DISEASES OF THE EXTERNAL NOSE NASAL VESTIBULE FOREIGN

DISEASES OF THE EXTERNAL NOSE & NASAL VESTIBULE, FOREIGN BODY IN THE NOSE, RHINOLITH, CSF RHINORRHEA Dr. Sheetal Rai Dept of ENT Yenepoya Medical College

SPECIFIC LEARNING OBJECTIVES � List the diseases affecting the external nose � Describe in brief the congenital tumours associated with the nose. � Describe in brief aetiology, clinical features and management of Rhinophyma � List the diseases of the nasal vestibule � Describe nose in brief about Furuncle and Vestibulitis of the

SPECIFIC LEARNING OBJECTIVES �Discuss in brief about foreign bodies in the nose �Discuss the etiopathogenesis, clinical features and management of Rhinolith �Discuss the etiology, clinical features and management of CSF Rhinorrhea

DISEASES OF THE EXTERNAL NOSE � Infection ------ Cellulitis � Nasal deformities ---- Saddle nose Hump nose Crooked /deviated nose � Tumours • Congenital ---- Dermoid cyst Encephalocele or meningoencephalocele Glioma • Benign ------ Rhinophyma • Malignant ------ Basal cell carcinoma Squamous cell carcinoma Melanoma

CELLULITIS � Streptococci � Staphylococci � Superficial spreading inflammation of the nasal skin…. red, swollen and tender nose. � Treatment : Systemic antibacterials Hot fomentation Analgesics.

NASAL DEFORMITIES SADDLE NOSE � Bony/cartilaginous/both bony and cartilaginous �Aetiology 1. 2. 3. : Nasal trauma ------ most common excessive removal of septum in SMR destruction of septal cartilage by - haematoma or abscess, - leprosy, tuberculosis or syphilis.

SADDLE NOSE DEFORMITY

�Treatment : • Augmentation rhinoplasty by filling the dorsum with cartilage, bone or a synthetic implant. • If depression is only cartilaginous ------ cartilage is taken from the nasal septum or auricle. • If deformity involves both cartilage and bone -----cancellous bone from the iliac crest is the best. • • • Autografts are preferred to allografts Synthetic implants ------ silicone or teflon.

HUMP NOSE �May involve the bone or cartilage or both bone and cartilage. �Management • : Reduction rhinoplasty
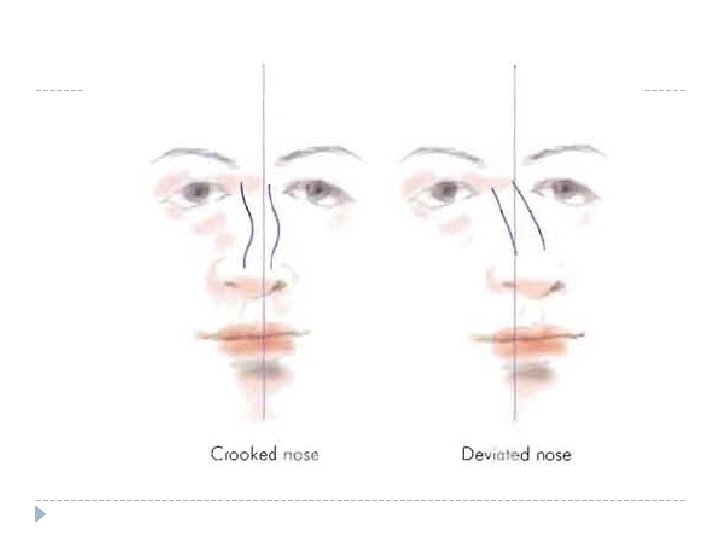

CROOKED OR DEVIATED NOSE �Crooked nose ----- Midline of the nasal dorsum is curved in a C or S shaped manner. �Deviated nose ---- the midline is straight but deviated to one side. �Management • : Rhinoplasty or septorhinoplasty.

CONGENITAL TUMORS DERMOID CYST v Midline swelling under the skin without any external opening. v Represented by a pit or a sinus in the midline of the dorsum of nose. v Hair may be seen protruding through the sinus opening. v The sinus track may lead to a dermoid cyst under the nasal bone or may have an intracranial dural connection ……. ? ? ? meningitis.

DERMOID CYST

DERMOID CYST

Treatment : �Excision of the cyst along with the tract by splitting the nasal bones to remove any extension in the upper part of the nasal septum. �A combined neurosurgical and otolaryngologic approach is required in case of intracranial extension

ENCEPHALOCELE/MENINGOENCEPHALOCELE � Herniation of brain tissue with meninges through a congenital bony defect. � extranasal or intranasal � Extranasal presents as a subcuteneous, pulsatile swelling � Cough impulse – positive and may be reducible. � Treatment : Neurosurgical - severing the tumour stalk from the brain and repairing the bony defect through which herniation has taken place.

