Disseminated Intravascular Coagulation Robert R Zaid D O

Disseminated Intravascular Coagulation Robert R. Zaid D. O. Genesys Regional Medical Center PGY-I

Barcelona - Gaudi

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Primarily a thrombotic process – Systemic process producing both thrombosis and hemorrhage – Also called consumption coagulopathy and defibrination syndrome 1 – Its clinical manifestation may be widespread hemorrhage in acute, fulminant cases 2. 1. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY 2. Uptodote, 2005, www. utdol. com, Clinical feadures, diagnosis and teratment of disseminated intravascular coagulation

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Basic pathophysiology – Entry into the circulation of procoagulant substances • Trigger systemic activation of the coagulation system and platelets • Lead to the disseminated deposition of fibrinplatelet thrombi. – Procoagulant stimulus is tissue factor (most cases) • Lipoprotein • Not normally exposed to blood. – Tissue factor gains access to blood by • Tissue injury, • Malignant cells, • Expression on the surfaces of monocytes and endothelial cells by inflammatory mediators. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Stein B, Fuster V, Israel DH, et al. Platelet inhibitor agents in cardiovascular disease: an update. J Am Coll Cardiol. 1989; 14: 813– 836.

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Tissue factor triggers – Thrombin • Protease • Induces fibrin formation and platelet activation • Other procoagulants – Cysteine protease – Mucin – Trypsin Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Acute DIC – Coagulation factors are consumed at a rate in excess of the capacity of the liver to synthesize them, – Platelets are consumed in excess of the capacity of bone marrow megakaryocytes to release them. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

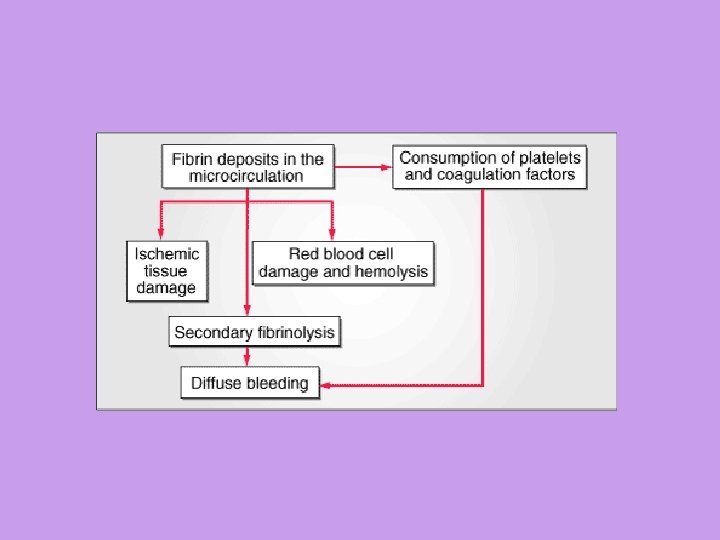
Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Laboratory manifestations – Prolonged prothrombin time (PT) – Prolonged Activated partial thromboplastin time (a. PTT) – Thrombocytopenia. – Increased fibrin formation • Stimulates compensatory process of secondary fibrinolysis, • Plasminogen activators generate plasmin to digest fibrin (and fibrinogen) into fibrin(ogen) degradation products (FDPs). – FDPs are potent circulating anticoagulants that contribute further to the bleeding manifestations of DIC. • Intravascular fibrin deposition cause fragmentation of red blood cells and lead to the appearance of schistocytes in blood smears • Hemolytic anemia is unusual in DIC. • Microvascular thrombosis in DIC can compromise the blood supply to some organs and lead to multiorgan failure Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris

Citadel Park

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • DIC always has an underlying etiology – Must be identified and eliminated to treat the coagulopathy successfully. – The development of DIC in many of these disorders is associated with an unfavorable outcome 1. • Occurs in 1% of hospitalized patients 2 • Mortality rate approaches 40 -80% 1. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY 2. Uptodote, 2005, www. utdol. com, Clinical feadures, diagnosis and teratment of disseminated intravascular coagulation

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Causes – Infection • Most common cause of DIC. • The syndrome particularly is associated with gram-negative or gram-positive sepsis • Can be triggered by a variety of other – – Bacterial Fungal Viral Rickettsial, and protozoal microorganisms. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Obstetrics – The placenta and uterine contents are rich sources of • Tissue factor • Other procoagulants that normally are excluded from the maternal circulation Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

La Familia

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris – Clinical manifestations of DIC may accompany obstetric complications, especially in the third trimester. • These syndromes range from – Acute, fulminant, and often fatal DIC in amniotic fluid embolism » Blood is exposed to large amounts of tissue factor in a short period of time creating large amounts of thrombin » Multiorgan failure – Chronic or subacute DIC with a retained dead fetus. » Exposure to small amounts of tissue factor Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris – Other obstetric problems associated with DIC include • Abruptio placentae • Toxemia • Septic abortion. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Clinical manifestations – Determined by • Nature • Intensity • Duration of the underlying stimulus. – Chronicity • Low-grade DIC is often asymptomatic – Diagnosed only by laboratory abnormalities. – Bleeding is most common clinical finding » Generalized or widespread ecchymoses • Chronic disease – Thrombotic complications » Trousseau's syndrome in cancer » Gangrene of the digits or extremities » Hemorrhagic necrosis of the skin » Purpura fulminans – Enhanced by • Coexistence of liver disease Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Candy Factory

