Disorders of Lipid Metabolism By Dr Nermin Ahmed

Disorders of Lipid Metabolism By Dr. Nermin Ahmed Sheriba Prof. Of Endocrinology

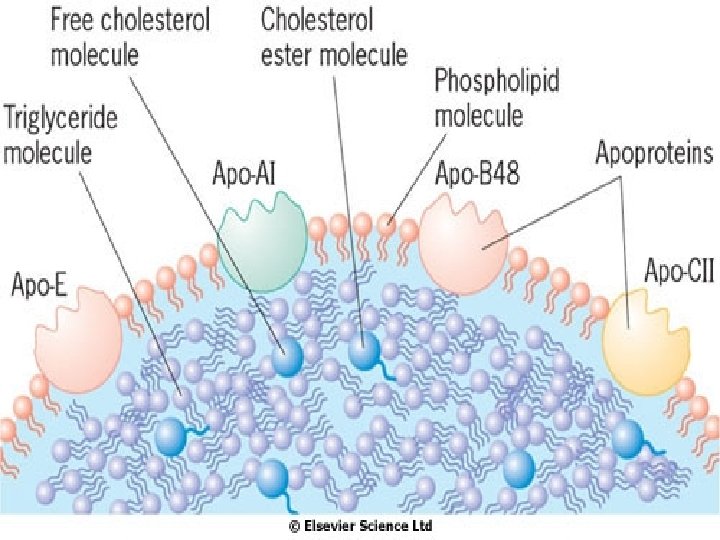
• Lipids are insoluble in water and are transported in blood stream as macromolecular complexes. • In these complexes, lipids (triglycerides, cholesterol and cholesterol esters) are surrounded by phospholipids. • Proteins (apoproteins) embedded into the surface of these particles exert stabilizing function and allow the particles to be recognized by receptors in the liver and peripheral tissues.
 • Intermediate density lipoproteins •")
Lipoproteins • Chylomicrons • Very low density lipoproteins (VLDL) • Intermediate density lipoproteins • Low density lipoproteins (LDL) • High density lipoproteins (HDL)

Chylomicrons • They are synthesized in the small intestine postprandially passing into the intestinal lymphatic drainage to the thoracic duct to blood stream. • They provide the main mechanism for transporting the digestion products from small intestine to the liver and peripheral tissues.

• Each newly formed chylomicron contains apo B-48, A-II and aquire apo C-II and E from HDL in the blood stream. • Apo C-II: binds to specific receptors in adipose tissue, muscle and liver, allows the endothelial enzyme lipoprotein lipase to remove most of triglycerides giving rise to chylomicron remnant which is taken up by the liver.

Very Low Density Lipoproteins • These are synthesized and secreted by the liver and contain most of the endogenously synthesized triglyceride and a smaller quantity of cholesterol. • They are the body’s main source of energy during prolonged fasting. • In circulation, lipoprotein lipase removes triglyceride from VLDL to form intermediate density lipoprotein.

• Apo B-100 is an essential component of VLDL • Apo C-II and E are incorporated into VLDL by transfer from HDL • VLDL binds through apo C-II to lipoprotein lipase allowing triglycerides to be removed. This leaves a particle depleted of TG and apo C-II which is IDL

Intermediate Density Lipoprotein • They have apo B-100 and apo E on the particle surface. • IDL binds to liver LDL receptors through apo E and are then catabolized. • Some IDL particles have further TG removed by hepatic lipase producing LDL.

Low Density Lipoprotein • They are the main carrier of cholesterol and deliver it to liver and peripheral tissues. • They are taken by the liver by LDL receptors. • The number of LDL receptors regulates the circulating LDL concentration. • It is also regulated by the enzyme HMG-Co. A reductase activity.

LDL receptors in the liver cells • Each LDL contains a single apo B-100 which is the principle ligand for LDL clearance receptor. • LDL binds to receptors, internalized and taken up by endosomes • LDL receptors are formed in the endoplasmic reticulum and transported via the Golgi apparatus to the surface of hepatocyte

High Density Lipoprotein • HDL particles are produced in both liver and intestine. • HDL particle is capable of transporting cholesterol away from periphery to the liver and steroid-synthetic tissues (ovaries, testes, adrenal cortex) • HDL particles carry 20 -30% of the total quantity of cholesterol in the blood.

Lipids and Risk of Coronary Artery Disease • There is strong association between both total cholesterol and LDL and coronary artery disease. • HDL particles protect against atheroma. • There is a relatively weak link between VLDL and cardiovascular risk. • Excess chylomicrons do not confer a cardiovascular risk.

