Diseases of Spleen Splenomegaly Dr C P Bhale
")
Diseases of Spleen, Splenomegaly Dr. C. P. Bhale M. D. (Path)

§ Galen – source of black “black bile’ or § olia”

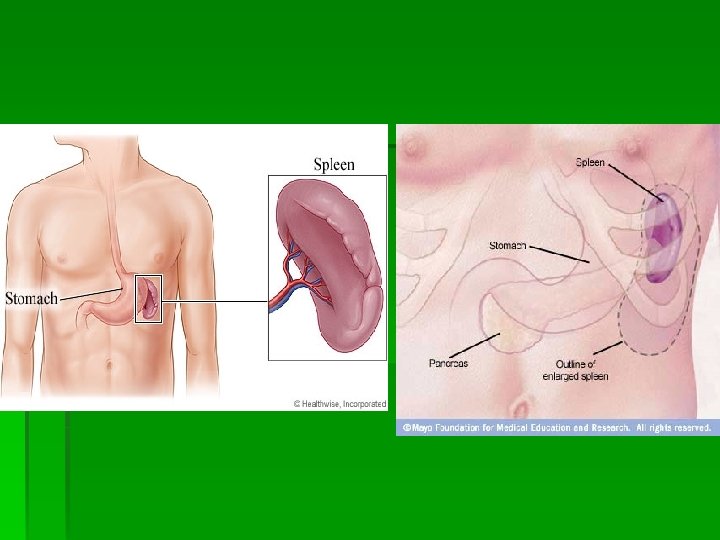
Normal spleen § Normal size – 12 cm length , 7 cm width § weight- < 250 gm § Located along- 9 th, 10 th, 11 th ribs mid-axillary § Spleen should be twice the size to be PALPABLE § Palpable spleens are not always ABNORMAL § 3% normal population has palpable spleen

Bimanual palpation

differences spleen § Sharp edge § Notch –med border § Cross midline § Moves with respiration § Cannot get above it kidney § Round edge § No notch § Not cross midline § Not moves with resp. § Can get above it

Histology - consists of the capsule and trabeculae which enclose the pulp. - 3 zones of the pulp a. White pulp – lymph node; contains lymphocytes, macrophages, and plasma cells in a reticular network b. Red pulp – consists of the cord and sinuses; contains the cellular elements of the blood c. Marginal zone – poorly defined vascular space between pulps; contains sequestered foreign material and plasma as well as abnormal cellular elements
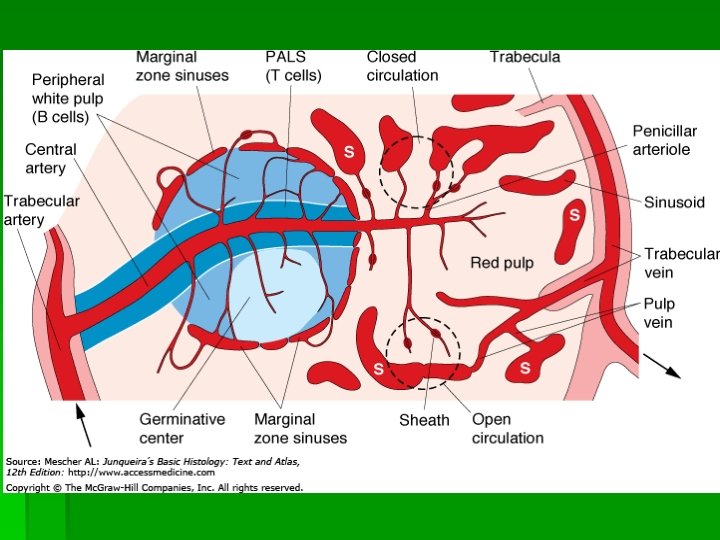

§ The spleen is the major organ of RES. § Blood cells leave the splenic arterial bed through afferent arterioles , which pass through lymphoid nodules(white pulp) and then terminates in the cords of Billroth(red pulp) into which the blood cells are discharged § The normal slow flow permits selective action on the blood cells by macrophages

functions § Quality control over RBC – culling & pitting § Synthesis of antibodies § Removal of antibody coated bacteria & RBC § Source of haemopoietic cells. § Storage of blood

splenomegaly § Mild, moderate, massive § Massive - beyond umblicus, crosses mid line into pelvis (>8 cm) § Moderate- b/w costal margin & umblicus (4 -8 cm) § Mild just palpable (1 -3 cm)

Mechanism of spenomegaly § § § Reactive Reticulo-endothelial hyperplasia Lymphoid hyperplasia Proliferation of lymphoma cells Infiltration by abnormal cells Extramedullary hemopoeisis Proliferation of macrophages due to RBC destruction § Vascular congestion

Causes of splenomegaly § Infective § Hyperplastic § Congestive § Infiltration

infective § Acute & subacute- IMN, infective endocarditis, severe pyogenic inf. Viral hepatitis, CMV, AIDS § Chronic - TB, syphilis, brucellosis § Tropical splenomegaly § Malaria, kala azar, trypanosomiasis

hyperplastic § Extramedullary hemopoeisismyeloproliferative disorders - marrow damage - marrow infiltration § Reticulo endothelial hyperplasia – (abn. RBC) - sickle cell disease, spherocytosis, Hbnopathies, thalassemia major, PNH

