Disorders of cardiovascular system 2 Dr Zainab Sajid

Disorders of cardiovascular system: 2 Dr. Zainab Sajid Al-Shimmari

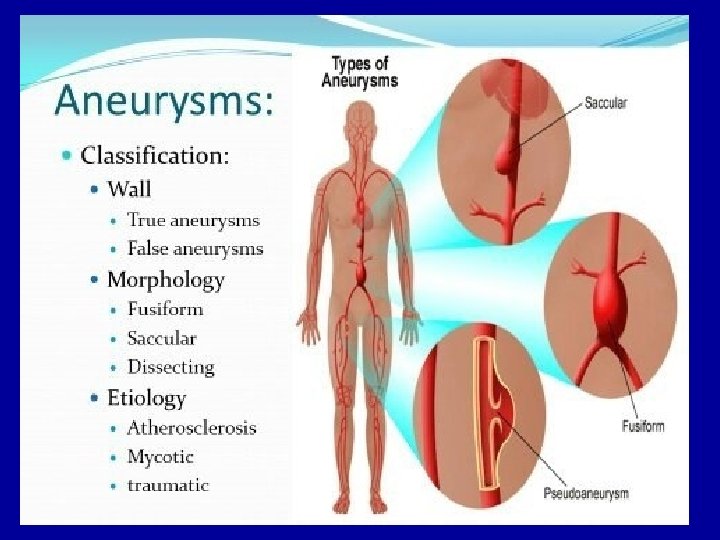
Aneurysm: 1 -An aneurysm is a localized, balloon-like swelling in the wall of an artery caused by weakening of the arterial wall. Aneurysm may occur in any artery, but the aorta is most susceptible (vulnerable ) to aneurysm due to the constantly high pressure on the walls of that vessel. Cerebral aneurysms may also occur. 2 - A leading cause of aneurysm is atherosclerosis, as the formation of lipid plaques can erode arterial walls and compromise their integrity.

3 -Aneurysms may also be associated with hypertension, vascular infections and the normal aging process. 4 Aneurysms that involve all three layers of the blood vessel wall are called true aneurysms to distinguish them from other types of arterial distention that may occur from external injury or trauma. 5 -A dissecting aneurysm is a very severe condition in which there is a tear in the inner layers of the blood vessel (tunica intima and tunica media) and as a result bleeding occurs in the space below the adventitia of the vessel.
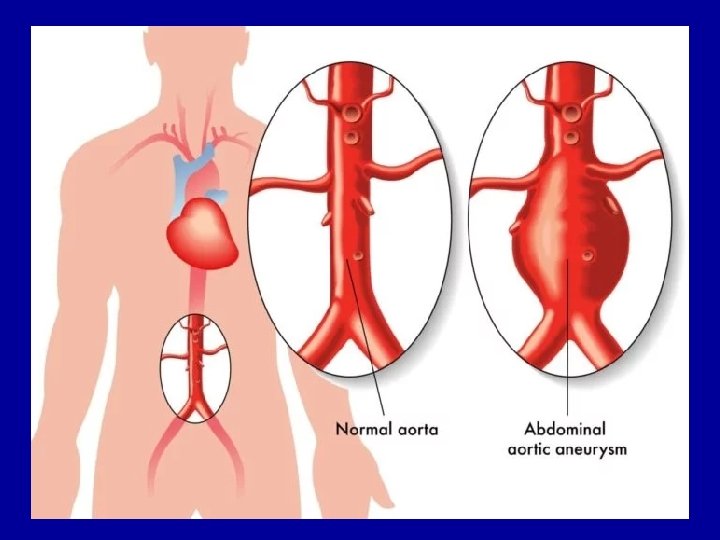

