DISEASES OF THE BLOOD VESSELS HYPERTENSION Dr Eman

DISEASES OF THE BLOOD VESSELS HYPERTENSION Dr Eman MS Muhammad
 n Arteriolosclerosis is a degenerative change of the small arteries")
ARTERIOSCLEROSIS (DIFFUSE HYPERPLASTIC SCLEROSIS) n Arteriolosclerosis is a degenerative change of the small arteries and arterioles caused by persistent hypertension. n Two n The basic types: hyaline and hyperplastic. basic lesions in systemic hypertension are characterized by diffuse arteriolar wall thickening and luminal narrowing → ischemia.

Hyaline arteriolosclerosis • In elderly patients with mild essential hypertension and DM. • • Endothelial injury → leakage of plasma into the arterial wall. Smooth muscles synthesize ECM. Hyperplastic arteriolosclerosis • In malignant hypertension. • Concentric arteriolar thickening with basement membrane reduplication. • Smooth muscles proliferation. • Fibrinoid necrosis (necrotizing arteriolitis)

SYSTEMIC HYPERTENSION n Definition: n Persistent elevation of the systolic and diastolic blood pressure above 140/90 mm of mercury in adult person due to ↑ peripheral resistance in the arterioles.

n General consideration: n Hypertension affects 15 -20% of the population in many developed countries. n It is a major factor in their high mortality from cardiovascular diseases. n Blood pressure rises through childhood and adolescence and reaches the plateau of normal adult level in the third decade.

n There is a good evidence of inverse relationship between the height of the blood pressure and the life expectancy. n Normal blood pressure shows a circadian variation with low levels during sleep. n Stimuli such as, exercise, exposure to cold, emotion and change from a supine to a standing position cause an ↑ in the blood pressure. n In some individuals the blood pressure rise is excessive and the term “labile hypertension” is applied.

n In about 95% of cases of hypertension the cause is not apparent and the patient is said to have primary, essential, or idiopathic hypertension. n In the remaining 5% of cases hypertension is secondary to other disease processes. n Diseases of the kidneys are nearly always responsible for secondary hypertension “renal hypertension”. n Occasional cases results from functioning adrenal tumors or Cushing’s syndrome.

n Hypertension may develop during pregnancy, the so called pre-eclampsia. n Coarctation of the aorta is accompanied by hypertension in the arteries arising proximal to the constriction. n Regardless of the etiology hypertension may be divided into benign and malignant, sometimes also referred to as chronic and accelerated hypertension.

Factors involved in regulation of blood pressure n Normal blood pressure is maintained by factors that regulate the relationship between cardiac output (COP) and total arteriolar resistance. n Vasoconstriction →↑ arteriolar resistance.

n Examples of: • Vasoconstrictors Vasodilators • Angiotensin II Kinins • Catecholamines Adenosine • Thromboxane Prostacyclins • Leukotriens Hydrogen ions • Endothelin Lactic acid

n Regional auto-regulation i. e. ↑ blood flow → vasoconstriction. n COP is regulated by blood volume (sodium load, mineralocorticoids, natriuretic factors), cardiac rate, stroke volume and contractility. n Imbalance between these factors and/or changes in the “set point” → hypertension.
 and is")
Types of systemic hypertension I. Primary or essential hypertension: n Common (95%) and is of two types: a. Benign essential hypertension 90% b. Malignant essential hypertension 10% II. Secondary hypertension: n Uncommon (5%). It is also classified as: a. Benign 80% b. Malignant 20%

Classification and causes of secondary hypertension 1. Renal causes: A. Acute GN B. Chronic GN C. Chronic pyelonephritis D. Renal artery stenosis E. Renin-producing tumors

2. Endocrine causes: A. Cushing’s syndrome B. Pheochromocytoma C. Myxedema D. Thyrotoxicosis

3. 4. Vascular causes: A. Coarctation of aorta B. Polyarteritis nodosa C. Aortic insufficiency Neurogenic causes: A. Psychogenic B. ↑ICT C. Polyneuritis, poliomyelitis

