Diuretics Nephron Speed of primary urine formation 120


 membrane Na+ enters a cell 1) with the concentration gradient 2) with")
 ( 1% of volume of")




 Effective even in a case of decreased glomerular filtration less than 10")





 Indications 1. 2. 3. 4. 5. Oedema in case of chronic cardiac")

 ECFV Depletion Hypercalcemia Hyponatremia Hypokalemia Metabolic Alkalosis Hyperuricemia Hypomagnesemia Hyperglycemia")

")
 Duration of action")







 2. Dichlothiaside + triamteren")
")


")
")


")

: - i. v. dropply – 1 ml")
 Dinoproston (prostaglandin E 2) • They cause rhythmic contractions")
 bleedings Absolutely contraindicated for labour")
- Slides: 45
Diuretics
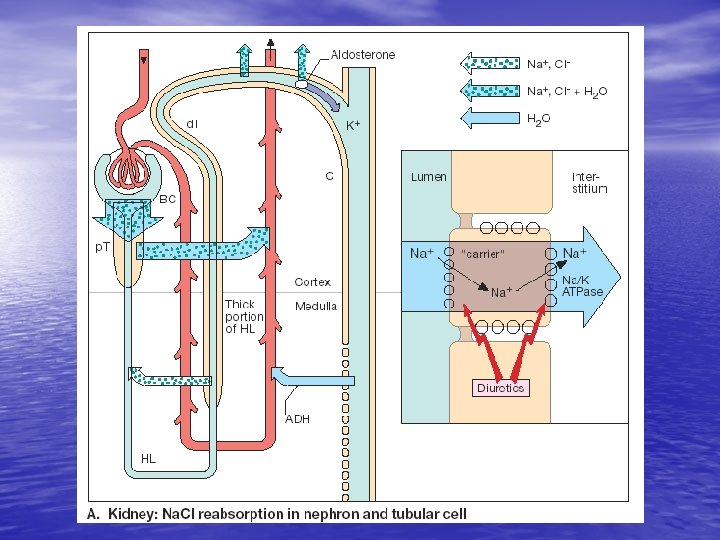
Nephron Speed of primary urine formation – 120– 127 ml/min There about 1 mln. nephrons in a kidney, reabsorbtive surface of which is – 6 -8 m 2. Along the nephron 99% of ultrafiltrate is reabsorbed and 1. 2 -1. 5 l of secondary urine forms from 150 -200 l of primary urine.
Apical (lumenal) membrane Na+ enters a cell 1) with the concentration gradient 2) with the help of protein transporters – permeases (synthesized under the influence of aldosterone) Basal membrane Na+ enters interstitial space against concentration gradient with energy consumption and with the help of specific transport systems (K+, Na+-ATPases, c. АMPadenilatcyclases and phosphodiesterases, etc. )
Filtration Reabsorbtion Primary urine Quantity of diuresis (secondary urine) ( 1% of volume of primary urine) Norm Increasing of filtration for 10% Decreasing of reabsorbtion for 10%
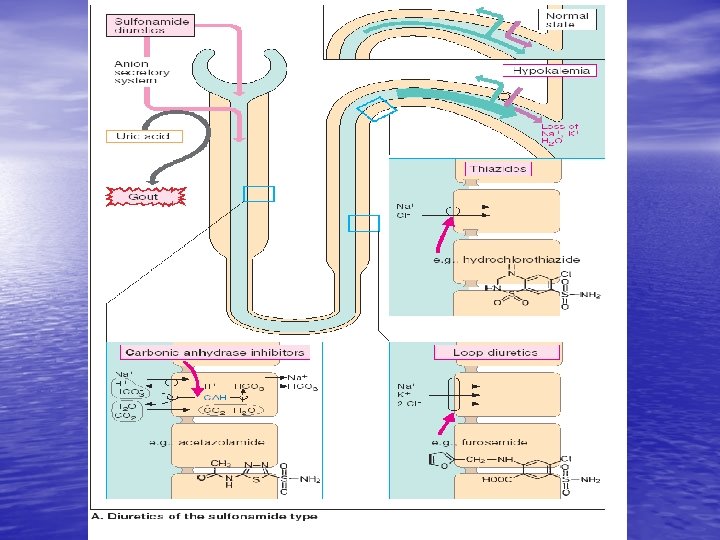
1 – vascular glomerulus with capsule; 2 – proximal tubule; 3 – descendent part of loop of Henle; 4 – ascendent part of loop of Henle; 5 – distal tubule; 6 – collective tubules. Classification of diuretics according to place of dominant action I Mostly act on beginning part of distal nephral canalicules : dichlothiasid, cyclomethiasid, clopamid (brinaldix), oxodolin (chlortalidon, hygroton) ІІ Act on ascendent part of loop of Henle (“loop” diuretics) : furosemide (lasix), etacrynic acid (uregit), bufenox ІІІ Act on ending part of distal nephral canalicules and collective tubules (potassium sparing diuretics): triamterene, amiloride, spironolactone ІV Act along the whole nephral canalicules: mannitol, urea (carbamide) V Act on proximal nephral canalicules: euphylline