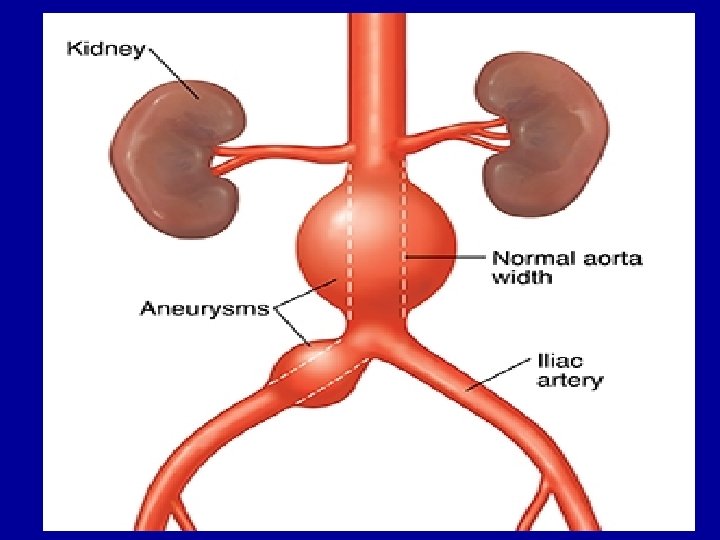
Here is an example of an atherosclerotic aneurysm of the aorta in which a large "bulge" appears just above the aortic bifurcation. Such aneurysms are prone to rupture when they reach about 6 to 7 cm in size. They may be felt on physical examination as a pulsatile mass in the abdomen. Most such aneurysms are conveniently located below the renal arteries
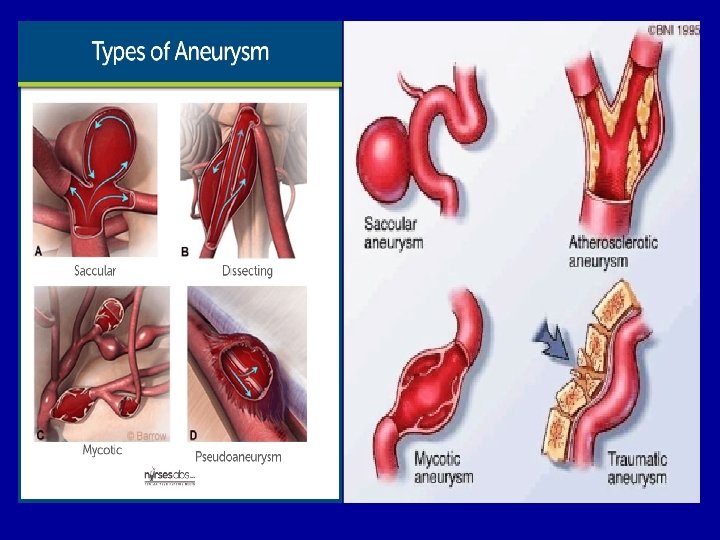
 aneurysms are the most common type.")
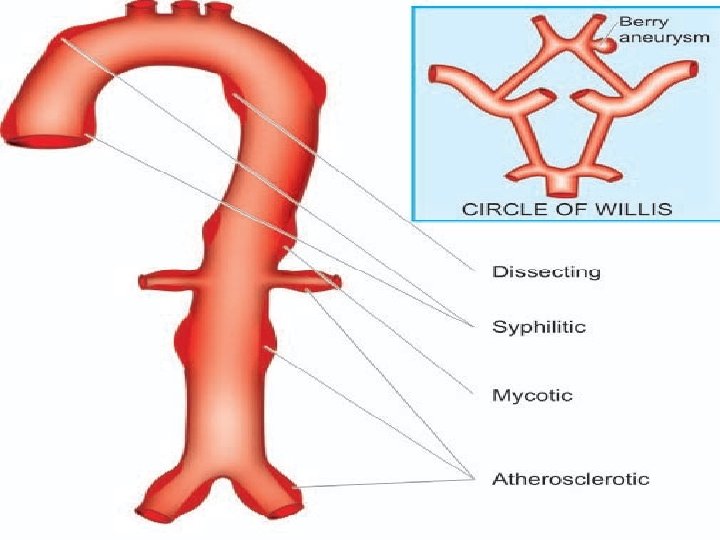
6 -Classification of aneurysms are: A. Atherosclerotic (arteriosclerotic) aneurysms are the most common type. B. Syphilitic (luetic) aneurysms found in the tertiary stage of the syphilis. C. Dissecting aneurysms (Dissecting haematoma) in which the blood enters the separated or dissected wall of the vessel. D. Mycotic aneurysms which result from weakening of the arterial wall by microbial infection. E. Berry aneurysms which are small dilatations especially affecting the circle of Willis in the base of the brain.