When to investigate for hyperlipidemia? • Family history of coronary heart disease (especially below 50 y of age) • Family history of lipid disorders • Xanthoma • Xanthelasma • Corneal arcus before the age of 40 y • Obesity, diabetes, hypertension

xanthelasma

Arcus Senilis

Hyperlipidemia Primary Secondary
 • Nephrotic syndrome •")
Causes of secondary hyperlipidemia • Hypothyroidism • Diabetes (poorly controled) • Nephrotic syndrome • Drugs: thiazide diuretics, corticosteroids, op. DDD.
 • Disorders of LDL (Hypercholesterolemia)")
Primary Hyperlipidemia • Disorders of VLDL and chylomicrons (Hypertriglyceridemia) • Disorders of LDL (Hypercholesterolemia) • Combined hyperlipidemia
 • It appears to be due to multiple")
Disorders of VLDL and chylomicrons (Hypertriglyceridemia) • It appears to be due to multiple genes to produce excess VLDL (polygenic hypertriglyceridaemia). • The only clinical feature is attacks of pancreatitis or retinal vein thrombosis.

Lipoprotein lipase deficiency and apoprotein C-II deficiency • There is persistence of chylomicrons in the circulation because the triglycerides within cannot gain access to lipoprotein lipase due to deficient apo C-II or due to defective enzyme

Clinical Picture • Patients present in childhood with: • Eruptive xanthomas • Lipaemia retinalis • Retinal vein thrombosis • Pancreatitis • hepatospleenomegaly

Lipaemia Retinalis • Retinal vessels appear white due to milky chylomicron rich plasma.

Management • Weight reduction and correction of other cardiovascular risk factors. • Lipid lowering diet. • Fibric acid drevative (gemfibrozil). • Fish oil capsules which contain omega 3 long-chain fatty acids.
 • Autosomal dominant monogenic disorder. • Patients may have no")
Disorders of LDL (Hypercholesterolemia) • Autosomal dominant monogenic disorder. • Patients may have no physical signs. • The diagnosis is made on laboratory basis. • Typical family history of early cardiovascular diease. • The genetic defect is underproduction or malproduction of LDL receptors in the liver.
 Homozygous familial hypercholesterolaemia Mutation of apo B-100 gene Polygenic hypercholesterolaemia")
Disorders of LDL (Hypercholesterolemia) Homozygous familial hypercholesterolaemia Mutation of apo B-100 gene Polygenic hypercholesterolaemia

Homozygous familial hypercholesterolaemia • Very rare disease, the affected children have no LDL receptors in the liver • The natural history is death from IHD in late childhood or adolescence. • Treatment: repeated plasmapheresis, liver transplantation, possibility of gene therapy in the future.




Mutation of apo B-100 gene • Relatively common single gene disorder. • LDL particles bind to their clearance receptors in the liver through apo B-100 • It has the same clinical picture of homozygous familial hypercholesterolemia

Polygenic hypercholesterolaemia • This term is used to lump together patients with raised serum cholesterol without one of the monogenic disorders mentioned before.

Management • Stop smoking • Treatment of hypertension • Reduction of excessive alcohol consumption and weight • Perimenopausal women should receive HRT • HMG-Co. A reductase inhibitors

Combined hyperlipidemia • Familial combined hyperlipidemia is relatively common, with typical family history, with no typical physical signs • Remnant hyperlipidemia is rare and is due to accumulation of LDL remnant particles with extremely high risk of cardiovascular disease. It is characterized by xanthomas in the palmar creases (diagnostic), and tuberose xanthomas over knees and elbows.

Tuberose xanthoma

Tuberous xanthomata and lipid deposits in the hand creases in a patient with remnant hyperlipidaemia

Management • The concurrent use of fibrate and statin is usually avoided due to overlaping side effects. • Combination of fibric acid derivative and bile acid binding resin if fibrate alone is insufficient.

The lipid lowering diet • Reduce the total fat intake • Substitution with monounsaturated and polyunsaturated fat. • Reduce the dietary cholesterol intake • Increase the intake of fiber • Achieve an ideal body weight
 • Bile acid binding resins (cholestyramine)")
Lipid Lowering Drugs • Fibrates (gemfibrosil, bezafibrate, fenofibrate) • Bile acid binding resins (cholestyramine) • HMG-Co. A reductase inhibitors (statins): Simvastatin, pravastatin, atorvastatin, fluvastatin. • Nicotinic acid • omega 3 long-chain fatty acids (for hypertriglyceridaemia)

Fibrates • Contraindications: severe hepatic or renal impairment, gall bladder disease, pregnancy • Adverse effects: reversible myositis, nausea, gallstones, malaise, impotance.

Statins • Contraindications: active liver disease, pregnancy, lactation. • Adverse effects: derangement of liver function tests, myositis.

- Slides: 42