Disorders of Hemostasis Sultana Qureshi PGY2 Resident Rounds






 – I, II, V,")





 • Trauma (eg, polytrauma, neurotrauma, fat")

 n Neuro n n Skin")
 n")















 n Mgmt: DDAVP 0.")












 Intra-articular bleeding")

 More likely")
")

 Long PTT n B)")




- Slides: 57
Disorders of Hemostasis Sultana Qureshi, PGY-2 Resident Rounds March 1, 2007 Thanks to Adam Oster for some slides!
Goals Approach and when to be suspicious n Pattern of presentation n ED Management – when to use blood products n
Hemostasis Endothelial cells n Platelets n Blood flow & vasoconstrictors n Clotting cascade n Fibrinolysis n
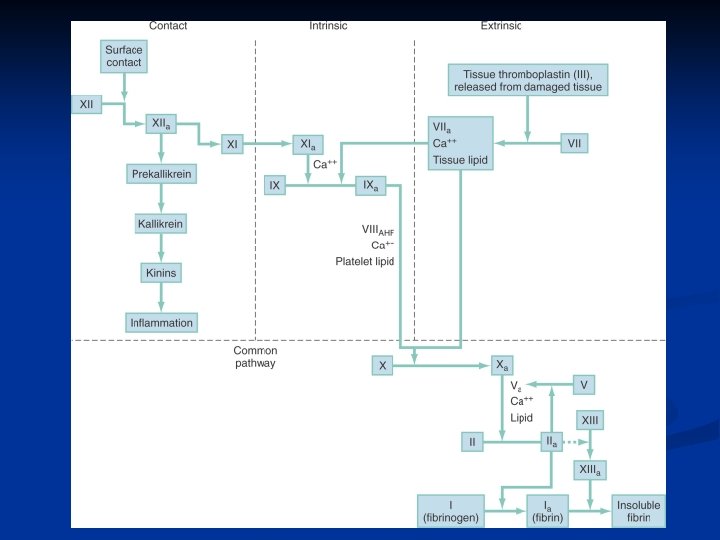
Approach to Bleeding Disorders n Primary Hemostasis n n Exposed endothelial cells cause platelets to aggregate and form plug Platelet Disorders n n n ITP TTP Also partially in liver disease, v. WD n Secondary Hemostasis n n n Tissue factor iniates coagulation cascade eventually leading to fibrinogen forming fibrin cross links Extrinsic starts pathway, intrinsic sustains Coagulation Disorders n n n v. WD Hemophilia A & B Other – consumptive (DIC)
When to be suspicious n n n n n Petechiae, Purpura, Ecchymosis Nature of bleeding/sites Significant or multiple episodes Signs of previous bleeding Medications (anti-coagulants) Associated disease: liver disease, sepsis Massive transfusion FHx Other important historical/physical info to know? ? ?
Approach to Bleeding Disorders n Platelet Disorder n n Immediate onset Superficial bleeding n n n Petechiae/Ecchymoses (mucocutaneous) GI/GU bleeding Menorrhagia, epistaxis, melena Plt or Bleeding Time abn PT/PTT N n n n Coagulation Factor Disorder Delayed onset (hours/days) Deep bleeding n n n n Intramuscular Intraarticular Retroperitoneal Hematuria Hemarthrosis/hematomas Less common to have menorrhagia, epistaxis, etc Plt and BT N PT/PTT abn
Labs n n n n n CBC, plts PTT (intrinsic) – I, II, V, VII, IX, X, XII INR (extrinsic)– I , II, V, VII, X Peripheral smear Fibrinogen D-dimer FDP Factor levels Thrombin time
What and how do you measure bleeding time? n When is it useful? n
Blood Products Platelets – 1 unit raise value by 5 -10 n Cryoprecipitate – FVIII, v. WF, fibrinogen, fibronectin n FFP – contains all coagulation factors (about 7% of a 70 kg person) n
Case 25 F – 32 wks GA presents with decr. LOC n Husband states had intermittent abdo pain X 2 days, suddenly got worse today n Vitals: 120, 90/50, 18, 99% 2 L NP, 36. 5 n Doppler – fetal bradycardia n Uterus is tender and tense n
DIC - Causes • Sepsis/severe infection (any microorganism) • Trauma (eg, polytrauma, neurotrauma, fat embolism) • Organ destruction (eg, severe pancreatitis) • Malignancy –solid tumors –myeloproliferative/ lymphoproliferative • Vascular abnormalities –Kasabach-Merritt Syndrome –large vascular aneurysms • Severe hepatic failure • Severe toxic or immunologic reactions –snake bites –recreational drugs –transfusion reactions –transplant rejection n • Obstetrical calamities –amniotic fluid embolism –abruptio placentae n Hypothermia Acidosis