Clinical manifestations of aneurysm 1 • Depending upon size and location, aneurysms may be complelyet asymptomatic or may be associated with severe pain. 2 • Aneurysms in the thoracic aorta most commonly present with back or neck pain, cough, difficulty swallowing or compression of the trachea. 3 • Aneurysms in the abdominal aorta are often asymptomatic until they cause pain from compression on spinal nerves or abdominal organs. 4 • Aneurysms of the cerebral arteries often present with symptoms that are characteristic of increased intracranial pressure. Stroke can result if the abnormal blood vessel ruptures and bleeding occurs into the brain tissue.

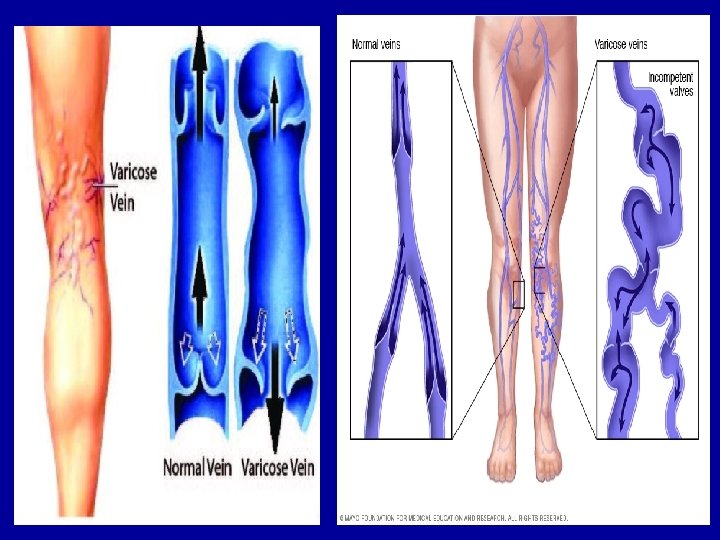
Varicose veins: 1 -Varicose veins are veins that have become distended over time due to the pooling of blood in the lower extremities. This condition occurs most frequently in individuals who spend long periods of time standing or who have impaired return of blood from the lower extremities.

2 -Veins are thin-walled vessels that are easily distended by the chronic pooling of blood in the lower extremities. Chronic distention of veins can reduce effectiveness of one-way venous valves that are present in the lumen to prevent the back flow of blood and lead to a condition termed valvularincompetence. 3 -These venous valves work in conjunction with skeletal muscle pumps in the legs to move blood back to the heart from the extremities. The most common manifestations of varicose veins are aching and edema.


