical features : � Most patients are asymptomatic( asymptomatic 80%) � Occasionally, diverticulosis is associated with lower (mostly left ) abdominal colicky or constant pain � Diverticular bleeding: bleeding Most only have symptoms of bloating and diarrhea but no significant abdominal pain �Painless hematochezia , Start – stop pattern; “water faucet” , Bright red blood no previous melena

Diagnosis �radiograph film with barium enema; Air-Contrast Barium Enema Saw tooth appearance

Diagnosis � high-resolution CT scan enhanced with per os and IV contrast �Colonoscopy

Diverticular bleeding

Diverticulosis management � IF ASYMPTOMATIC : LIFE STYLE MODIFICATIONS � If Diverticular bleeding : 80% resolve spontainiously need only resuscitation , then perform colonoscopy (6 week after the attack not during it due to risk of perforation ) to R/O CA �Resuscitation �Localization �Supportive care with blood products

Localization �Right colon is the source of diverticular bleeding in 50 -90% of patients �Possible reasons �Right colon diverticuli have wider necks and domes exposing vasa recta over a great length of injury �Thinner wall of the right colon � Colonoscopy after rapid preparation �Can localize site of bleeding �Offers possible therapeutic intervention (cautery, clip, etc)
 �A site of active bleeding was identified �Treated")
Diverticular bleeding Management ( Cauterization ) �A site of active bleeding was identified �Treated successfully with placement of two hemoclips

Surgical management of bleeding �Resection of the affected colon segment (segmental or sub total ) �Indications : Elective : 1 - pt with recurrent bleeding 2 - need for long term anticoagulation 3 - excessive blood loss can’t be tolerated Urgent : Active ongoing bleeding >6 units packed RBCs /24 hours

Diverticulitis �Diverticulitis refers to inflammation and infection associated with a diverticulum �It’s estimated to occur in 10% to 25% of people with diverticulosis
")
Pathophysiology � Peridiverticular and pericolic infection results from a perforation (either macroscopic or microscopic) of a diverticulum, which leads to contamination, contamination inflammation, and infection � Previously thought to be due to fecaliths causing increased diverticular pressure; this is really rare

Classification � 1 - Uncomplicated diverticulitis 75% Only inflammation , usually resolve without surgery Classic triad : *localized tenderness *fever *leukocytosis � 2 - Complicated diverticulitis With abscess , obstruction, diffuse peritonitis, fistulas Hinchy classification to assess severity

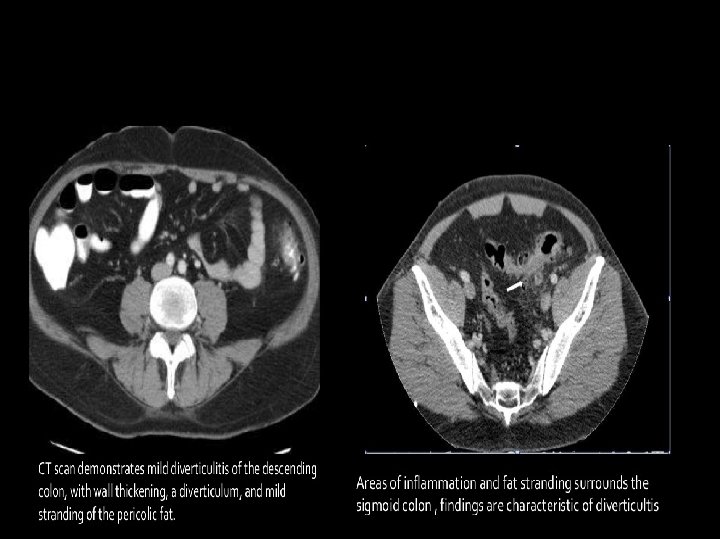
Invistigatons �Labs ; wbcs , C-Reactive Protein �Plain Radiography, Upright X-Ray; Free air under the diaphragm, air fluid level �Ultrasonography, Graded Compression; Thickened bowel loop with a target-like appearance �CT &MRI; Thickness of colonic wall, pericolic fat stranding, inflamed diverticula, abscess formation, free air, fistula formation �Colonoscopy ; Not recommended in acute phase of diverticulitis

