Dislocation of the hip joint Three types of


")
of the neck")






 : • Four methods of")



- Slides: 15
Dislocation of the hip joint Three types of hip dislocation : 1. Anterior dislocation ( 10 – 15 %) 2. Posterior dislocation ( 70 % ) 3. Central dislocation ( rest )
Hip joint
Posterior dislocation of hip • Common in the hip joint ( 70 % ) Mechanism of injury : – Dashbroad injury as in RTA – Simple dislocation : - Flexed knee + neutral adduction – Fracture dislocation : - flexed knee + slight abduction
Mechanism that causes the majority of dislocations is impingement (to strike )of the neck of the femoral component against the rim of the cup.
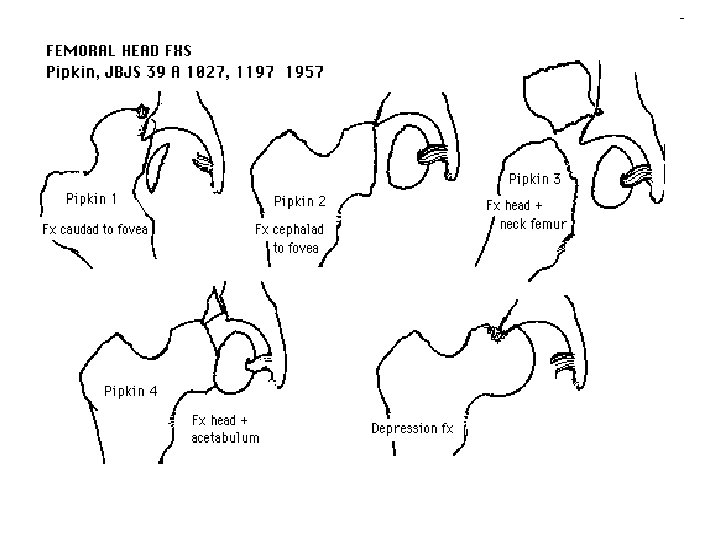
Pipkin Fracture – I - Posterior dislocation of the hip with fracture of the femoral head caudad to the fovea centralis – II - Posterior dislocation of the hip with fracture of the femoral head cephalad to the fovea centralis – III - Type I and type II with associated fracture of the femoral neck – IV - Type I, II, or III with associated fracture of the acetabulum
Femur bone showing fovea centralis
Clinical features – Limb shortening – Flexion , adduction and medial rotation deformity of the affected limb – Thigh rest on the contralateral limb – Head felt in the gluteal region – Movement of hip decrease – Feature of sciatic nerve palsy
Feature of sciatic nerve palsy • SCIATICA or pain localized to the hip, • PARESIS or PARALYSIS of posterior thigh muscles and muscles innervated by the peroneal and tibial nerves, • sensory loss involving the lateral and posterior thigh, posterior and lateral leg, and sole of the foot. - Pain when sitting, sneezing or coughing - tingling sensation or numbness down the leg - Foot drop
Fig: - Foot drop
Radiology • X – ray AP and Lateral view of the pelvis showing both the hip joints • CT scan and MRI ( for acetabular fracture)
Treatment • Closed reduction ( to reduce pain ) : • Four methods of closed reduction : 1. Stimson`s method : – Position : prone , at the edge of the table – An assistant stabilizes the pelvis – Physician applies downward pressure on the calf with one hand while applying external rotation to the femur.
2. Allis traction – Position : supine – An assistant stabilizes the pelvis – The physician simultaneously distract (to pull away ) the femur and rocks it medial to lateral. 3. Bigelow`s method: – Position : supine – Physician applied upwards traction on the femur while an assistant stabilize the pelvis 4. Classical watson`s – jones method : – Position : supine – Limb is brought to the neutral position first then longitudinal traction in the of femur is given.
After treatment • After reduction , the patient is put on a skin traction or immobilised in a Thomas split for 3 weeks. • Full weight bearing after 6 weeks. • Indication of open reduction : – 1. Failure of close reduction : due to obstruction by bony fragments or by soft tissues. – 2. Instability after reduction – 3. Sciatic nerve palsy
Complications Early : – – Sciatic nerve palsy Irreducible fracture dislocation Missed knee injuries Recurrent dislocation Late : – – Myositis ossificans Avascular necrosis of bone Post – traumatic arthritis Unreduced posterior dislocation