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Diagnosis of severe, acute (easy) – Prolongation of PT, a. PTT and Thrombin time • Due to consumption and inhibitiion of clotting factors – Thrombocytopenia – Fibrin degradatin products • Increased due to secondary fibrinolysis – Measured by latex agglutination or D-dimer assays. – Schistocytes may be seen in the peripheral blood smear • Neither sensitive nor specific for DIC. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Chronic or compensated forms of DIC – Highly variable patterns of abnormalities in "DIC screen" coagulation tests. – Increased FDPs and prolonged PT are generally more sensitive measures than are abnormalities of the a. PTT and platelet count. – Overcompensated synthesis of consumed clotting factors and platelets in some chronic forms • Cause shortening of the PT and a. PTT and/or thrombocytosis • Though, elevated levels of FDPs indicate secondary fibrinolysis in such cases. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Street entertainers

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Treatment – Identify underlying cause and treat – All otherapies are temporizing Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Asymptomatic patients with selflimited DIC – Have only laboratory manifestations of the coagulopathy – No treatment may be necessary. Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Actively bleeding or who are at high risk of bleeding, – Blood component treatments of choice • Transfusions of platelets – Improve thrombocytopenia • Fresh-frozen plasma (FFP) – Replace all consumed coagulation factors and correct the prolonged PT and a. PTT. • Large volumes of plasma in severe cases – The theoretical concern that these blood products may "fuel the fire" and exacerbate the DIC has not been supported by clinical experience Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Special cases – Profound hypofibrinogenemia • Additional transfusion of cryoprecipitate, • Plasma concentrate enriched in fibrinogen – Sepsis • Infusion of antithrombin III concentrate may be considered as an adjunctive measure Schafer, A. , I. , Cecil Textbook of Medicine, Saunders, 2004, chapter 179, HEMORRHAGIC DISORDERS: DISSEMINATED INTRAVASCULAR COAGULATION, LIVER FAILURE, AND VITAMIN K DEFICIENCY

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Pharmacologic inhibitors of coagulation and fibrinolysis – Heparin – Theoretical benefit • • It blocks thrombin and the secondary fibrinolysis. Might exacerbate the bleeding tendency – Usually reserved for – Forms manifested by » Thrombosis » Acrocyanosis » Cancer » Vascular malformations » Retained dead fetus » Acute promyelocytic leukemia.

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Antifibrinolytic agents, – ε-aminocaproic acid and tranexamic acid – Generally are contraindicated • May precipitate thrombosis – May be effective in decreasing lifethreatening bleeding

Festivals
")
Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • XIGRIS® (Lilly) Drotrecogin alfa (activated) – Recombinant form of human Activated Protein C

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • • General Pharmacology Activated Protein C – Antithrombotic effect – Inhibits Factors Va and VIIIa. • • • Indirect profibrinolytic activity through its ability to inhibit plasminogen activator inhibitor-1 (PAI-1) Limits generation of activated thrombinactivatable-fibrinolysis-inhibitor. In vitro data indicate that Activated Protein C may exert an anti-inflammatory effect by inhibiting human tumor necrosis factor production by monocytes – Blocks leukocyte adhesion to selectins – Limits the thrombin-induced inflammatory responses within the microvascular endothelium.

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Clinical study (PROWESS) – 1690 patients with severe sepsis – Entry criteria included a systemic inflammatory response presumed due to infection and at least one associated acute organ dysfunction – The study was terminated after a planned interim analysis due to significantly lower mortality in patients on Xigris than in patients on placebo • (210/850, 25% vs. 259/840, 31% p=0. 005).

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • INDICATIONS AND USAGE – Xigris is indicated for the reduction of mortality in adult patients with severe sepsis (sepsis associated with acute organ dysfunction) who have a high risk of death (APACHE II)

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Contraindications – Active internal bleeding – Recent (within 3 months) hemorrhagic stroke – Recent (within 2 months) intracranial or intraspinal surgery, or severe head trauma – Trauma with an increased risk of lifethreatening bleeding – Presence of an epidural catheter – Intracranial neoplasm or mass lesion or evidence of cerebral herniation

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • Warnings – – – Concurrent therapeutic dosing of heparin to treat an active thrombotic or embolic event Platelet count <30, 000 × 10 6 /L, even if the platelet count is increased after transfusions Prothrombin time-INR >3. 0 Recent (within 6 weeks) gastrointestinal bleeding Recent administration (within 3 days) of thrombolytic therapy Recent administration (within 7 days) of oral anticoagulants or glycoprotein IIb/IIIa inhibitors Recent administration (within 7 days) of aspirin >650 mg per day or other platelet inhibitors Recent (within 3 months) ischemic stroke Intracranial arteriovenous malformation or aneurysm Known bleeding diathesis Chronic severe hepatic disease Any other condition in which bleeding constitutes a significant hazard or would be particularly difficult to manage because of its location.

Disseminated Intravascular Coagulation -Background -Pathophysiology -Etiology -Clinical Manifestations -Diagnosis -Treatment -Xigris • DOSAGE AND ADMINISTRATION – Xigris should be administered intravenously at an infusion rate of 24 µg/kg/hr for a total duration of infusion of 96 hours.

Any questions?
- Slides: 37