Treatment of uncomplicated diverticulitis Management is always individualized according to pt , these are general guidelines ; �Bowel rest �Clear liquids for 2 -3 days then diet as tolerated �IV fluids �Antibiotics IV antibiotics that cover G-/anaerobe for 3 -5 days then switch to oral to complete 10 -14 days Ex : ceftriaxone + metronidazole Or – Ampicillin-sulfabactam _ Ticarcillin-Clauvalanate �May include percutaneous drainage of abscess

Surgery indications ; �After first or any complicated diverticulitis attack �After two or more episodes of uncomplicated
, or fistulas between")
Complicated diverticulitis �includes diverticulitis with abscess, obstruction, diffuse peritonitis (free perforation), or fistulas between the colon and adjacent structures. �The Hinchey staging system is often used to describe the severity of complicated diverticulitis

Hinchey staging system �Stage I includes colonic inflammation with an associated pericolic abscess �stage II includes colonic inflammation with a retroperitoneal or pelvic abscess �stage III is associated with purulent peritonitis �stage IV is associated with fecal peritonitis

�STAGE I and STAGE II is suitably managed with drainage and antibiotics �STAGE surgery III and STAGE IV usually requiring

Complicated diverticulitis �Diverticular abscess Usually identified on CT also can be seen in US and barium enema (tethering)
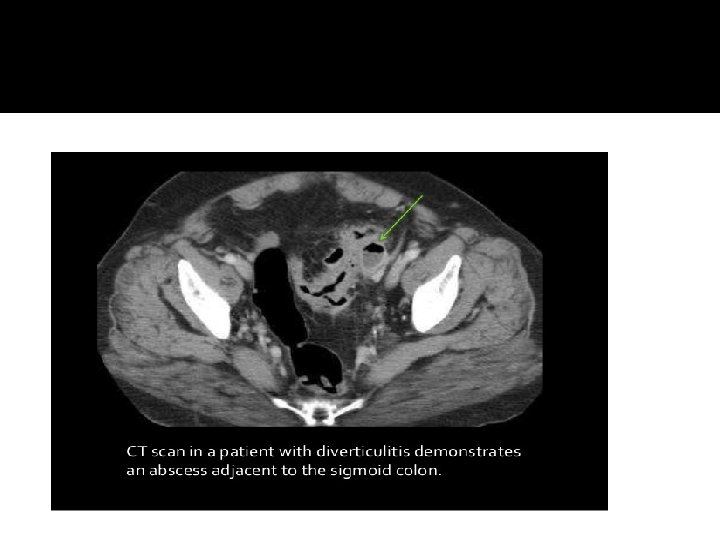

Management of abscess � Treatment depends on the patient’s overall clinical condition and the degree of peritoneal contamination and infection. � Small abscesses <2 cm may resolve with antibiotic therapy � Patient with larger abscesses or those who falls to improve with antibiotics CT guided percutaneous drainage + AB � Colonic resection is indicated for those who develop either recurrent diverticulitis or another abscess Urgent or emergent laparotomy may be required If ; 1 -An abscess is inaccessible to percutaneous drainage, 2 -The patient’s condition deteriorates or fails to improve, 3 - The patient presents with free intra-abdominal air or peritonitis �

