Disorders of hair Less hair Excessive hair The

 The bulb A swelling")
 The medulla An area in the core which contains loose")























 therapy may help in")

 Cause It is because of miniaturization of hair follicles Although")





, an inhibitor of human type II 5α-reductase, reduces serum and scalp")






 Hairy pinna (Congenital hairs")









- Slides: 61
Disorders of hair Less hair Excessive hair
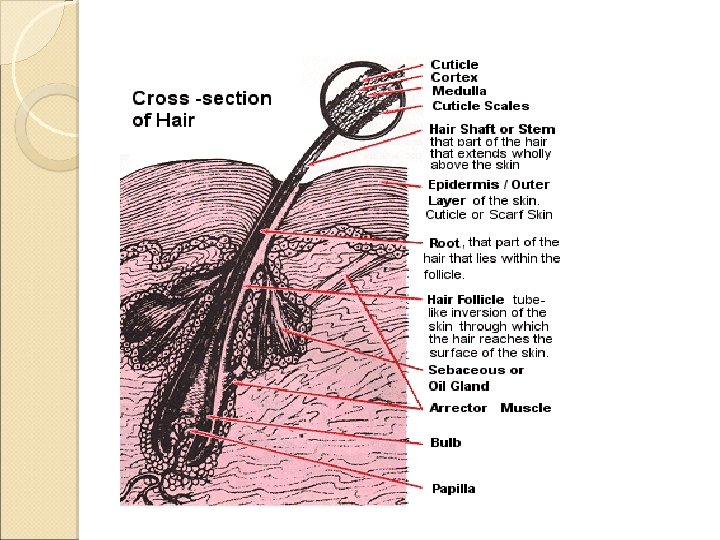
The hair can be divided into three parts (1) The bulb A swelling at the base which originates from the dermis (2) The root The hair lying beneath the skin surface (3) The shaft Which lies above the skin surface.
In cross-section, (1) The medulla An area in the core which contains loose cells and airspaces (2) The cortex Which contains densely packed keratin and (3) The cuticle Which is a single layer of cells arranged like roof shingles.
Classification Hairs are classified into three main types ◦ Lanugo hair ◦ Vellus hair ◦ Terminal hairs convert to vellus hairs in male pattern alopecia Vellus hairs convert to terminal hairs in hirsutism.
Lanugo hair Fine long hair covering the foetus Shed about 1 month before birth unless born prematurely. May reappear sometimes in severe malnutrition and anorexia nervosa.
Vellus hair Fine, short unmedullated hair covering much of the body surface. They replace the lanugo hair just before birth.
Terminal hair Fully developed Long coarse medullated hair in the scalp or pubic regions. Their growth is influenced by circulating androgen levels.
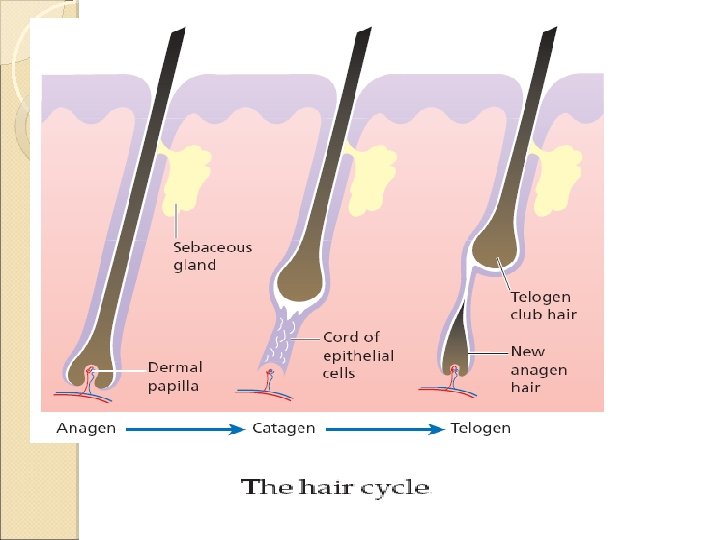
The hair cycle Each follicle passes through regular cycles of growth and shedding. There are three phases of follicular activity ◦ Anagen The active phase of hair production. ◦ Catagen A short phase of conversion from active growth to the resting phase. Growth stops, and the end of the hair becomes club-shaped. ◦ Telogen A resting phase at the end of which the club hair is shed.