Classification of diuretics according to power of action І Strong (slowing down of Na+ reabsorbtion for 10 – 20 %) – loop diuretics furosemide, etacrynic acid, clopamide, bufenox ІІ Medial power of action (slowing down of Na+ reabsorbtion for 5 – 8 %) dichlothiaside, oxodoline ІІІ Light (slowing down of Na+ reabsorbtion no more than for 3 %) diacarb, spironolactone, amiloride, triamteren, xantines (theophylline)
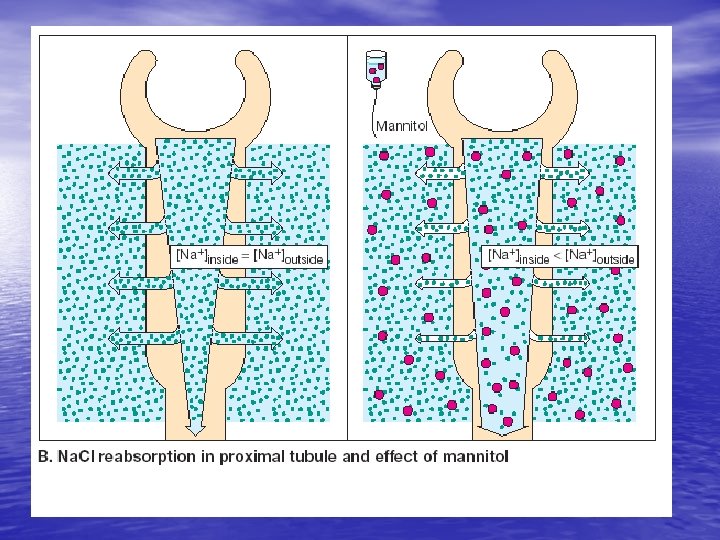
Mannitol 15 % solution rapid intravenous introduction dehydrating action diuretic action intravenous dropping introduction diuretic action
Mannitol Indications 1. 2. 3. 4. 5. 6. Brain oedema (in case of maintaining of HEB permeability) Toxic lung oedema (poisoning with gasoline, gass, formaline, skipidar etc. ) Larynx oedema of allergic or inflammatory genesis Performing of forced diuresis (poisoning with barbiturates, salycylates, sulphonamides, PASA, metanole, boric acid, haemolytic poisons, antifreezers; in case of transfusion of incompatible blood, massive hemoglobinuria etc. In oliguric phase of acute kidney insufficiency Burns, osteomielitis, peritonitis, sepsis (to improve elimination out of the organism toxic compounds which formed from destroyed tissues) Contraindications Acute cardiac insufficiency, arterial hypertension, skull trauma, intracranial hemorrhages
Furosemide (lazix) Effective even in a case of decreased glomerular filtration less than 10 ml/min. (norm – 120 -127 ml/min) Indications 1. Acute left ventricular insufficiency, lung oedema 2. Chronic cardiac insufficiency 3. Arterial hypertension, especially hypertensive crisis 4. Brain oedema of any etiology 5. Acute kidney insufficiency 6. Performing of forced diuresis 7. For excretion of Calcium ions (hypervitaminosis D)
Furosemid
Side effects of furosemide 1. Hypopotassiumaemia, hypopotassiumhystia 2. Hypovolemia, vascular collapse, hyposodiumaemia, hypocalciumaemia, hypochloraemia, metabolic alkalosis 3. Ototoxic action (deafness) 4. Contrinsulinic action (manifestation of latent diabetes mellitus) 5. Formation of oxalate and phosphate stones in urinary tract 6. Decreasing of secretion of uric acid (acute attack of gout) 7. It should not be combined with antibiotics