Extranasal meningoencephalocele Three varieties : 1. Nasofrontal - in the midline at the root of nose 2. Nasoethmoid – side of nose 3. Naso-orbital - on the anteromedial aspect of the orbit

GLIOMA � Portion of encephalocele that got separated during embryonic development. 60% - extranasal � Firm subcutaneous swelling on the bridge, side of nose or near the inner canthus. � intranasal - 30% � 10% are both intra and extranasal. � � Extranasal gliomas are encapsulated. Can be easily removed by external nasal approach.
 �Haemangioma �Pigmented naevus �Seborrhoeic keratosis")
BENIGN TUMORS �Arise from the nasal skin �Papilloma(skin wart) �Haemangioma �Pigmented naevus �Seborrhoeic keratosis �Neurofibroma �Tumour of sweat glands.
 � Slow-growing benign tumour � Due to hypertrophy of the sebaceous")
RHINOPHYMA (POTATO TUMOUR) � Slow-growing benign tumour � Due to hypertrophy of the sebaceous glands of the tip of nose � Affects men past middle age � Seen in cases of longstanding acne rosacea.

�Presents as a pink, lobulated mass over the nose with superficial vascularity �Obstruction in breathing �Obstruction to vision (due to the large size of the tumour) �Treatment : Paring down the bulk of tumour with sharp knife or carbon dioxide laser and allow the area to reepithelialise. Sometimes, tumour is completely excised and the raw area skin-grafted

MALIGNANT TUMORS BASAL CELL CARCINOMA � Most common malignant tumour involving skin of nose � 40 -60 yrs � Site : tip and ala. � Very slow-growing � Cyst / papulo-pearly nodule / an ulcer with rolled edges. � Nodal metastases extremely rare.

Treatment : �depends on the size, location and depth of the tumour. �Early lesion - cryosurgery, irradiation or surgical excision with 3 -5 mm of skin around the palpable borders of the tumour. �Lesions which are recurrent, extensive or with involvement of cartilage or bone – Wide excision and reconstruction of the surgical defect with local or distant flaps or a prosthesis.
 � Second most common malignant tumour (11%) � 40 -60")
SQUAMOUS CELL CARCINOMA (EPITHELIOMA) � Second most common malignant tumour (11%) � 40 -60 yrs � Side of nose or columella � Infiltrating nodule or an ulcer with everted edges � Nodal metastases in 20% of cases

Treatment : �Early lesions - radiotherapy. �Advanced lesions or those with exposure of bone or cartilage - wide surgical excision with neck dissection with reconstruction of the defect.

MELANOMA Least common � Slow-growing � Superficially-spreading type or nodular invasive type. � Treatment : �Surgical excision

DISEASES OF NASAL VESTIBULE �Furuncle �Vestibulitis �Stenosis �Tumours / Atresia of the nares

FURUNCLE �Acute infection of the hair follicle by Staphylococcus aureus. �Trauma from nose picking or plucking the nasal vibrissae �painful and tender. � skin of nasal tip and dorsum --- red and swollen.

Treatment : � analgesics to relieve pain � topical and systemic antibiotics � If fluctuant (abscess) - incision and drainage under cover of IV antibiotics � DO NOT squeeze or prematurely incise the furuncle ……due to the danger of spread of infection to cavernous sinus through venous thrombophlebitis. Complications : � cellulitis of the upper lip � septal abscess � cavernous sinus thrombosis

VESTIBULITIS � Acute /Chronic diffuse dermatitis of nasal vestibule. � Staph. Aureus � Acute • • Vestibulitis : vestibular skin is red, swollen and tender with crusts and scales covering an area of skin erosion, excoriation. upper lip may also be involved

�Chronic vestibulitis : induration of vestibular skin with painful fissures and crusting. �Treatment : �Cleaning the nasal vestibule of all crusts and scales with cotton applicator soaked in hydrogen peroxide � application of antibiotic-steroid ointment. chronic fissure - cauterised with silver nitrate. �Treat the cause for nasal discharge. �

STENOSIS AND ATRESIA OF THE NARES � Accidental or surgical trauma to the nasal tip or vestibule � Young's operation ---- for treatment of Atrophic Rhinitis � Destructive inflammatory lesions of the nose � Small pox � Congenital atresia Treatment : � Recanalisation by reconstructive plastic surgery

TUMOURS NASOALVEOLAR CYST Benign � presents a smooth bulge in the lateral wall and floor of nasal vestibule. Treatment : � Excision of the cyst by sublabial approach preserving the vestibular skin.

PAPILLOMA OR WART �Benign �single or multiple, �Pedunculated or sessile. Treatment : �surgical excision under local anaesthesia.