Pathophysiology n n Unifying cause relates to widespread endothelial damage with extensive cytokine release DIC is a spectrum, may have thrombosis or bleeding or both n Activation of procoagulant pathway n n Endothelial damage n n Liver disease, splenectomy Vascular stasis n n Sepsis, vasculitis, aneurysm, hemangioma Reticuloendothelial injury n n Hemolysis, tissue injury, malignancy, fat embolism, heat stroke Hypotension, hypovolemia, PE Other n Acute hypoxia/acidosis
Clinical Features n Signs of Microvascular Thrombosis (10 -40%) n Neuro n n Skin n n ARDS GI n n Oliguria, azotemia, cortical necrosis Pulmonary n n Focal ischemia, superficial gangrene Renal n n Multifocal, delirium, coma, seizures Acute ulceration RBC n Microangiopathic hemolysis n Signs of hemorrhagic diasthesis (more common) n Neuro n n Skin n n Petechiae, echymosis, oozing Renal n n IC bleed hematuria Mucosal n Gingival oozing, epistaxis, massive bleed
Labs n Consumptive Coagulopathy ↓Plts n ↑PT, ↑PTT n ↓Fibrinogen (careful in sepsis) n +D-dimer (DIC) n
DIC Scoring System Bakhtiari K et al. Critical Care Med. 2004; 32: 2416 -2421. n Step 1. Risk assessment: does the patient have an underlying disorder known to be associated with overt DIC? If yes, proceed. If no, do not use this algorithm. Step 2. Order global coagulation tests: platelet count, prothrombin time (PT), fibrinogen, soluble fibrin monomers, or fibrin degradation products. n Step 3. Score global coagulation test results: • platelet count (> 100 = 0, < 100 = 1, < 50 = 2) • elevated fibrin-related marker (eg, soluble fibrin monomers/fibrin degradation products) no increase: 0; moderate increase: 2; strong increase: 3* • prolonged prothrombin time (< 3 sec. = 0, > 3 but < 6 sec = 1, > 6 sec = 2) • fibrinogen level (> 1. 0 g/L = 0, < 1. 0 g/L = 1) Step 4. Calculate score. Step 5. If ≥ 5: compatible with overt DIC; repeat scoring daily. If <5: suggestive (not affirmative) for non-overt DIC; repeat next 1– 2 days. n * In the prospective validation studies, D-dimer assays were used and a value above the upper limit of normal was considered moderately elevated; whereas, a value above five times the upper limit of normal was considered a strong increase.
DIC Scoring System Bakhtiari K et al. Critical Care Med. 2004; 32: 2416 -2421. n n Sens 93% Spec 96%
Management n n n TREAT UNDERLYING CAUSE!!! Blood Products Only if active bleeding or high risk of bleeding (ie. early post op or pre-invasive procedure) n Platelets n n Bleeding – tranfuse if count <50 No bleeding – transfuse if <10 -20 FFP Cryoprecipitate n n If fibrinogen <2 1 -4 U/10 kg
Novel treatments APC – up to Phase III trials show benefit in septic DIC n TFPI – promising n ATIII- RCT promising n Heparin n Only case series. Controversial n Therapeutically if overt venous TE or purpura fulminans n
Case n n n n n 22 M presents with seizures, decr. LOC, jaundice and fever Purpuric rash over body V: 60, 110/70, 16, 96% RA, T=38. 3 Hb 90, WBC 8. 0, plt 20 PT/PTT N Cr 130, small hematuria T. bili 60 other LFTs N, LDH 500 Ddx? D-dimer/fibrinogen?
TTP n Main ED mgmt point: n NO platelet transfusion unless life threatening hemorrhage
Liver Disease What mechanisms of coagulopathy? n What blood products to use? n
Liver Disease n Why they bleed? n n n n Thrombocytopenia from hypersplenism (portal HTN) Platelet dysfunction Reduction in absorption of Vit K dependant factors (2, 7, 9, 10) Reduction in synthesis of most factors Dysfibrinogenemia (abn fibrinogen synthesis) Enhanced fibrinolysis (decr. Plasmin inhibitor) In bleeding ER – may require transfusion of many different products (RBC, plts, FFP, cryo) Vs. DIC? ? ?