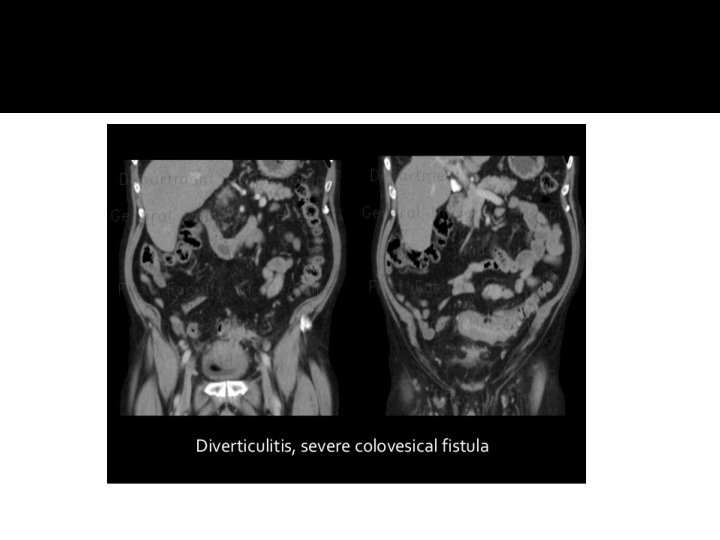
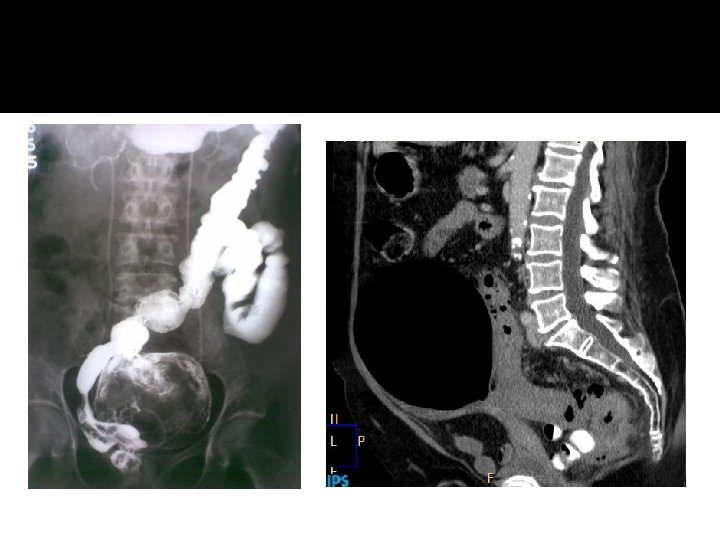
Fistulas � Occurs in up to 80% �requiring surgery �Major of cases types �Colovesical fistula 65% �Colovaginal 25% �Coloenteric, colouterine 10%

�COLOVESICAL, COLOUTERINE AND COLOVAGINAL FISTULAE

Fistulas �–Symptoms�Passage of gas and stool from the affected organ Colovesical fistula: �pneumaturia, dysuria, fecaluria � 50% of patients can have diarrhoea and passage of urine per rectum Diagnosis �CT: thickened bladder with associated colonic diverticuli adjacent and air in the bladder �BE: direct visualization of fistula track only occurs in 20 -26% of cases �Flexible sigmoidoscopy

generalised peritonitis Surgery is principally directed to control sepsis in the peritoneum and circulation � Vigorous resuscitation and antibiotic therapy is still warranted � Opoid analgesia � Oxygen therapy � Urinary catheter to assess hourly urine out put � Resection of sigmoid colon and colorectal anastomosis � Primary resection and anastomosis after on table lavage in selected case � Hartman’s procedure : Resection of sigmoid colon with formation of end colostomy , rectal stump (two stage. . 3 month later colostomy takedown and colorectal anastomosis ) We do it when condition do not favour primary anastomosis �

obstruction/stricture �Symptoms: pain, increasing constipation, passage of ribbon like stools � However majority of patient presents with classic symptoms of large bowel obstruction �Diagnosis is confirmed by ; patient’s history physical examinations radiological confirmation either by contrast enema or CT with oral/rectal contrast

�Patients with incomplete obstruction often respond to fluid resuscitation nasogastric suction and gentle, low volume water or Gastrografin enemas. �Relief of obstruction allows full bowel preparation and elective resection. � A high-volume oral bowel preparation is contraindicated in the presence of obstructive symptoms. �Obstruction that does not rapidly respond to medical management mandates laparotomy.

Surgery � Hartman’s resection and resection with primary anastomosis rarely with loop ostomy is the procedure of choice.

Giant Colonic Diverticulum �Extremly rare �Most occur on the antimesenteric side of the sigmoid colon �Pts may be asymptomatic or may present with vague abdominal complaints such as pain, nausea, or constipation. � Barium enema is usually diagnostic. �Complications of a giant diverticulum include , stasis , perforation, obstruction, and volvulus. �Resection of the involved colon and diverticulum is recommended

Right-Sided Diverticula �The cecum and ascending colon �A true solitary diverticulum �more often in younger patients than do left- sided �more common in people of Asian descent than in other populations �Most patients with right-sided diverticula are asymptomatic �they are often thought to suffer from acute appendicitis, and the diagnosis of right-sided diverticulitis is subsequently made in the operating room.

Right-Sided Diverticula…. con �. If there is a single large diverticulum and minimal inflammation, diverticulectomy may be performed, but an ileocecal resection is usually the preferred operation in this setting

�schwartzs-principles-of-surgery-tenth- edition. pdf �Bailey & Love’s Short Practice of Surgery 27 th Edition �Step-up to surgery Stanley Zaslau, Richard A. Vaughan. - Second edition.

� Thank you
- Slides: 45