Disturbances of IntraCranial Pressure ICP and Hydrocephalus Andrew
 and Hydrocephalus Andrew Danks Chairman of Neurosurgery, MMC")
Disturbances of Intra-Cranial Pressure (ICP) and Hydrocephalus Andrew Danks Chairman of Neurosurgery, MMC

Significance of raised ICP depends clinical context § Fast vs Slow tempo l slow rise allows compensation • brain shift / moulding/atrophy • CSF shifts • even bone moulding / atrophy § Young child l splitting of sutures, head growth • can often allow compensation

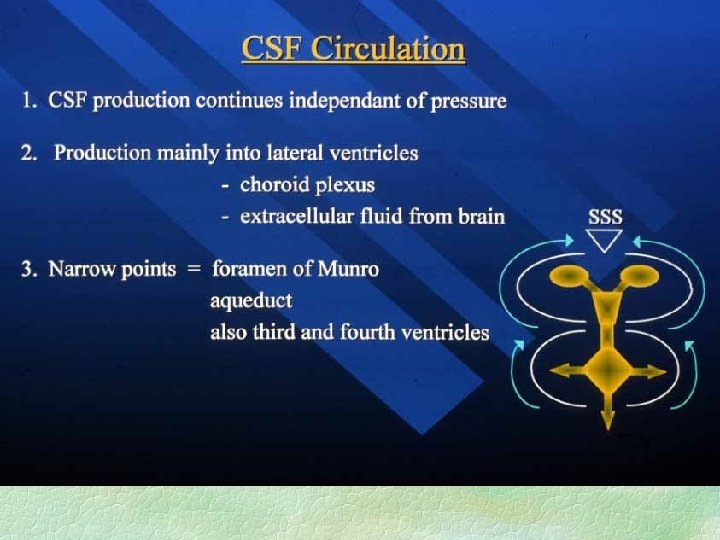
Normal ICP § Normally 10 -15 cm water in supine position l lower in young children § -5 to 0 cm water in standing position l at foramen of Munro (mid temple) § CSF actively secreted at 20 ml/hr or so § CSF resorbed at arachnoid villi in pressuredependant mechanism § CSF pressure is the driver for head growth

Benign Intracranial Hypertension § Chronic raised ICP l § § § up to 40 - 60 cm water no hydrocephalus / brain distortion normal brain function may get headaches, papilloedema, and visual loss due to raised venous or CSF pressure

Clinical Features of Chronically Raised ICP § Symptoms : l l l headache vomiting impaired mentation, conscious state § Signs : l l l papilloedema : vision at risk poor upgaze, 6 th nerve palsy impaired mentation, conscious state

Papilloedema

Common causes of acute ICP § § § § § Severe head injury Intracranial haematoma Tumour / abscess Infection - meningitis, encephalitis Metabolic Post operative swelling Ischaemic strokes Hydrocephalus Sub-arachnoid haemorrhage

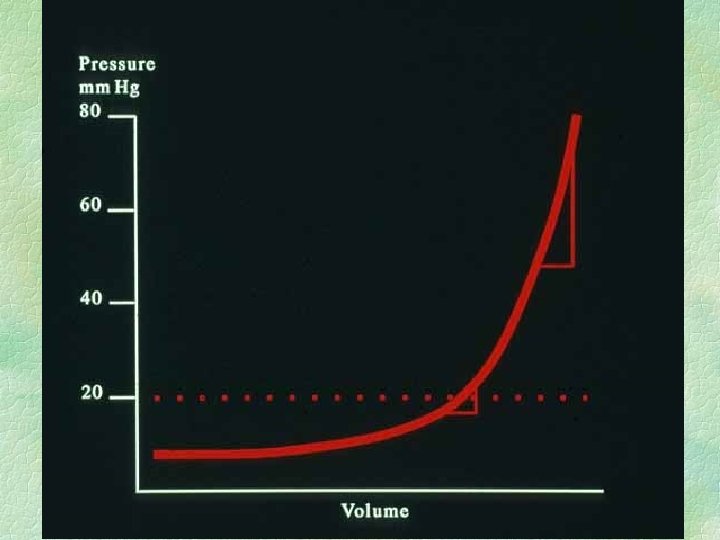
ICP Reflects : § Volume of contents / volume of cranium § contents = l l l brain blood CSF pathology : tumour, haematoma, etc oedema : intracellular / extracellular § normal ICP = 5 - 15 cm water, postural