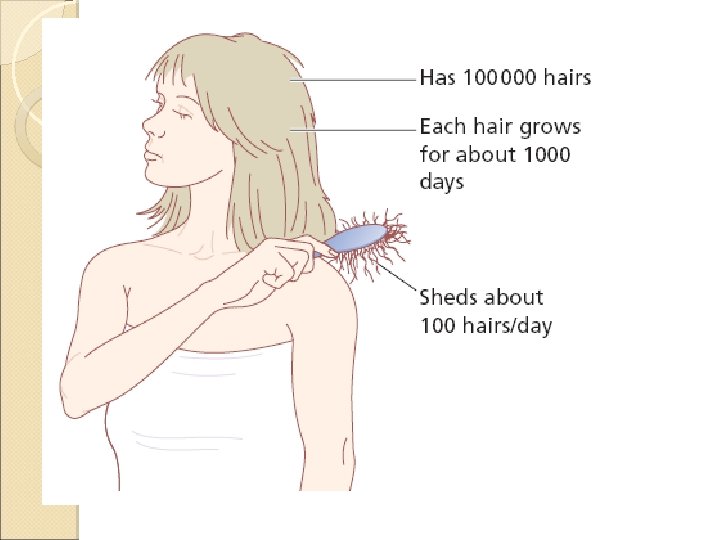
The duration of each of these stages varies from region to region. On the scalp it is said to contain an average of 100, 000 hairs ◦ Anagen lasts for upto 5 years ◦ Catagen for about 2 weeks ◦ Telogen for about 3 months As many as 100 hairs may be shed from the normal scalp every day as a normal consequence of cycling.
Alopecia The term alopecia means loss of hair Alopecia has many causes and patterns. One convenient division is into ◦ Localized ◦ Diffused It is also important to decide if the hair follicles are replaced by scar tissue; if they have, regrowth cannot occur.
CLASSIFICATION OF ALOPECIA Localised Non-scarring Tinea capitis Alopecia areata Androgenetic alopecia Traumatic (trichotillomania, traction, cosmetic) Syphilis Scarring Idiopathic Developmental defects Discoid lupus erythematosus Herpes zoster Pseudopelade Tinea capitis/kerion Diffuse Androgenetic alopecia Telogen effluvium Metabolic Hypothyroidism Hyperthyroidism Hypopituitarism Diabetes mellitus HIV disease Nutritional deficiency Liver disease Post-partum Alopecia areata Syphilis Discoid lupus erythematosus Radiotherapy Folliculitis decalvans Lichen planus pilaris
Localized alopecia Alopecia areata
Etiology An immunological basis is suspected because of an association with ◦ ◦ Autoimmune thyroid disease Pernicious anemia Vitiligo Atopy Histologically, T lymphocytes cluster like a swarm of bees around affected hair bulbs because cytokines produced by the dermal papillae in lesions not only attract lymphocytes to perifollicular region but also stimulate them to multiply
Alopecia areata is probably inherited as a complex genetic trait Sometimes HLA-DQ 3, -DR 11 or -DR 4 act as susceptibility factors ◦ With an increased occurrence in the first-degree relatives of affected subjects and twin concordance. It affects some 10% of patients with Down’s syndrome, suggesting the involvement of genes on chromosome 21. Environmental factors as well as emotional factors may trigger alopecia areata in the genetically predisposed.