Furosemide
Furosemide
Furosemide
Dichlothiaside (hydrochlorthiaside) Indications 1. 2. 3. 4. 5. Oedema in case of chronic cardiac insufficiency Oedema in case of chronic pathology of liver and kidneys Long-term treatment of arterial hypertension Diabetes insipidus Retention of Ca ions Side effects 1. Hypopotassiumaemia, hypopotassiumhystia 2. Hypochloraemic alkalosis 3. Retention of uric acid - artralgy, acute attack of gout, chronic nephropathy 4. Hyposodiumaemia of dilution: nausea, vomitting, diarrhea, weakness 5. Pancreatitis
THERAPEUTIC EFFECTS Increase Na Excretion to 5% of Filtered Load Treatment for Mild Edema Decrease Ca Excretion Treatment for Hypertension Treatment for Nephrogenic Diabetes Insipidus Treatment for Calcium Nephrolithiasis
ADVERSE EFFECTS Dichlothiaside (hydrochlorthiaside) ECFV Depletion Hypercalcemia Hyponatremia Hypokalemia Metabolic Alkalosis Hyperuricemia Hypomagnesemia Hyperglycemia Impotence Increased LDL (Renal Cell Carcinoma? ? )
Post diuresis Sodium Retention!! – ricochet effect
Indapamide (ariphone – sulphamoil benzamide)
Pharmacokinetics of some diuretics Drug Way of administration Latent period (onset) Duration of action Sulfonyl derivates Oxodolin (chlortalidon, hygroton) orally 2 -4 hours 3 days Clopamide orally 1 -3 hours 8 -18 (till 24) hours Bufenox (bumetanide) In muscle i. V. 20 -40 min. 2 -5 min. 4 -6 hours 1 -3 hours Potassium-, magnesium-sparing Spironolactone orally 2 -5 days 2 -3 days Triamteren (pterophen) orally 20 -30 min. 6 -8 hours Amiloride orally 2 hours 24 hour
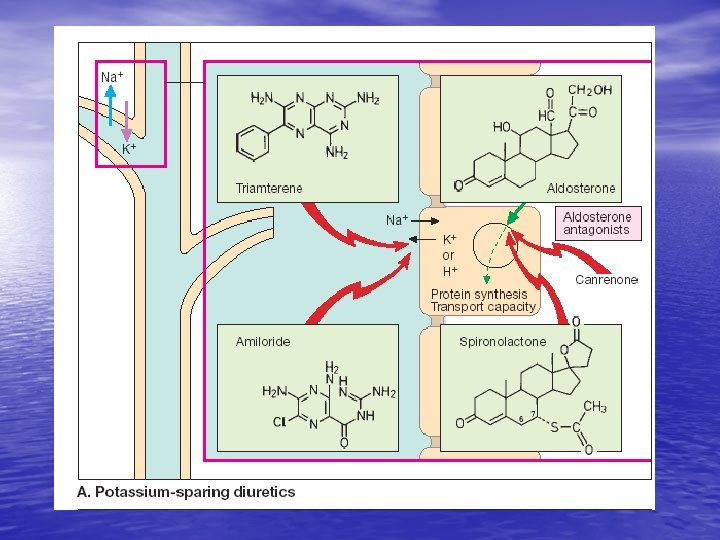
K-Sparing Diuretics Triamterene Spironolactone Amiloride
THERAPEUTIC EFFECTS Enhance Natriuresis Caused by Other Diuretics Prevent Hypokalemia Used in Combination with Loop & Thiazide Diuretics Block Na Channels Treatment for Liddle’s Syndromen (pseudoaldosteronism) Treatment for Lithium. Induced Diabetes Insipidus
ADVERSE EFFECTS Amiloride Hyperkalemia Triamterene Hyperkalemia Renal Stones Interstitial Nephritis Megaloblastosis
MINERALOCORTICOID RECEPTOR ANTAGONISTS Also Called: • K-Sparing Diuretics • Aldosterone Antagonists Spironolactone Eplerenone
THERAPEUTIC EFFECTS Used in Combination with Loop & Thiazide Diuretics Enhances Natriuresis Caused by Other Diuretics Prevents Hypokalemia Blocks Aldosterone Treatment for Primary Hyper -aldosteronism Treatment for Heart Failure Treatment for Edema of Liver Cirrhosis Treatment for Hypertension