CT and MRI show shapes of tissues, not pressure § Pressure can often be inferred § However, significant traps exist § in “acutely blocked shunt”, ventricles often are not dilated l l some pts have slit ventricles when controlled some pts do not dilate ventricles due to stiff walls, but pressure increased

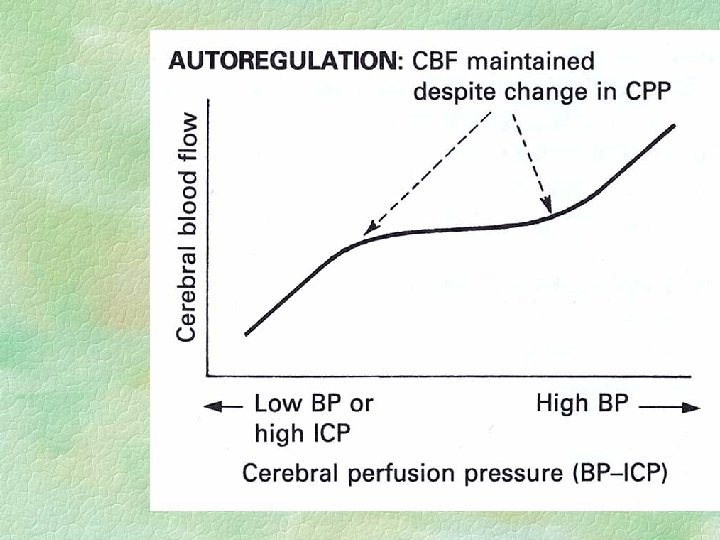
More important than ICP : § Cerebral perfusion pressure l l CPP = Arterial pressure - ICP accepted goal in ICU setting = 60 mm. Hg § Herniation l brain tissue forced between compartments • damage to this brain • further increased ICP
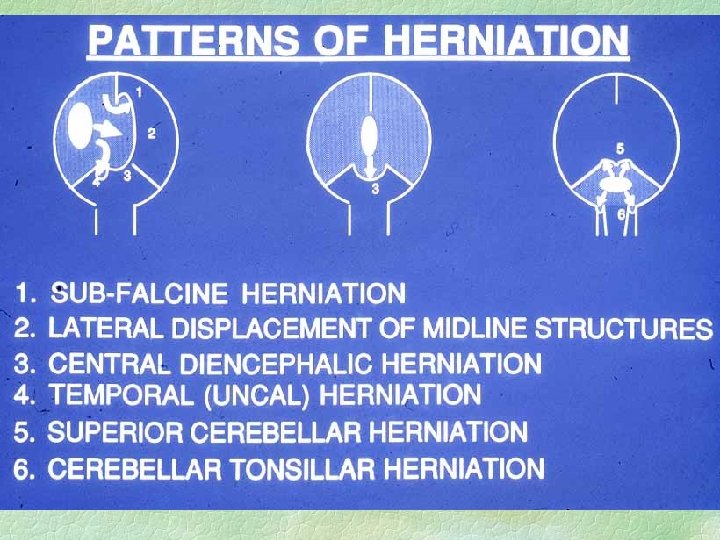

Consequences of herniation § Local damage in herniated tissue § infarction l vessel compression / traction § further oedema due to above § nerve damage due to pressure l 3 rd nerve § CSF entrapment - more pressure