Epidemiology AA is the common type Both gender affected Can start at any age
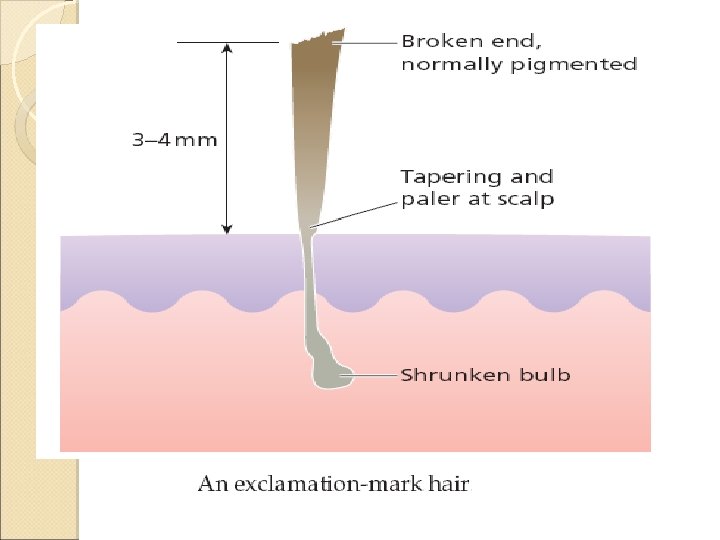
Presentation A typical patch of hair loss area is uninflamed, with no scaling, but with empty hair follicles Pathognomonic ‘exclamation-mark’ hairs may be seen around the edge of enlarging areas. They scalp Are are broken off about 4 mm from the narrowed and less pigmented proximally
Incidence is most common in the scalp and beard but other areas, especially the eyelashes and eyebrows, can be affected too. An uncommon diffuse pattern is recognized, with exclamation-mark hairs scattered widely over a diffusely thinned scalp. Up to 50% of patients show fine pitting or wrinkling of the nails.
The characteristic uninflamed patches of alopecia areata.
Exclamation-mark hairs: Pathognomonic of alopecia areata.
Course The outcome is unpredictable. In a first attack, regrowth is usual within a few months. New hairs appear in the centre of patches as fine pale down, and gradually regain their normal colour The new hair may remain white in older patients. Fifty percent of cases resolve spontaneously without treatment within 1 year Only 10% have severe chronic disease Subsequent episodes tend to be more extensive Regrowth is slower.
Hair loss in some areas may coexist with regrowth in others. A few of those who go on to have chronic disease loose all the hair from their heads (alopecia totalis) or from the whole skin surface (alopecia universalis). other variant is ophiasis which is lose of hair in a band like patternat the periphery of scalp Regrowth is tiresomely erratic but the following suggest a poor prognosis: type) 1. Onset before puberty 2. Association with Atopy or Down’s syndrome 3. Unusually widespread alopecia and 4. Involvement of the scalp margin (ophiasiform
Alopecia totalis Alopecia universalis
Differential diagnosis Ringworm infection Lupus erythematosus Lichen planus Hair-pulling habit of children Traction alopecia Secondary Pseudopelade
Investigations None are usually needed. The histology of bald skin shows lymphocytes around and in the hair matrix. Syphilis can be excluded with serological tests Organ-specific autoantibody screens
Treatment A patient with a first or minor attack can be reassured about the prospects for regrowth. Topical corticosteroid creams of high potency can be prescribed The use of systemic steroids should be avoided in most cases Intradermal injection of 0. 2 ml intralesional triamcinolone acetonide (5– 10 mg/ml), raising a small bleb within an affected patch, leads to localized tufts of regrowth. Side effects dermal atrophy evident as depressed areas at the sites of injections.