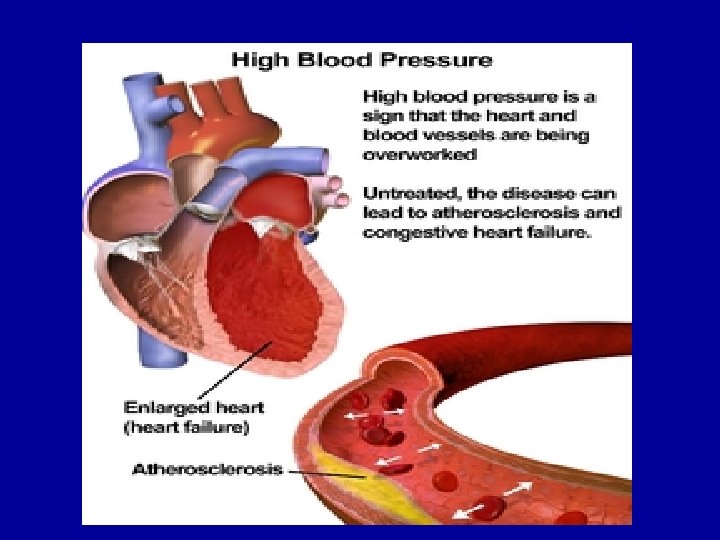
Hypertension: is defined as a consistent elevation of arterial pressure above the normal range expected for a particular age group. Approximately 90% of all hypertension cases are classified as primary hypertension. This form of hypertension is also called essential or idiopathic hypertension since its etiology is uncertain. Approximately 5 to 10% of patients are afflicted with secondary hypertension in which the cause of the elevated blood pressure is clearly defined.

I-Primary or essential hypertension: A-Although the cause of primary hypertension is still unknown, several theories involving chronic increases in fluid volume, enhanced sympathetic activity or abnormal salt and water excretion by the kidneys have been proposed to explain the mechanism of its occurrence. B-A number of key physiologic changes have also been observed in the kidneys of patients with essential hypertension that may contribute to the development of the disorder. These renal changes include increased resistance to renal blood flow, decreased renal blood flow with disease progression and inadequate excretion of fluid and electrolytes at normal blood pressures.

C-A number of genetic, environmental and dietary factors are associated with an increased risk for the development of essential hypertension: • Familial history of hypertension. • Increasing age. • Race and gender: incidence of hypertension is significantly higher in black men. • High dietary salt intake. • Hyperinsulinemia. • Heavy alcohol consumption. • Obesity. • Cigarette smoking. • Low dietary intake of potassium, calcium and magnesium.

Manifestations of essential hypertension: 1. Blood vessels: A- Prolonged high blood pressure in the arteries and arterioles will cause the walls of the blood vessels to thicken to compensate for the excess shear stress. B-The chronic increased shear forces that the blood vessel walls are exposed to also predispose them to atherosclerosis and aneurysm. As a result, untreated essential hypertension puts patients at a greater risk of coronary artery disease, cerebrovascular disease and renal vascular disease. C-The risk for atherosclerosis is exacerbated in hypertensive patients who have high serum cholesterol, are obese, have diabetes or who smoke.
 in addition to")
There are two other forms of arteriosclerosis (hardening of the arteries) in addition to atherosclerosis: arteriolosclerosis and medial calcific sclerosis. Arteriolosclerosis is typically seen in the kidneys. One form, called hyaline arteriolosclerosis, is demonstrated by the markedly thickened arteriole to the lower right of this glomerulus with PAS stain. Hyaline arteriolosclerosis is seen in the elderly.

2. Heart: A- Chronic elevation of arterial pressure means the heart must now pump blood out against a continually elevated after load. As compensation for this increased after load, left ventricular hypertrophy occurs. B-The hypertrophied ventricle will require increased blood, oxygen and nutrient supplies and will be at greater risk for arrhythmia. C-When the ventricular enlargement reaches a certain point, contractile function will no longer be supported and pump failure (congestive heart failure, CHF) will ensue.
, but the")
This left ventricle is very thickened (slightly over 2 cm in thickness), but the rest of the heart is not greatly enlarged. This is typical for hypertensive heart disease. The hypertension creates a greater pressure load on the heart to induce the hypertrophy.

3. Kidneys: A- Chronically elevated pressure can damage the renal vasculature and compromise renal blood flow, oxygen delivery and filtration. As a result, renal insufficiency can occur that may eventually progress to renal failure. B- Decreased renal blood flow can lead to activation of the renin–angiotensin system and contribute to avicious cycle of increasing blood pressure and decreasing renal function. C-Hypertension-induced renal injury is exacerbated in patients with diabetes.