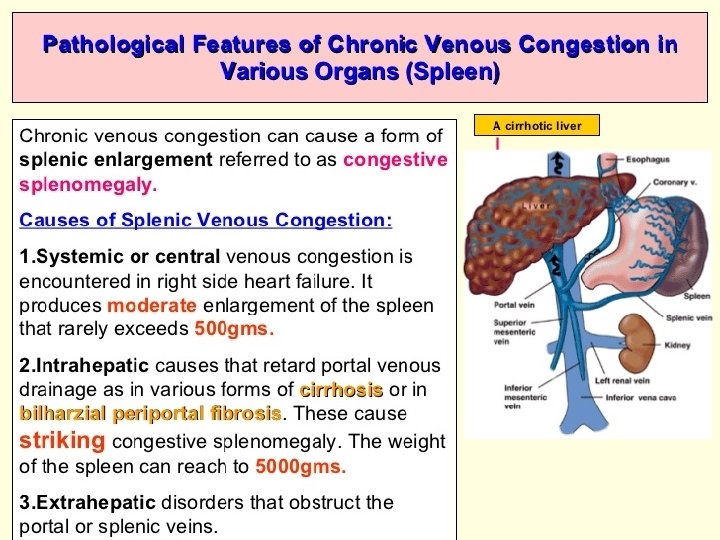
congestive § Intra hepatic obst. portal hypertension - cirrhosis, biliary cirrhosis, hemochromatosis - primary sclerosing cholangitis § Extra-hepatic portal hypertension - venous malf, thrombosis, stenosis - ext. occlusion of portal, splenic vein § Chronic passive congestion of cardiac origin


infiltrative § Malignant infiltration- CML, lymphoblastic - lymhomas, MPD, - angiosarcoma, tumors - metastasis (melanoma) § benign - storage d/s –Gaucher’s, Neiman-pick - amyloidosis - hurler’s syndrome, MPS Cysts, fibromas, hemangiomas, hamartomas -Eosnophilic granulomas

Neoplasms § Primary & Secondary § Benign primary – Fibromas, chodromas, osteomas, Hemangiomas § Malignant – Hodgkin & nonhodgkin lymphoma, Hemangiosarcoma § Metastatic - Melanoma

Disordered immunoregulation § Felty’s syndrome- RA+ splenomegaly+leucopenia § Systemic lupus erythromatosis § Collagen vascular diseases § Sarcoidosis
 § Myelofibrosis § Chronic malaria, kala-azar (trop. Splenomegaly)")
Massive splenomegaly (>8 cm >1000 gm) § Myelofibrosis § Chronic malaria, kala-azar (trop. Splenomegaly) § Hypersplenism § Thalassemia major § Hairy cell leukemia § Gaucher disease
 § § § § Cirrhosis CML Lymphomas‘ Congestive splnomegaly Splenic abscess,")
Moderate splenomegaly(48 cm) § § § § Cirrhosis CML Lymphomas‘ Congestive splnomegaly Splenic abscess, infarct Hemolytic anemias Infectcious mononucleosis
 § Acute infective conditions § Early stages of moderate")
Mild splenomegaly (1 -3 cm) § Acute infective conditions § Early stages of moderate splenomegaly

Step-wise approach to splenomegaly § § History Physical examination Laboratory testings Imaging

history § § § Age , gender Race h/o recent infections like malaria Fever, weight loss, sweating (lymphomas, infections) Pruritis Abnormal bleeding/bruising Joint pain h/o alcholism h/o trauma h/o neonatal umblical sepsis Residence & travel abroad
 Past medical")
History § § …. . cont Jaundice High risk sexual behavior (AIDS) Past medical history Drugs

Physical examination § § § Size of the spleen Hepatomegaly Lymphadenopathy Fever Icterus Bruising, petechiae Oral & supf. sepsis Stigmata of liver disease Stigmata of RA/SLE Splinter hemorrhage, retinal hemorrhage Cardiac murmurs

Lab investigations § § § CBC Blood smear Retic count Blood C/S Serology (fungal, viral, parasitic) LFT Hb electropheresis/ coombs test Coag. profile Amylase/lipase AMA, Anti CCP, RA factor Bone marrow analysis. Radiological Inv

Special situations associated with splenomegaly § Fever- typhoid, malaria, kalaazar, infect. endocarditis, leukemia, lymphoma § Tender spleen- rupture, abscess, infarct § a/c illness+ anemia- AIHA, leukemia § Fever + LN- IMN, leukemia, lymhomas, SLE, sarcoid § Anemia- HA, hemoglobinopathies § Jaundice – cirrhosis, hemolytic anemia § Pulsatile spleen- aneurysm § High ESR- connective tissue disorder § Leukopenia- felty’s syndrome, septicemia

Splenic Infarct § Ischemic necrosis § Casued by Mural thrombi, septic thrombi, Sickle cell anemia, Myelopropiferative disorders, Malignant cell infiltration


- Slides: 34