SQUAMOUS CELL CARCINOMA �Malignant �Arises from the lateral wall of the vestibule ; may extend into nasal floor, columella and upper lip. �Metastasis to parotid and submandibular nodes. �Treatment : surgical excision or irradiation

FOREIGN BODY IN THE NOSE Seen in children mostly • Organic – seeds, peas • Inorganic - Pieces of paper, chalk, button, pebbles Pledgets of cotton or swabs accidentally left in the nose. � May present immediately if the history of foreign body is known. � If overlooked, the child presents with unilateral foulsmelling nasal discharge, occasionally bloodstained �

Treatment : � Pieces of paper or cotton swabs - removed with nasal packing forceps � Rounded foreign bodies - removed by passing a blunt hook or eustachian catheter past the foreign body and gently dragging it forward along the floor.

� EUSTACHIAN CATHETER TUBE

� In babies and uncooperative children, foreign body removal is done under general anaesthesia with cuffed endotracheal tube � Procedure • • : Endoscopic removal with a forceps Foreign bodies lodged far behind in the nose are pushed into the nasopharynx removed transorally.
 nasal")
�Complications : A foreign body left in the nose may result in: (i) nasal infection and sinusitis. (ii) rhinolith formation. (iii) inhalation into the tracheobronchial tree.

RHINOLITH � Stone formation in the nasal cavity. � Pathogenesis : v Forms around the nucleus of a foreign body, blood clot or inspissated secretion v slow deposition of calcium and magnesium salts v grows into a large, irregular mass ---- pressure necrosis of the septum and/or lateral wall of nose � More common in adults

Symptoms : • Unilateral nasal obstruction • Foul-smelling discharge often blood-stained. • Frank epistaxis and neuralgic pain (from ulceration of the surrounding mucosa)

Treatment : � Removed under general anaesthesia. � Most of them can be removed through anterior nares endoscopically. � Large ones need to be broken into pieces before removal.

� Large rhinoliths particularly hard and irregular ones, require lateral rhinotomy.

CSF RHINORRHEA Flow of CSF through the nose. Aetiology : � Traumatic: • Head injuries • surgery of frontal, ethmoid or sphenoid sinus or hypophysectomy • as a complication of endoscopic sinus surgery � Tumours: osteomas of frontoethmoid region/tumours of the pituitary or the olfactory bulb � Congenital defects in skull associated with encephalocele � Spontaneous

Sites of leakage � Anterior cranial fossa – through cribriform plate, ethmoid air cells or frontal sinus. � Middle cranial fossa - via sphenoid sinus. � Temporal bone fracture ----invovling the tegmen plate result in leakage of CSF into the middle ear ---- via the eustachian tube into the nose ----otorhinorrhoea

�Diagnosis: �History of dribbling of clear fluid from the nose on bending or straining. �Presence of β 2 transferrin is confirmatory for CSF. (absent in nasal secretions or tears. ) �D/D : allergic or vasomotor rhinitis.

CHARACTERISTICS OF CSF RHINORRHOEA 1. 2. 3. 4. 5. clear and watery appears suddenly in a gush of drops uncontrollable cannot be sniffed back. not associated with sneezing, nasal congestion or lacrimation. 6. Allowed to stand, it remains clear (nasal discharge leaves a sediment) 7. Contains glucose

LOCALISATION OF CSF LEAK � Done by intrathecal injection of a dye (fluorescein 5%, 1 ml) or a radioisotope and placing pledgets of cotton in � Olfactory slit ------ Cribriform plate � Middle meatus ------- frontal or ethmoid sinus � Sphenoethmoidal recess ------ Sphenoid sinus � Inferior meatus near the -----Temporal bone eustachian tube Examine the pledgets for dye or radioactivity.

Site of leak can be determined by �CT cisternogram. �MRI cisternogram. �In traumatic CSF leak, when CSF and blood are mixed ------- double ring sign (or target sign) discharge collected un a piece of filter paper shows a central spot of blood while CSF spreads out like a halo around it.

� Treatment : � Early cases are managed conservatively. • semi-recumbent position • avoid blowing of nose, sneezing and straining. • Prophylactic antibiotics to prevent meningitis. � Persistent cases are treated surgically � CSF leak repair ------ endoscopic or intracranial approach. � Nasal endoscopic approach is useful for leaks from the frontal sinus, cribriform plate, ethmoid or sphenoid sinuses.

SUMMARY � Diseases affecting the external nose are varied ranging from infections to tumours. � Infections of external nose need to be diagnosed and treated early due to the risk of spread to cavernous sinus. � Retained foreign body in the nose can lead to rhinolith formation. � CSF rhinorrhea may mimic Allergic or Vasomotor Rhinitis.

Thank you All images have been derived from Google Image Search
- Slides: 53