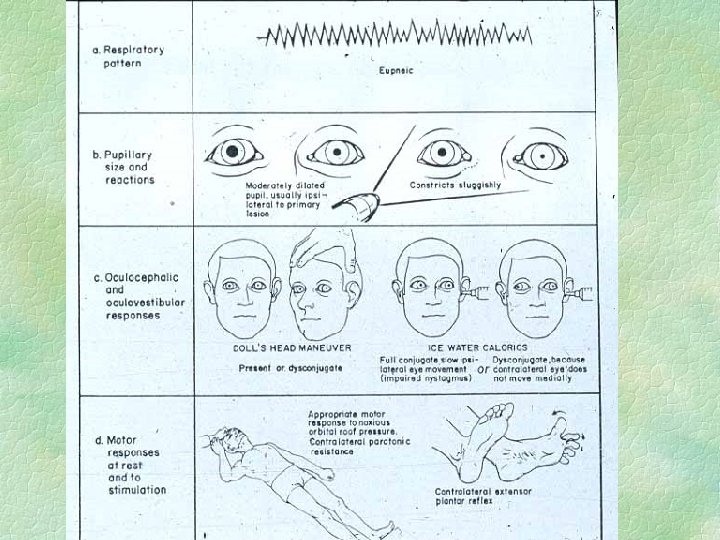
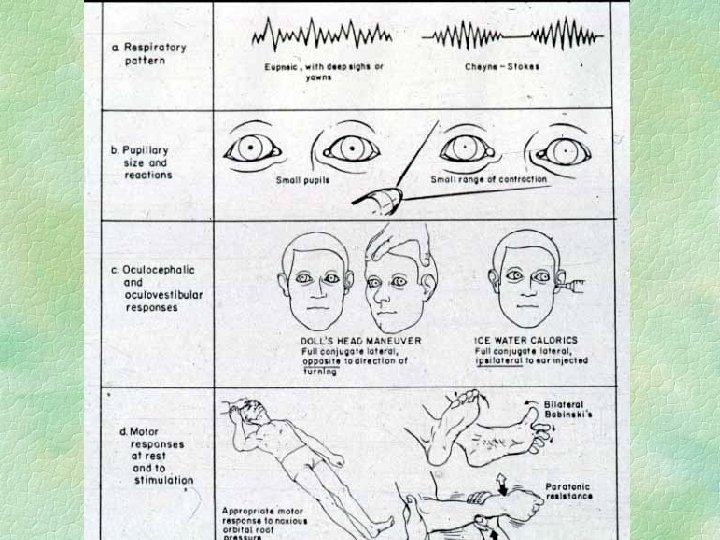
Acute trans-tentorial herniation unilateral § Medial temporal lobe forced into tentorial hiatus § Third nerve palsy, pupil first § mid-brain compression l l ipsilateral contralateral vs. opposite tentorial edge
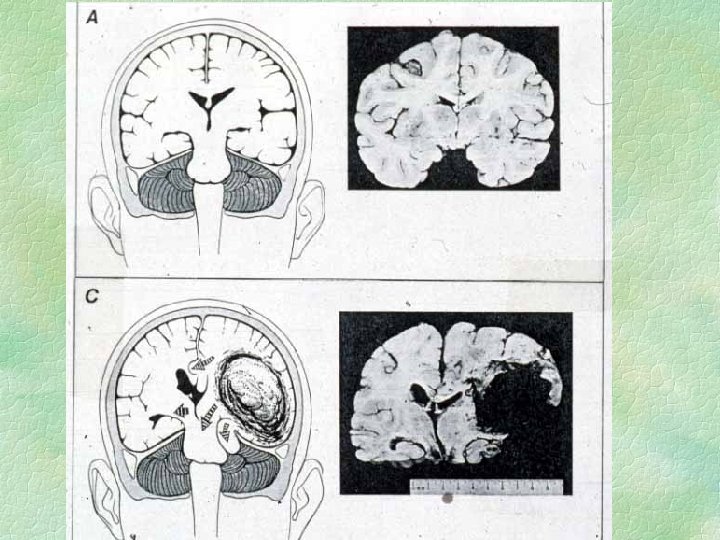
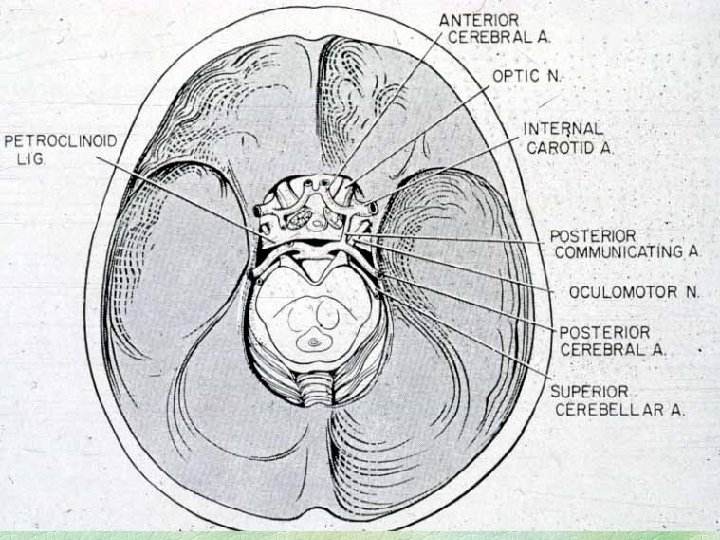