spironolactone ADVERSE EFFECTS Hyperkalemia Metabolic Acidosis Gastritis Peptic Ulcers Deepening of Voice Impotence CNS Side Effects Gynecomastia Hirsutism Menstrual Irregularities
Spironolactone
Combined administration of diuretics 1. Mannitol + furosemide (etacrynic acid) 2. Dichlothiaside + triamteren (spironolactone) 3. Furosemide + spironolactone 4. Furosemide (excretes Calcium ions) + dichlothiaside (retains Calcium ions)
Triampur (triamteren + hydrochlorthiaside)
IMPORTANT DRUG INTERACTIONS NSAIDS Salt Decongestants Probenecid ACE Inhibitors Beta-Blockers K Supplements K-Sparing Diuretics Heparin Ototoxic Drugs Diminished Diuretic Response Hyperkalemia. Induced by K-Sparing Diuretics Enhanced Ototoxicity of Loop Diuretics
kidney tea Fol. Orthosiphoni
Shots of birch tree (Gemmae Betulae)
Leaves of red bilberries (fol. Vitisidaeae)
Horse-tail Herba Equiseti
Blue corn-flowers (Flores Centaureae
Juniper berries (Fructus Juniperi)
Drugs effecting uterus contraction І Influence mostly on myometrium contraction 1. Increase rhythmic contraction Oxytocine, Pituitrine, Hyphotocine Dinoprost (prostaglandine F 2α ), Dinoproston (prostaglandine E 2 ), 2. Decrease contractions (tokolytic substances) Salbutamol, Fenoterol, Sodium oxybutyrate, Magnesium sulphate Diazoxide ІІ Increase mostly myometrium tone Ergometrini maleas Cotarnine chloride Ergotamine hydrotartrate Ergotal ІІІ Decrease tone of uterus cervix Atropine sulphate Dinoproston
For labour stimulation (rhythmic contraction of uterus): - i. v. dropply – 1 ml (5 Units) dissolve in 500 ml 5 % glucose - i. m or in cervix of uterus 0, 52, 0 Units for single injection For post labor atonic bleeding (it is necessary to provoke spastic contraction of uterus) 1 -2 ml i. m.
Dinoprost (prostaglandin F 2α ) Dinoproston (prostaglandin E 2) • They cause rhythmic contractions of uterus • For stimulation of labor, i. v. dropply • Initiate uterus contractions independently of the term of pregnancy • Uses only after hospital admission!
Ergometrini maleas – for stopping after labor atonic (hypotonic) bleedings Absolutely contraindicated for labour stimulation !!! Fungi Claviceps purpurea (Ergot) Secale cornutum