5. Others: A. Pre-eclampsia B. Alcohol abuse C. Renin secreting tumors

ESSENTIAL HYPERTENSION n General consideration: n A common disease which occurs above the age of 40 years. n It is characterized by a slowly progressive rise in the blood pressure and a long course for 30 years or more. n About 90– 95% of cases of hypertension; defined as high blood pressure due to nonspecific lifestyle and genetic factors.

n Lifestyle factors that increase the risk include excess salt, excess body weight, smoking, and alcohol. n Lifestyle changes and medications can lower blood pressure and decrease the risk of health complications. n Lifestyle changes include weight loss, decreased salt intake, physical exercise, and a healthy diet. n If lifestyle changes are not sufficient then blood pressure medications are used.
: n It affects small arteries and")
n Pathological Lesions: I. Vascular Lesions (benign arterioloscierosis): n It affects small arteries and arterioles less than 100 micron in diameter. n The changes occur in the vessels of any structure specially in the kidney, brain and retina.

n The lesion takes a patchy distribution: a. Hyalinosis: • Hyaline change in the intima and media of the small arterioles leading to thickening of the wall and narrowing of the lumen. b. Elastosis: • Hyperplasia and splitting of the internal elastic lamina into several layers affects the larger artetioles and small arteries.
: n Gross picture: n In long standing cases of")
II. Kidney Lesions (Benign nephrosclerosis): n Gross picture: n In long standing cases of hypertension both kidneys are small, contracted and firm (primary contracted kidney). n The capsule is adherent. n The outer surface is finely granular and shows small retention cysts. n The cut surface shows irregular atrophy and fibrosis of the cortex with loss of demarcation between the cortex and medulla. n The arteriole are thick walled and prominent. The peri-nephric fat is relatively increased. n

n Microscopic picture: a. The afferent and efferent arterioles show hyalinosis and elastosis. b. The glomeruli show thickening of the glomerular basement membrane due to ischemia followed by atrophy, fibrosis and hyalinosis of the whole glomerulus. c. The tubules attached to the fibrosed glomeruli undergo atrophy and fibrosis, while the tubule, attached to the functioning glomeruli show compensatory dilatation and may form small retention cysts. d. The interstitial tissue is increased and shows lymphocytic infiltration.
: a. Concentric hypertrophy of the left ventricle due to")
III. Cardiac Lesions (Hypertensive Cardiomyopathy): a. Concentric hypertrophy of the left ventricle due to the high resistance caused by the elevated blood pressure. n The wall becomes thickened, 2 cm or more. n The papillary muscles show hypertrophy and the septum is thickened and bulges into the right ventricular cavity. n Next the left atrium undergoes hypertrophy.

n The hypertrophy enables the heart to remain in a state of compensation for a long time. b. n Eventually decompensation occurs. The myocardium starts to fail and the cavities of the left side dilate.

IV. Retinal Lesions: a. Arteiolosclerosis of the retinal arterioles with compression of the veins. b. Retinal hemorrhages. c. Retinal exudates. V. Cerebral Lesions: n Micro-aneurysms occur in the small cerebral arteries which may rupture causing massive cerebral hemorrhage.

n Etiology: n Genetic factors: n Essential hypertension often run in families, however its mode of inheritance is not clear. n Sodium intake: n The disease is more common in populations with high sodium intake. n Humoral n In vasoconstrictor factors: renal hypertension the ischemic kidney releases renin by the Juxtaglomerular cells.

n Renin acts on a plasma globulin hypertensinogen to form hypertensin which causes constriction in the peripheral arterioles. n In most patients with benign essential hypertension the level of these vasoconstrictor substances are normal, but there is ↑ sensitivity to their pressor effect. n Neurogenic n Stress factors: and emotional stimuli ↑ the sympathetic tone.

Pathogenesis of essential hypertension: I. Defect in renal sodium excretion in addition to excess salt intake leads to → inadequate Na+ excretion → salt & H 2 O retention. n These leads to → ↑ plasma and extra-cellular fluid (ECF). n This leads to ↑COP → ↑ total peripheral resistance → hypertension.