Detail of lateral tentorial herniation
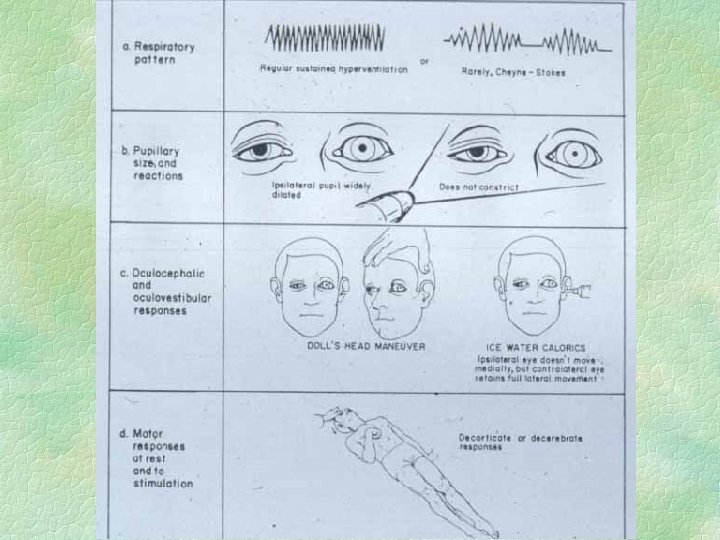
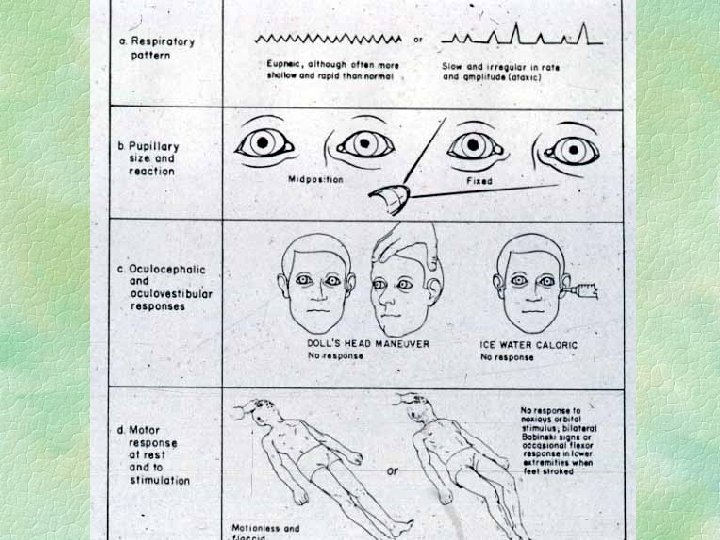