Case n n n n 6 F with epistaxis (has had multiple mild episodes in past 2 d) Also history of spitting up blood in morning Examine mouth and see blood oozing from gums when scraped with tongue depressor Otherwise well other than flu 3 weeks ago Notice petechiae around sock elastic Dx? Lab results?
Acute ITP n n n n Usually children 2 -6 M=F Usually have had recent infection Abrupt onset of bleeding (vs insidious) Platelets <20 Usually lasts week 80% spontaneous remission Management: IVIG if bleeding significant of plts <10 -splenectomy in very severe cases
Chronic ITP n n n n n MCC of isolated thrombocytopenia Adults (20 -40 yo), F>M (3: 1) No precipitating infection Insidious bleeding (heavy periods, easy bruising) Plt 30 -80 May last months to years, and uncommon spont. Remission Mgmt: steroids, IVIG, splenectomy Need w/u for other causes of thrombocytopenia! Esp if older (ie malignancy)- Smear Major concern is cerebral hemorrhage is plt<5
Platelet Disorders Quantitative Destruction Immune Non-immune ITP TTP DIC HELLP Sepsis Decreased Production Qualitative Sequestration splenomegaly Marrow failure ASA, plavix rena and hepatic disease, v. WD
Case 12 F hx of VWD n Presents with heavy menarche (ongoing bleeding for >7 days) n Pale, asymptomatic n Hb = 60 n Mgmt? n
Erik Adolf von Willebrand n n 1870 -1949 Finnish Pediatrician “known for integrity and modesty” Hjordis – 5 yo girl with FHx of bleeding disorders
Von Willebrand’s Disease n n AD Qualitative vs. quantitative abn Different sized multimers v. WF has 2 jobs n n Platelet adhesion, carrier for Factor VIII New Classification n Type 1: mild quantitative defect (75%) Type 2: qualitative defect (impaired fxn)20% Type 3: severe total quantitative defect (rare)
Management n Type 1 Usually mild symptoms (mucocutaneous bleeding sources) n Mgmt: DDAVP 0. 2 mcg/kg IV/IM/IN n n Type 2 or 3 More likely to have mod-severe symptoms incl. soft tissue hematomas, GI bleeds, hemarthroses n Mgmt: Cryoprecipitate +/- DDAVP +/- Humate P n
Case 50 M slipped on ice and twisted R knee n On exam: large hemarthrosis n What is most likely hemostatic disorder? n Management? n
Hemophilia A – FVIII deficiency n B – FIX deficiency n X-linked recessive n Mild/mod/severe is based on factor activity n n 5 -30%, 1 -5%, <1% PTT prolonged (if factor activity <30%) PT N n However, if mild hemophilia, PTT may be N n
Bleeding first noticed usually in early years n 5 Hs: n Hemarthroses n Hematomas n Hematochezia n Hematuria n Head hemmorhage n
n n Recurrent hemarthroses lead to joint damage IC bleed is major cause of death Also, tend to bleed LATE – days after minor injury Therefore treat aggressively n n Goal to achieve 30 -100% factor activity Options: Specific factor replacement, cryo, FFP Consider: Severity of bleeding, disease severity and availability of products Always consider factor activity is zero in ED!!!
Factor Replacement Is ideal if available in ED, otherwise cryo n 1 U/kg will increase factor by 2% n May develop alloantibodies and need 3 -4 X predicted dose n Goals: n Mild: 5 -10% activity desired -initial dose 12. 5 U/kg n Mod 20 -30% - 25 U/kg n Severe >50% - 50 U/kg n