Regrowth within a patch of alopecia areata after a triamcinolone injection.
Ultraviolet radiation or even psoralen with ultraviolet A (PUVA) therapy may help in extensive cases, but hair fall often returns when treatment is stopped. Contact sensitizers (e. g. diphencyprone) seemed promising but the long-term effect of persistent antigen stimulation is worrying; they are still being used only in a few centres under trial conditions. Wigs are necessary for extensive
A trial of diphencyprone to one side of the scalp caused some regrowth
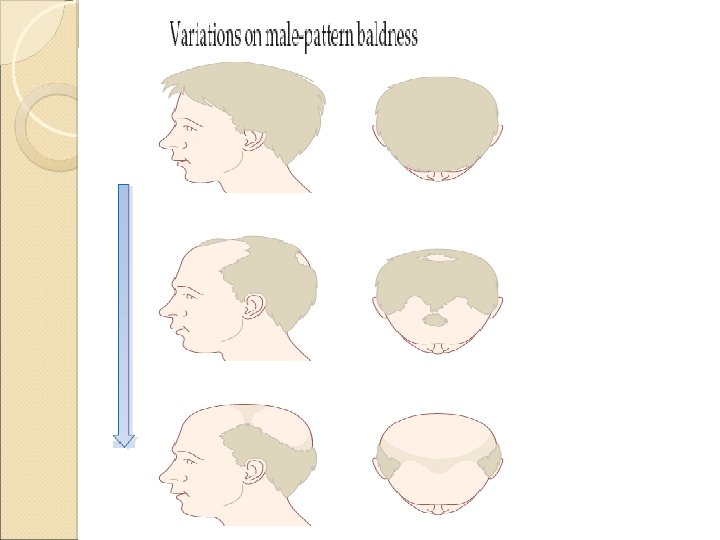
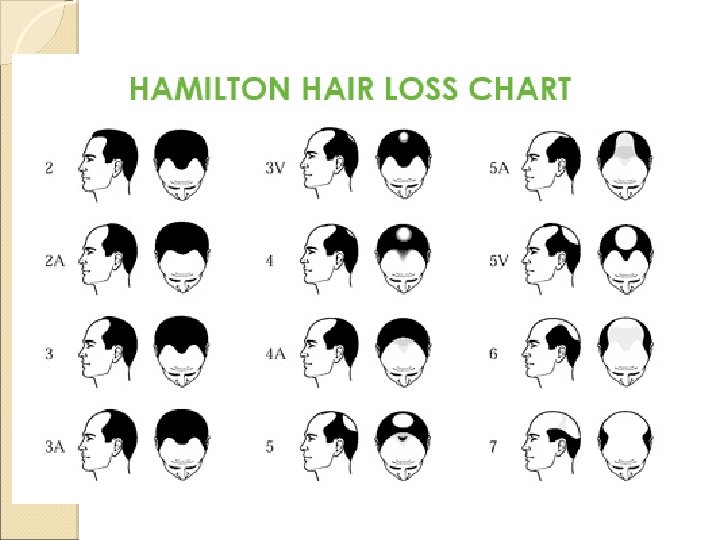
Androgenetic alopecia (malepattern baldness) Cause It is because of miniaturization of hair follicles Although clearly familial, the exact mode of inheritance has not yet been clarified. Male-pattern In baldness is androgen dependent females, androgenetic alopecia (femalepattern hair loss), with circulating levels of androgen within normal limits, is seen only in those who are strongly predisposed genetically.
Presentation The common pattern in men is the loss of hair first from the temples, and then from the crown However, in women the hair loss may be much more diffuse, particularly over the crown In bald areas, terminal hairs are replaced by finer vellus ones.
Androgenetic alopecia beginning in the frontal area
Complications Anxiety Bald scalps burn easily in the sun It has been suggested recently that bald men are more likely to have a heart attack and prostate cancer than those with a full head of hair
Differential diagnosis The diagnosis is usually obvious in men, but other causes of diffuse hair loss have to be considered in women
Treatment Scalp surgery Hair transplants Wigs Topical application of minoxidil lotion may slow early hair loss and even stimulate new growth of hair but the results are not dramatic ◦ Small and recently acquired patches respond best. ◦ When minoxidil treatment stops, the new hairs fall out after about 3 months. Antiandrogens help some women with the diffuse type of androgenetic alopecia.
Treatment Finasteride (Propecia), an inhibitor of human type II 5α-reductase, reduces serum and scalp skin levels of dihydrotestosterone in balding men and at the dosage of 1 mg/day, it may increase hair counts ◦ Lead to a noticeable improvement in both frontal and vertex hair thinning. ◦ However, the beneficial effects slowly reverse once treatment has stopped. ◦ This treatment is not indicated in women or children. Side-effects are rare, but include ◦ Decreased libido, erectile dysfunction and altered prostate-specific antigen levels