4. Eyes: — Vision can suffer in a patient with chronic hypertension as a result of increased arteriolar pressure in the eyeball or from vascular sclerosis, both of which can damage the retina and eye as a whole.
")
Here is the normal funduscopic appearance of the retina. Note the arteries (brighter red) emanating from the central optic disk. The larger caliber and darker retinal veins extend back to the optic disk. The vessels are evenly distributed. Note that the margins of the optic disk are sharp and clear.

The normal histologic appearance of the retina shows many layers. The lowest layer just above the connective tissue is the layer of rods and cones. Above this are layers of external and internal plexiform and nuclear lamina. The nerve fibers are at the top and collect together to enter the optic nerve at the optic disk.

Here is an example of hypertensive retinopathy. There is arteriolar narrowing and "cotton wool" spots. Additional findings can include hemorrhages into the nerve fiber layer and papilledema.

II-Secondary hypertension: The cause of secondary hypertension are. 1 -One of the most common causes of secondary hypertension is renal artery stenosis, which is a narrowing of the renal arteries due to atherosclerosis. 2 -As a result of the reduced renal blood flow that accompanies the narrowed blood vessels, the kidney responds by activating the renin–angiotensin system that in turn leads to vasoconstriction and salt and water retention. 3 - Hyperaldosteronism(excess aldosterone production) and pheochromocytoma (tumor of the adrenal medulla).

Malignant hypertension: 1 -In a small percentage of patients with chronic essential hypertension, dramatic increases in blood pressure (greater than 120 to 130 mm. Hg diastolic pressure) may occur suddenly. 2 - These sudden increases in blood pressure are termed malignant hypertension and are especially dangerous because dramatic increases in pressure may damage the retina or kidneys and lead to cerebral edema and stroke.

The second form of arteriolosclerosis is shown here. The arteriole here has an "onion skin" appearance typical of hyperplastic arteriolosclerosis. This lesion is most often associated with malignant hypertension.

One complication of hyperplastic arteriolosclerosis with malignant hypertension is fibrinoid necrosis, as seen here in a renal arteriole.

Hypotension: 1 -Hypotension is an abnormally low blood pressure. One common form of hypotension is orthostatic hypotension (also called postural hypotension) that occurs upon standing. 2 -The act of standing initiates a series of reflex responses in the body that are designed to prevent pooling of blood in the lower extremities and a decrease in blood pressure. These reflexes include vasoconstriction in the lower limbs and a reflex increase in heart rate.

Rheumatic heart disease: 1 • Acute, recurrent or chronic inflammation of the heart that may affect the endocardium, myocardium and heart valves. 2 • May occur following throat infection with group Aβ-hemolytic streptococci bacteria, although the exact etiology is unclear. 3 • Primarily a disease of school-age children. Manifestations: 1 • The most serious manifestation is chronic disease of the heart valves that may markedly alter cardiac function and lead to heart failure a number of years later.

Here are flat, pale tan, spreading vegetations over the mitral valve surface and even on the chordae tendineae. This patient has systemic lupus erythematosus. Thus, these vegetations that can be on any valve or even on endocardial surfaces are consistent with Libman-Sacks endocarditis. These vegetations appear in about 4% of SLE patients and rarely cause problems because they are not large and rarely embolize. Note also the thickened, shortened, and fused chordae tendineae that represent remote rheumatic heart disease.

Microscopically, acute rheumatic carditis is marked by a peculiar form of granulomatous inflammation with so-called "Aschoff nodules" seen best in myocardium. These are centered in interstitium around vessels as shown here. The myocarditis may be severe enough to cause congestive heart failure.

Here is an Aschoff nodule at high magnification. The most characteristic component is the Aschoff giant cell. Several appear here as large cells with two or more nuclei that have prominent nucleoli. Scattered inflammatory cells accompany them and can be mononuclears or occasionally neutrophils.