Cryoprecipitate n Contains 80 - 100 U FVIII (als contains v. WF, fibrinogen, FXIII and fibronectin) Considered a second line agent for Hem A n Dose = 2 bags/10 kg to raise FVIII to hemostatic levels n T ½ = 8 hrs n
FFP Fluid portion of blood separated at 18 C then frozen n Contains all coagulation factors n n n Approx 7% of of all coag factor activity of a 70 kg person Not routinely used as factor replacement in Hem A n Could consider if nothing else available
Case 25 M hemophiliac n Tripped on stairs and fell from 1 ft height n Hit head on floor. No LOC, NV. Feels fine n Management? n
Mgmt All hemophiliacs with any trauma need admission for observation n Minor head trauma can be life threatening n n Give Factor VIII to 50% activity BEFORE CT
Take Home Points n Approach to bleeding disorders n High index of suspicion n Difference in presentation of platelet dysfunction vs. coagulation factor d/o n When to give blood products?
Take Home Points n DIC – treat underlying cause n v. WF – important to know type n Hemophilia – aggressive therapy with factors
Quiz n Which of the following is least likely due to a platelet disorder? A) Epistaxis n B) Retroperitoneal Bleeding n C) Ecchymoses n D) Petechiae n
Quiz n Which is least likely associated with coagulation factor deficiency? A) Intra-articular bleeding n B) Delayed bleeding n C) Retroperitoneal Bleeding n D) Petechiae n
Quiz n Which clinical finding is MOST COMMONLY associated with the onset of ITP? A) Ecchymoses n B) Purpura n C) Petechiae n D) Gingival bleeding n
Quiz n Which of the following are true of chronic ITP? A) More likely in female children n B) Spontaneous remission typical n C) Underlying disorder is autoimmune n D) Platelet transfusion is initial, definitive therapy n
Quiz n Which lab finding is more indicative of liver disease vs DIC? A) Thrombocytopenia with bleeding n B) Prolonged PT n C) Decreased fibrinogen n D) Normal or min. elevated D-dimer n
Quiz n n n 50 M cirrhotic with ascites presents with SBP. HD stable and no active bleeding Prolonged PTT, INR Low platelets and fibrinogen What to give prior to paracentesis? n n A) Cryo B)FFP C)Platelets D)DDAVP
Quiz n Most commonly observed lab abnormality in DIC? A) Long PTT n B) Thrombocytopenia n C) Low fibrinogen n D) elevated D-dimer n
Quiz n What is the most appropriate analgesic for a patient with Type 1 v. WD? 1) ASA 80 n 2) ASA 325 n 3) Ibuprofen n 4) Acetaminophen n 5) Naprosyn n
Quiz 9 M with Type 1 v. WD presents with mild gingival bleeding after flossing. n Stable, however slow bleeding has continued for hours despite local pressure n Most appropriate treatment? n
Quiz 19 M restrained back seat passenger, rear ended at 35 kph. Hit head on front seatback. No LOC. No neck pain. Ambulatory on scene. n Exam normal except small contusion to forehead. n History of Hemophilia B n Mgmt? n
Quiz n n n 7 M presents with LLQ pain after being “knee’ed” by a bully at school 2 hours ago History of Hemophilia A “severe” VSS, contusion in L inguinal area, mildly tender Pain with extension of lower extremity, and walks flexed at the torso with a limp Next step? n n A) Give Factor VIII and CT Abdo B) Give Factor IX and CT Abdo C) Give DDAVP and CT D) Give FFP and US Abdo