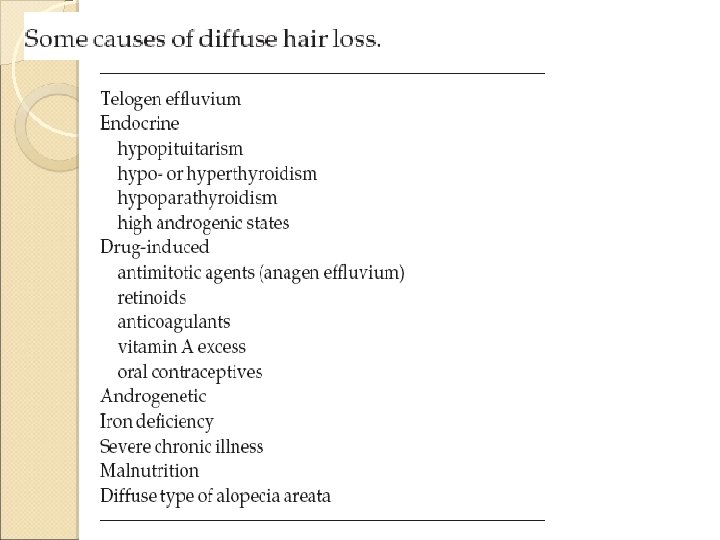
Telogen effluvium All the hair follicle are not synchronous in their cycle If anagen phase of several adjoining hair follicles is aborted and these follicles enter telogen phase at the same time and several hair are shed simultaneously this is called telogen effluvium
Etiology: Infections: typhoid, malaria, dengue Childbirth: prolonged Surgical trauma Haemorrhage Emotional stress
Clinical features: hair loss occurs after 2 -3 mths after the precipitating factor Severe cases associated with anemia and beau’s lines of the nails. Treatment: stops spontaneously after 2 -3 mths
Excessive hair Hypertrichosis Hirsutism
Hirsutism and hypertrichosis Hirsutism is the growth of terminal hair in a woman which is distributed in a pattern normally seen in a man (for example, mustache, beard, central chest, shoulders, lower abdomen, back, and inner thighs). Hypertrichosis is an excessive growth of terminal hair in either sex that does not follow an androgen-induced pattern
Types of hypertrichosis Congenital Hypertrichosis is very rare. ◦ A fetus is covered with lanugo and it does not fall off but continues to grow. Acquired Hypertrichosis ◦ Occurs after birth. ◦ Unpigmented vellus hair or pigmented terminal hair. ◦ The excessive hair may cover the entire body (Generalized), or it could be localized to one area.
Congenital Localized forms: Hypertrichosis cubiti (Congenital hairs on elbows) Hairy pinna (Congenital hairs on the external ears)
Acquired hypertrichosis
Causes of hypertrichosis Localized ◦ ◦ ◦ Melanocytic naevi Becker’s naevi Satyr’s tuft in sacral area- in patients with spina bifida Chronically inflamed joints Under plaster casts Carrying weights over shoulder
Causes of hypertrichosis Generalized Anorexia nervosa, starving, malnutrition Drug induced- minoxidil, diazoxide, ciclosporin anabolic steroids. porphyrias Fetal alcohol syndrome Fetal phenytoin syndrome Hypertrichosis lanuginosa(congenital or acpuired) General systemic illness (such as advanced HIV infection) Hypothyroidism or other endocrine disorders
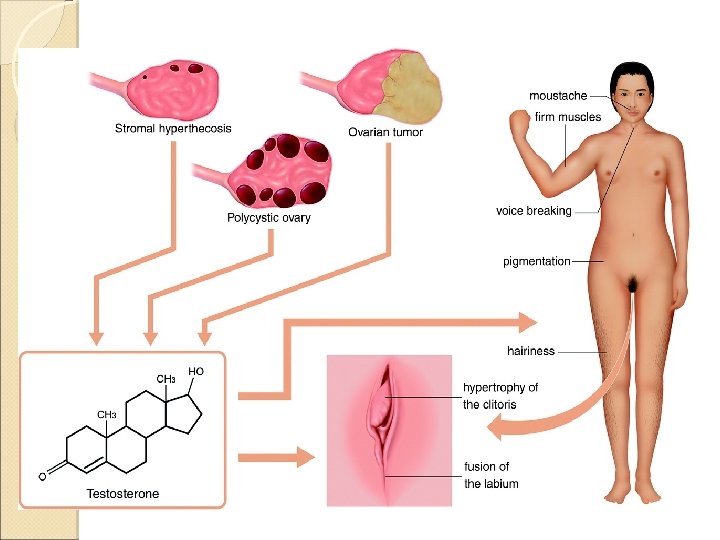
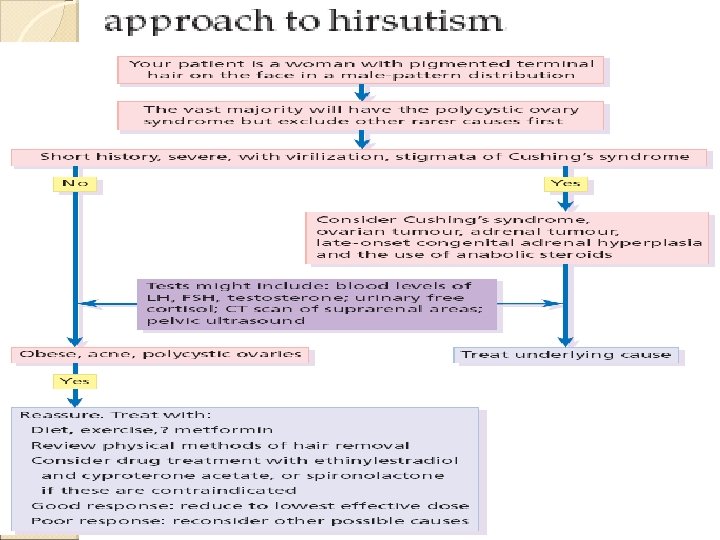
Hirsutism Cause Increased level of androgens or an oversensitivity of hair follicles to androgens Racial or familial trait (Mediterranean, Caucasians and Asians) Idiopathic hirsutism Hormonal: Polycystic Ovarian Syndrome Cushing's disease Tumors in the ovaries or adrenal gland Congenital adrenal hyperplasia postmenopausal women Itragenic: Drugs- androgens or progesterones, anabolic steroids.