Myocardial infarction: 1 -Myocardial infarction or “heart attack” is an irreversible injury to and eventual death of myocardial tissue that results from ischemia and hypoxia. 2 -Myocardial infarction is the leading killer of both men and women. Most heart attacks are the direct result of occlusion of a coronary blood vessel by a lipid deposit. 3 -These lipid deposits may accumulate to the point where they completely block a coronary vessel or, more commonly, accumulated lipid plaques may break off from the vascular endothelium and act as a thrombus that blocks a coronary artery at a narrower point downstream. Prolonged vasospasm might also precipitate a myocardial infarction in certain individuals.

Manifestations of myocardial infarction: 1. Severe chest pain and discomfort — Pressing or crushing sensation often accompanied by nausea, vomiting, sweating and weakness due to hypotension. A significant percentage of myocardial infarctions are “silent” and have no symptoms. 2. Irreversible cellular injury — Generally occurs 20 to 30 minutes after the onset of complete ischemia. 3. Release of myocardial enzymes such as creatine phosphokinase(CPK) and lactate dehydrogenase (LDH) into circulation from myocardial damaged cells.

4. Electrocardiogram changes — Inversion of T wave, ST elevation, pronounced Q waves. 5. Inflammatory response from the injured myocardium — Leukocyte infiltration, increased white blood cell counts, fever. 6. Coagulative necrosis of the area of the myocardium affected by the infarction. 7. Repair of damaged areas occurs by replacement with scar tissue and not functional muscle tissue; therefore, some alteration in function is inevitable.

Here is an Aschoff nodule at high magnification. The most characteristic component is the Aschoff giant cell. Several appear here as large cells with two or more nuclei that have prominent nucleoli.

The earliest change histologically seen with acute myocardial infarction in the first day is contraction band necrosis. The myocardial fibers are beginning to lose cross striations and the nuclei are not clearly visible in most of the cells seen here. Note the many irregular darker pink wavy contraction bands extending across the fibers.

In this microscopic view of a recent myocardial infarction, there is extensive hemorrhage along with myocardial fiber necrosis with contraction bands and loss of nuclei.

This myocardial infarction is about 3 to 4 days old. There is an extensive acute inflammatory cell infiltrate and the myocardial fibers are so necrotic that the outlines of them are only barely visible.

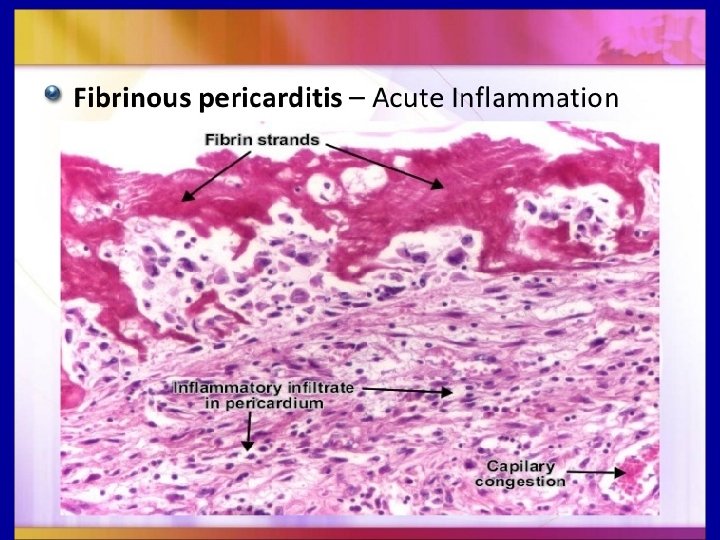
Complications of myocardial infarction: 1. Rupture of weakened myocardial wall. Bleeding into pericardium may cause cardiac tamponade and further impair cardiac pumping function. This is most likely to occur with a transmural infarction. Rupture of the septum between the ventricles might also occur if the septal wall is involved in the infarction. 2. Formation of a thrombo embolism from pooling of blood in the ventricles. 3. Pericarditis — Inflammation due to pericardial friction rub. Often occurs 1 to 2 days after the infarction.