II. ↑Neurohormonal release in addition to excess salt intake, in the presence of generalized defect in Na+/Ca + + transport → ↑vascular reactivity. n The above factors → ↑ total peripheral resistance → hypertension.

Pathogenesis of renal hypertension: n Reno-vascular spasm → renal ischemia → ↑ rennin secretion. Rennin is an important mechanism of hypertension secondary to renal causes. n↑ n Rennin combine with plasma globulin, angitensinogen → formation of angiotensin I which by converting enzyme → ↑ angiotensin II (vasoconstrictor) and aldosterone secretion (→↑Na+ reabsorption). n The subsequent development of AS potentiates the renal ischemia.

n Then the hypertension becomes permanent and progressive as a result of viscous circle producing ↑ renal anoxia and thus further hypertension.

n Causes of Death: 1. Left sided heart failure 2. Cerebral hemorrhage 3. Chronic renal failure (uremia)

MALIGNANT HYPERTENSION n General consideration: n A rare disease affecting mainly the young adults. n It is characterized by a rapid progressive rise in the blood pressure and a short fatal course. n Pathological Lesions: I. Vascular lesions (Malignant Arterioloscierosis): a. Arteriolar hyalinosis and elastosis: Are less marked than in benign hypertension due to the short course of the disease.

b. Cellular hyperplasia: n Concentric hyperplasia of the subendothelial connective tissue and smooth muscles of the media of small arteries and large arterioles. n The vessel becomes narrowed and its wall thickened and shows the onion-skin appearance.

c. Acute arteriolar necrosis: n Fibrinoid necrosis in the wall of the n The vessel wall appears thickened, necrotic and infiltrated by fibrin, RBCs and PMLs. n The lumen is reduced and often show thrombosis. n Hemorrhage occurs. arterioles and small arteries mainly in the kidney, brain and retina (It is the hallmark of malignant hypertension).
: n Gross picture: n The kidneys are of normal")
II. Kidney Lesions (Malignant Nephrosclerosis): n Gross picture: n The kidneys are of normal size. n The capsule strips easily. n The outer surface is smooth and shows focal hemorrhages. n The vessels are prominent, thick and narrow. n If malignant hypertension occurs on top of preexisting benign hypertension, the kidney is reduced in size, granular and shows focal hemorrhages on the surface.

n Microscopic picture: a. Necrosis of the afferent arterioles and glomerular capillaries. b. Hemorrhage in the Bowman’s capsules. c. Cellular hyperplasia in the small arteries. d. Glomerular hyalinosis and tubular atrophy or dilatation may be present.

III. Cardiac Lesions: • Slight hypertrophy of the left ventricle. IV. Retinal Lesions: • Retinal hemorrhages and exudations. V. Cerebral lesions: • Arteriolar necrosis causing massive cerebral hemorrhage may complicate malignant hypertension.

n Causes of Death: 1. Acute renal failure in 95 % of cases. 2. Cerebral hemorrhage. 3. Left sided heart failure.

Clinical presentation: n Hypertension is rarely accompanied by symptoms. n Its identification is usually through screening, or when seeking healthcare for an unrelated problem.

Some people with hypertension report headaches (particularly at the back of the head and in the morning), as well as lightheadedness, dizziness, vertigo, tinnitus (buzzing or hissing in the ears). n These symptoms, however, might be related to associated anxiety rather than the high blood pressure itself. n Others experience fatigue, reduced activity tolerance, palpitations, angina, dyspnea, altered vision or fainting episodes. n Long-term hypertension, however, is a major risk factor for coronary artery disease, stroke, heart failure, peripheral vascular disease, vision loss, and chronic kidney disease. n

n Hypertension may be associated with the presence of changes in the optic fundus. n The severity of the changes typical of hypertensive retinopathy is graded from I-IV. n The severity of the retinopathy correlates roughly with the duration or the severity of the hypertension.