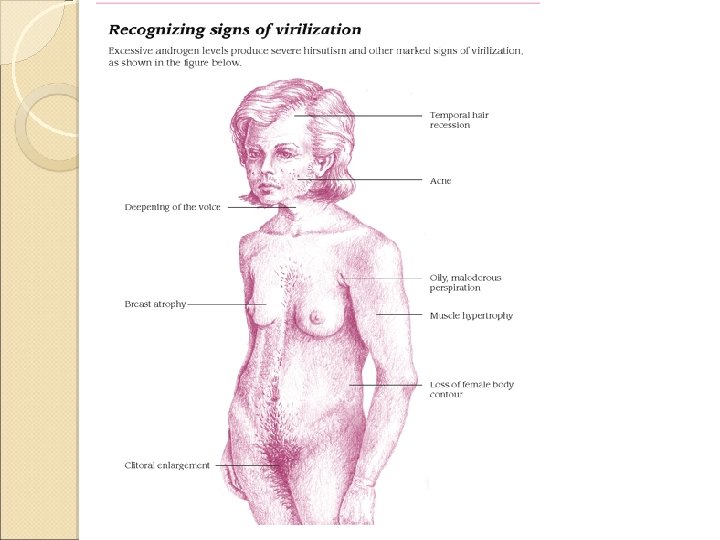
Presentation An excessive growth of hair in ◦ ◦ ◦ ◦ Beard area and side burn Chest Shoulder-tips Around the nipples Abdomen Male pattern of pubic hair Androgenetic alopecia Signs ◦ ◦ ◦ ◦ of virilization Temporal hair recession Acne Deep voice, increased size of Adam's apple Oily perspiration Breast atrophy Muscle hypertrophy Loss of female body contour
Investigations Significant hormonal abnormalities are not usually found in patients with a normal menstrual cycle. Investigations ◦ ◦ are needed if: Hirsutism occurs in childhood There are features of virilization Hirsutism is of sudden or recent onset There is menstrual irregularity or cessation
The tests sent are Total and free testosterone Sex hormone binding globulin Free androgen index Dihydroxyepiandrosterone sulfate Androstenedione (drawn after 10 a. m. ) If there is also menstrual disorder, additional tests may be requested. ◦ Luteinizing hormone (LH) and follicle stimulating hormone (FSH) ◦ Oestradiol, 17 -hydroxy progesterone ◦ Prolactin Tests may be requested to evaluate other related aspects of health, for example: ◦ Thyroid function ◦ Cortisol or overnight dexamethasone test ◦ Glucose ◦ Lipids (cholesterol and triglyceride)
Treatment Treat underlying disorder Home remedies for minor hirsutism include commercial, waxing or shaving, or making its appearance less obvious by bleaching Plucking should be avoided as it can stimulate hair roots into Anagen. The abnormally active follicles can be destroyed by electrolysis. If numerous, by laser Topical therapy with eflornithine, an inhibitor of ornithine decarboxylase, can slow regrowth.
Oral antiandrogens ◦ Oral contraceptive pills with oestrogen and cyproterone- antiandrogenic activity ◦ Cyproterone acetate 50 -200 mg for 10 days each cycle ◦ Spironolactone 50 -200 mg daily can slowly reduce excessive hair growth-long term. Pregnancy must be avoided during such treatment as it carries the risk of feminizing a male fetus.