One complication of a transmural myocardial infarction is rupture of the myocardium. This is most likely to occur in the first week between 3 to 5 days following the initial event, when the myocardium is the softest. The white arrow marks the point of rupture in this anteriorinferior myocardial infarction of the left ventricular free wall and septum. Note the dark red blood clot forming the hemopericardium. The hemopericardium can lead to tamponade.

In this case, there was a previous myocardial infarction 3 weeks before, and another myocardial infarction occurred, rupturing through the already thin ventricular wall 3 days later.

4. Arrhythmia — Common as a result of hypoxia, acidosis and altered electrical conduction through damaged and necrotic areas of the myocardium. 5. Reduced cardiac function — Typically presents with reduced myocardial contractility, reduced wall compliance, decreased stroke volume and increased left ventricular end diastolic volume. 6. Congestive heart failure may result if a large enough area of the myocardium has been damaged such that the heart no longer pumps effectively. 7. Cardiogenic shock — Marked hypotension that can result from extensive damage to the left ventricle. The resulting hypotension will trigger cardiovascular compensatory mechanisms that will further tax the damaged myocardium and exacerbate impaired function. Cardiogenic shock is associated with a mortality rate of 80% or greater.

Compensatory mechanisms for myocardial infarction: 1. Catecholamine release — Increases heart rate, force of contraction and peripheral resistance. Catecholamines can, however, be a rrhythmogenic. 2. Sodium and water retention. 3. Activation of renin–angiotensin system leading to peripheral vasoconstriction. 4. Ventricular hypertrophy.

Heart failure: Heart failure is a condition in which the heart is no longer pumping blood effectively. Depending upon the cause, heart failure may be classified as low output failure or high-output failure. 1 - Low-output failure is a reduced pumping efficiency of the heart that is caused by factors that impair cardiac function such as myocardial ischemia, myocardial infarction or cardiomyopathy.

2 - High-output failure, the cardiac output is normal or elevated but still cannot meet the metabolic and oxygen need of the tissues. Common causes of high-output failure include hyperthyroidism (hypermetabolism) and anemia (reduced oxygen-carrying capacity), conditions in which even greatly elevated cardiac output cannot keep up with the increased metabolic requirements of the tissues.
-The left side of the heart is responsible for pumping oxygenated")
I-Left heart failure: (i)-The left side of the heart is responsible for pumping oxygenated blood from the lungs out to the peripheral tissues of the body. (ii)-The most common causes of left heart failure include myocardial infarction, cardiomyopathy and chronic hypertension. (iii)-Left heart failure is also referred to as congestive heart failure due to the pulmonary congestion of blood that accompanies the condition.

Manifestations of left heart failure include the following: 1. Decreased stroke volume, increased leftventricular end-diastolic volume (LVEDV), increasedpreload 2. Congestion of blood in the pulmonary circulation leading to increased pulmonary pressure and pulmonary edema 3. Dyspnea, cough, frothy sputum; “rales” or crackling sounds that may be heard through a stethoscope as a result of fluid accumulation in the lungs.

4. Orthopnea, the accumulation of fluids and dyspnea that are often worse at night or when the patient lies in the supine position because blood and fluids from the lower limbs may redistribute into the pulmonary circulation. 5. Poor perfusion of systemic circulation that may lead to cyanosis. 6. Generalized fatigue and muscle weakness.

II-Right heart failure: Right heart failure often arises as a consequence of left heart failure. 1 - As a result of the increased pulmonary pressure that accompanies left heart failure, the resistance to blood flow now faced by the right ventricle is significantly increased as it pumps blood to the lungs. 2 -Over time, the increased workload on the right ventricle leads to dilation and eventual failure of the right heart. Right heart failure may also result from chronic obstructive pulmonary disease, cystic fibrosis or adult respiratory distress syndrome.

Manifestations of right heart failure include the following: 1. Increased right ventricular workload 2. Venous congestion and distention 3. Peripheral edema, ascites 4. Swelling of the liver with possible injury and eventual failure 5. Gastrointestinal symptoms.
- Slides: 57