Complications of hypertension n Complications are primarily related to development of atherosclerosis (“hardening of arteries”), or fatty deposits that harden with age

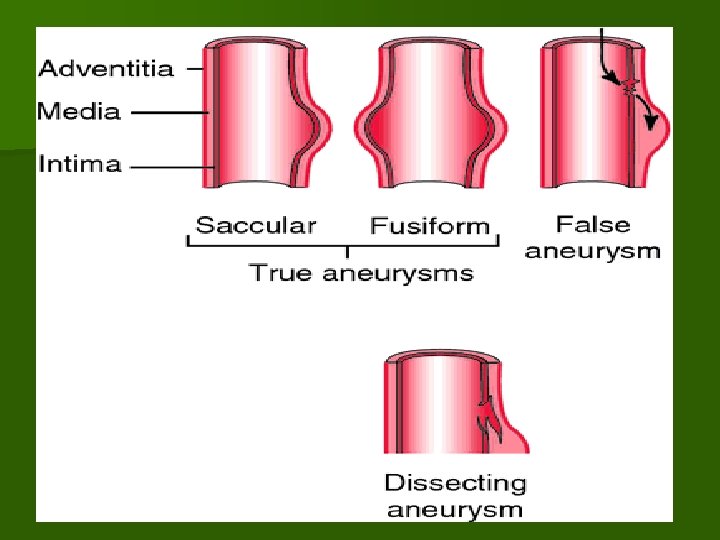
ANEURYSMS n Definition: n It is a localized dilatation in the wall of an artery caused by stretching of the wall. n Aneurysms are caused by lesions which weaken the media of the arteries. n Hypertension helps in the dilatation.

n Symmetrical dilatation stretching the whole circumference produces a fusiform aneurysm, while stretching of part of the circumference causes a saccular aneurysm which bulges on one side of the artery. n The term dissecting aneurysm is a misnomer for what is more correctly described as arterial dissection. n The term aneurysm is loosely applied to conditions which include traumatic and false aneurysm and arteriovenous fistula.

n Etiology: a. Syphilis: Causes aneurysm in the thoracic b. Atherosclerosis: Causes aneurysm in the c. Infected emboli and polyarteritis nodosa: Cause mycotic aneurysms. d. Medionecrosis: Causes dissecting aneurysm e. Congenital weakness of the media: f. Trauma: Causes false aneurysms. aorta. abdominal aorta. in the aorta. Causes congenital cerebral aneurysms.

n Pathogenesis: n The force which expands an aneurysm is the blood pressure, but for an aneurysm to form there must be focal weakening of the media which stretch. n Stretching commonly results in further weakening, so that once an aneurysm has formed it tends to expand, and then commonly ruptures. n The weakness in the vessel wall may be congenital or acquired.
, and vascuitis.")
n The acquired lesions are commonly atheroma, syphilitic arteritis, infection (mycotic aneurysm), and vascuitis. n Types of Aneurysms: 1. True aneurysms 2. False aneurysms

I. True aneurysm: n The wall of the aneurysm is a part of the arterial wall. n The following are the types of true aneurysms: 1. Atherosclerotic Aneurysm: n Occurs in the aorta mainly the abdominal part and the main branches in old age. n The dilatation affects the whole circumference in a segment of the artery, so the aneurysm appears fusiform or spindle shaped. n The aneurysm leads to pressure on the surrounding tissues and its rupture causes fatal hemorrhage.

Aneurysms

2. Syphilitic Aortic Aneurysm: n Fibrosis in the media weakens the wall which will stretch under the effect of the blood pressure and bulges out forming aneurysm. n If only a part of the wall is affected the aneurysm will be sac like, i. e. saccular aneurysm. n If the whole circumference is affected the aneurysm will be fusiform. n The intimal lining of the aneurysm is always degenerated which together with stasis and irregular blood movement in the dilated segment leads to the formation of a laminated thrombus.

n The thrombus does not organize because of the poor blood supply to the wall of the sac (syphilitic end arteritis). n The aneurysm ↑ in size presses on the trachea, esophagus or left recurrent laryngeal nerve. n Aneurysm may bulge forward against the sternum and backward against the vertebrae causing pressure atrophy. n The sac may rupture with fatal hemorrhage. n Rupture occurs in the pleura, pericardium, esophagus or bronchi.