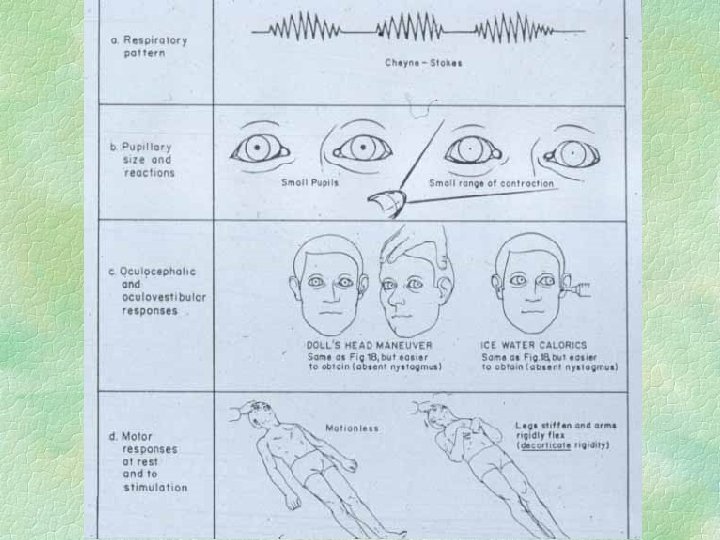
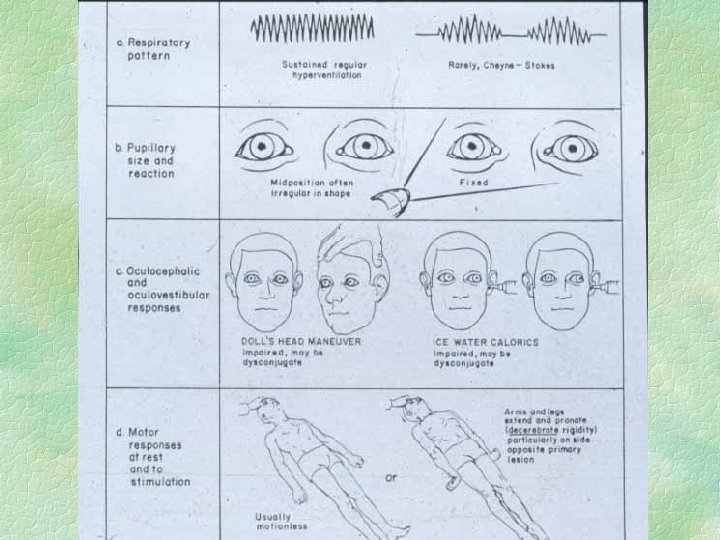
Acute trans-tentorial herniation symmetrical § Diencephalon symmetrically forced into tentorial hiatus § does NOT catch third nerve § symmetrical decline of conscious state with posturing etc. § pupils small not dilated

Symmetrical tentorial herniation

Treatment of Acutely Raised ICP § § § Diagnose and treat concurrently ETT, hyperventilate and paralyse Mannitol (1 gm/kg) CT call neurosurgeon : specific treatments : l l l drain CSF in hydrocephalus evacuate haematoma dexamethasone for tumour oedema

Complicating factors in emergency neurosurgery § § § A B C D dilutional : low sodium E epilepsy F fever : increases ICP, metabolism

Hydrocephalus § Acute vs. chronic § adult vs. infant l head size § non-communicating vs. communicating l l former may be prone to rapid decline LP dangerous in former, helpful in latter

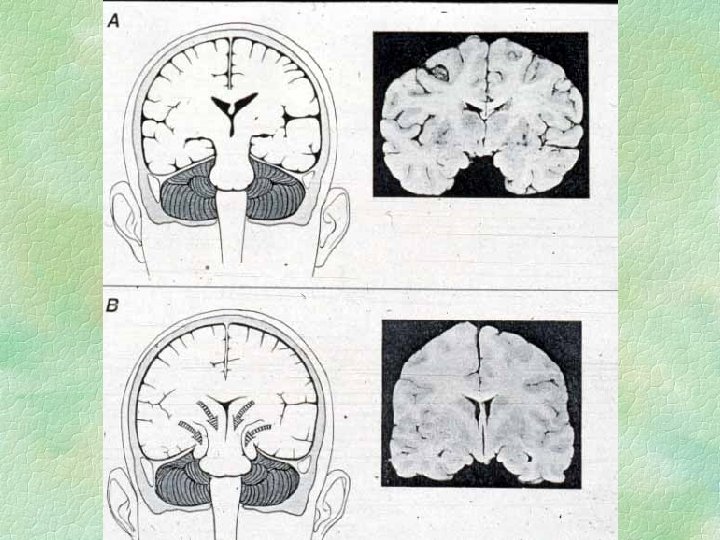
Clinical Hydrocephalic Syndromes § acute hydrocephalus l headache, vomiting, drowsiness, declining consciousness, papilloedema § chronic hydrocephalus in child l big head, headache, papilloedema, false localizing signs § “normal Pressure” hydrocephalus l triad of gait apraxia, incontinence, dementia l may be sequel to SAH, meningitis, etc § compensated hydrocephalus l chronic ventriculomegaly, stabilized, asymptomatic § differential includes cerebral atrophy