3. Dissecting Aneurysm: It is a rare type and affects the aorta in old age due to: a. Medionecrosis: Focal degeneration and necrosis of the musculoelastic tissue of the aorta in old age. § The cause is a hereditary disorder in the ground substance. § The vasa vasorum in the foci of medionecrosis lose their external support and rupture with hemorrhage inside the media splitting it into two layers.

b. Atherosclerosis and hypertension: § The blood passes through a crack in an atheromatous ulcer in the aorta and splits the media into two layers all around the circumference. § The blood may dissect its way to the aortic branches compressing their excites and causing ischemia. § The intramural blood may rupture through the inner layer of the aorta into the lumen, or rupture to the outside in the pericardium, peritoneum, pleura and periaortic structures.

4. Mycotic aneurysms: Occur in the cerebral, coronary or mesenteric arteries as a result of: a. Emboli containing low virulent organisms as in subacute bacterial endocarditis. b. Polyarteritis nodosa. § Mild inflammation occurs in the arterial wall followed by fibrosis, and small aneurysmal dilatation. § Rupture of the aneurysm is rare, while thrombosis and ischemia is more common.

5. Congenital aneurysms: Single or § They are caused by congenital defects of the media. § Their rupture cause suharachnoid or cerebral hemorrhage. multiple saccular small aneurysms pin’s head to 2 cm in diameter at the points of bifurcation of the cerebral arteries.

II. False aneurysms: § The wall of the aneurysm is not a part of the arterial wall. § The wall consists of fibrous tissue. § Types of false aneurysms are: a. § Pulsating hematoma (simple false aneurysm): Results from trauma to an artery causing a small damage. The escaped blood forms a hematoma in the periarterial tissue.

§ The periphery of the hematoma undergoes organization and forms a fibrous sac which communicates with the artery through a small opening. b. Arterio-venous fistula: Caused by traumatic injury to an artery, and the adjacent vein as that caused by a bullet. § The injury results in either: Ø Aneurysmal varix: Direct communication between the artery and the vein without the intervention of a sac.

§ The blood flows from the artery to the vein which dilates. Ø Varicose aneurysm: A false sac around a hematoma intervenes between and communicates the two vessels.

§ Complications of aneurysms: 1. Pressure atrophy on the surroundings. 2. Spontaneous rupture or as a result of secondary infection causing hemorrhage.

Diseases Of Veins Varicose Veins n Definition: n Dilatation, elongation and tortuousity of the veins. n Sites: a. Superficial veins in the lower limbs specially the saphenous. b. Veins at the lower end of the esophagus (esophageal varices).
. d. Pampiniform")
c. Veins at the lower end of the rectum (piles or hemorrhoids). d. Pampiniform plexus of the spermatic cord (varicocele).

n Causes: 1. Deficient support to the venous wall either congenital or caused by obesity and senility. 2. Congenital defect in the venous muscular coat. 3. Incompetence or rupture of the valves in the veins. 4. Increased pressure inside the veins due to:

a. Prolonged standing. b. Venous compression in pregnancy and by uterine, ovarian, prostatic and rectal tumors. c. Venous obstruction by thrombosis. d. Right sided heart failure causing ↑ in the systemic venous pressure. Liver cirrhosis and bilharzial hepatic fibrosis causing portal hypertension.

n 1. 2. 3. 4. Complications: Phlebothrombosis causing venous congestion and edema. Thrombophlebitis causing pyemia. Rupture causing hemorrhage and pigmentation in the surrounding tissues (local hemosiderosis). Compression and devitalization of the surrounding tissues causes a varicose ulcer as in the lower limbs.

Thank you
- Slides: 67