Causes of hydrocephalus § Non-communicating : l l l tumour esp. in posterior fossa aqueduct stenosis/blockage Arnold - Chiari malformation § Communicating : l l congenital sludge in SA space : SAH, meningitis blocked arachnoid villi congenital
 • At 6 yrs :")
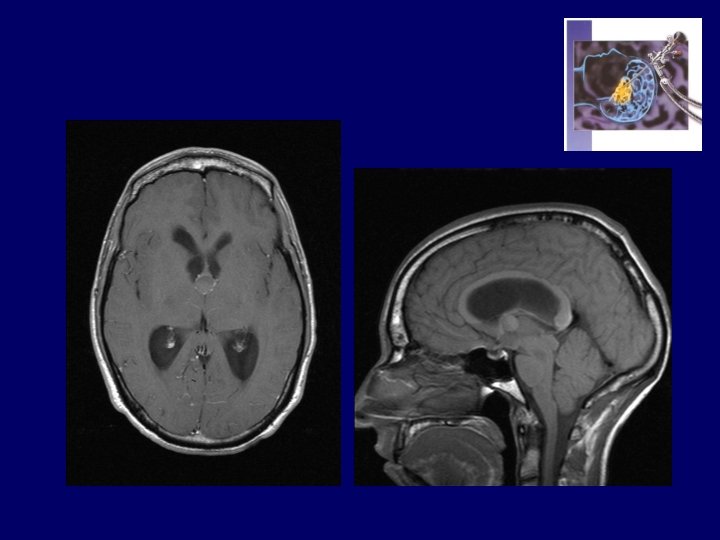
Obs. ZI…. Thomas ( 13 - 01 1992 ) • At 6 yrs : headaches, drowsiness, rapid visual deterioration • 24 -08 -1998 : OD = 4/10 OG = 2/10 • CT and MRI : Craniopharyngioma Hydrocephalus • 30 -08 -1998 : OD = 1/20 OG = 1/10 VP Shunt • 02 -09 -1998 : OD = 3/10 OG = 2/10 • 03 -09 -1998 : Total resection of C. • 18 -02 -1999 : OD = 1/30 OG = 0

Modern Management of Hydrocephalus SHUNTS ‘ COST

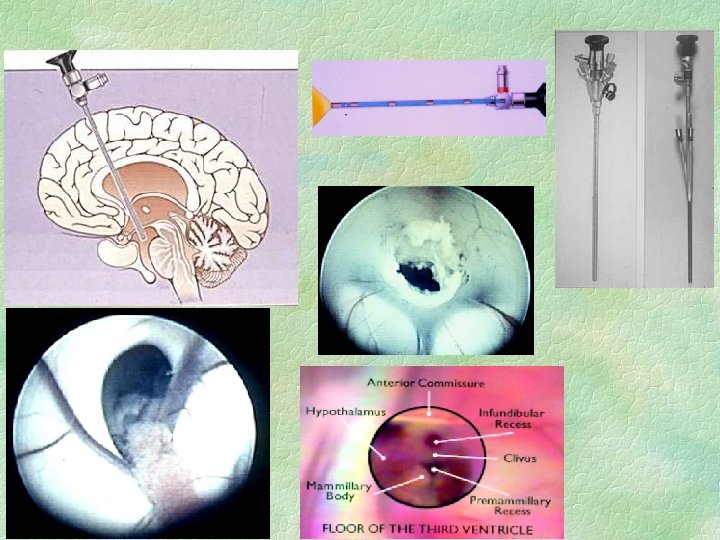
Treatment of hydrocephalus § Treat cause if possible l § § eg remove tumour, treat meningitis External ventricular drain if acute / infected Lumbar puncture, IF COMMUNICATING Ventriculo-peritoneal shunt - with valve Other shunts : l V-Atrial, V-pleural, Lumbo- p § Endoscopic 3 rd ventriculostomy l treatment of choice in aqueduct stenosis, 4 th ventricle obstruction

Common problems with V-P shunts § Blockage - early or late § Infection - acute or delayed up to 6 months § Over-drainage l l l subdural hygroma/haematoma slit ventricles, small head to due to chronic effects on head growth headaches

Cumulative shunt survival Long term shunt survival Sigma 1. 0 Standard Delta . 8 . 6 . 4 p=. 04 . 2 0 1 Time (years) 2 3 4 5 6 C. Sainte Rose

ETV’s may also fail

Has this person got a blocked shunt ? § § Headache, drowsiness, N&V GCS, eye movements, fundi Does the valve pump and refill ? Scan and compare l l l Very closely, slice by slice The trap is interval decrease in vents after shunting, which may take 1 year, then later increase due to blockage Catheter position, disconnection (XR series) § N/S Registrar

Intracranial haemorrhages Traumatic Spontaneous Extradural Y Rare Subdural Y acute/chronic Sometimes Subarachnoid Y Y Intracerebral Y Y Intraventricular Y Y

Intracerebral haemorrhage § Presentation – l Acute stroke, declining consciousness, seizure § Cause – l Aneurysm, AVM, trauma, hypertension § Surgical evacuation in minority l l l Young patients, larger lobar haematomas Cerebellar haematomas Not elderly, basal ganglia

Presentation of SAH § 5 ways

Presentation of SAH § § § sudden death sudden LOC, recovering or persisting. SUDDEN severe headache meningeal signs / symptoms lumbago, several days later

Diagnosis of SAH § 2 steps

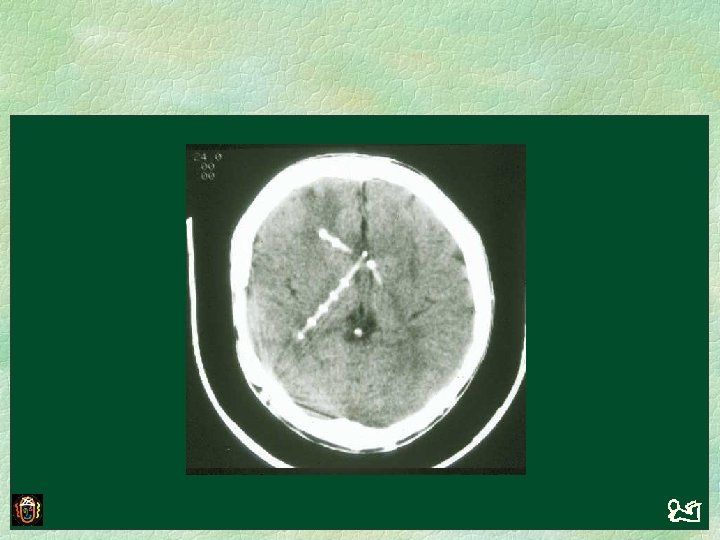
Diagnosis of SAH § CT : acute blood is white § LP - if and only if CT is normal l l best after 12 hours to allow xanthochromia experienced operator - traumatic tap problematic

Same patient, GCS 12

2 different patients

WHO Grading of SAH patients § § § 1 : normal neurologically 2 : GCS 13 -14 3 : GCS 13 -14, focal cerebral signs 4 : GCS 9 -12 5 : GCS < 9

Early management of SAH § acute resusc, ETT and ICU if GCS < 8 § Otherwise, monitor closely § Immediate transfer to neurosurgery l CTA, DSA, control aneurysm § CONTROL BP TO PREVENT RE-BLEED l l Start nimodipine, control pain with small doses of narcotics Hydrallazine, clonidine § Early deterioration : rebleed, hydrocephalus
- Slides: 53