DISEASES OF MAXILLARY SINUS MANAGEMENT Development Anatomy Mucosalined



 Pyramidal shaped • Base: lateral wall of")



 – Acute (up to 4 weeks)")

 Obstruction of osteomeatal complex – – Anatomical variations (DNS) Mechanical obstruction")







 (fluid level in")
 Post nasal")










")
")
 • Do not obliterate vestibular")








 , Caldwell (1866) § § § § Indications for Caldwell-Luc")




 • Minimally invasive technique in which sinus air cells")




 of antral mucosa Obstruction of gland outlet Mucosal hypertrophy Antral")















- Slides: 68
DISEASES OF MAXILLARY SINUS & MANAGEMENT
Development
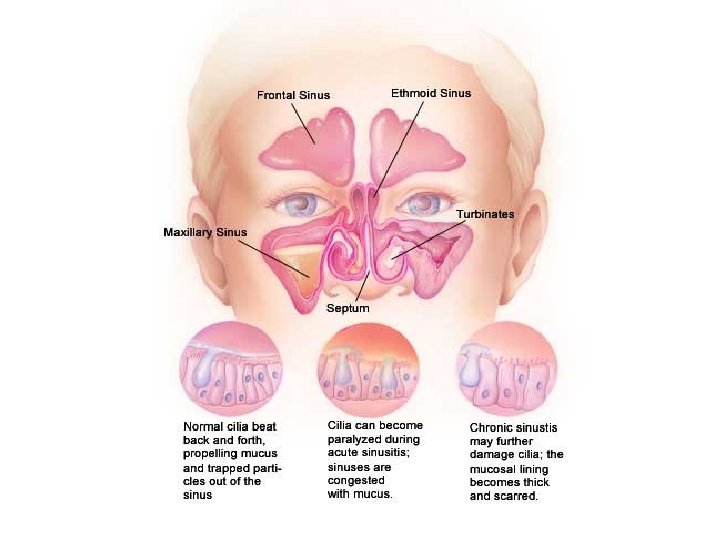
Anatomy Mucosa-lined airspaces within the bones of the face and skull. Four paired sinuses : § Frontal § Ethmoid § Maxillary § Sphenoid sinuses
MAXILLARY SINUS (Antrum of Highmore, sinus maxillaris) Pyramidal shaped • Base: lateral wall of the nose • Apex: Projects into zygomatic process • Roof: Floor of the orbit • Floor: alveolar process of maxilla • Walls: – Anterio-lateral wall: facial surface of body of maxilla – Posterior wall: infratemporal surface of maxilla Sinus
Blood supply: – – Facial Maxillary Infraorbital greater palatine Venous drainage: – anterior facial vein – Pterygoid plexus of veins Innervations (Branches of V 2) – greater palatine nerve – branches of the infraorbital nerve
Applied surgical anatomy • Relation of root apex with floor of sinus • Low incidence of OAC in children • Circumstances with increased incidence of OAC • Canine fossa • Fracture of middle third of the face
Functions of sinuses • Air conditioning • Pressure damping • Reduction of skull weight • Increases olfactory area • Vocal resonance & diminution of auditory feed back 7
Classification of maxillary sinus diseases I. Infection (sinusitis) – Acute (up to 4 weeks) – Subacute (4 -12 weeks) – Chronic (over 12 weeks) II. Traumatic penetration – Oro-antral fistula – Root in the antrum III. Cysts – Intrinsic cyst – Extrinsic cyst IV. Tumors V. Fractures – – Fractures tuberosity Zygomatic complex fractures Lefort fractures (I, III) Orbital floor blow out fractures VI. Miscellaneous – Developmental abnormalities – Diseases of bone – Granulomatous diseases
Maxillary Sinusitis Inflammation of the mucous lining of the sinus Classification: • Acute (up to 4 weeks) • Sub-acute (4 -12 weeks) • Chronic (over 12 weeks)
Predisposing factors: A) Obstruction of osteomeatal complex – – Anatomical variations (DNS) Mechanical obstruction (polyp, tumor, foreign bodies) Rhinitis (URTI, Allergy) Prolonged naso-tracheal intubation B) Decreased muco-cilliary clearance – cystic fibrosis – Kartagener syndrome C) Immuno-compromised state – AIDS – Agammaglobulinemia, Agranulocytosis
Acute Maxillary Sinusitis • Acute inflammation of maxillary sinus lining of less than 4 week duration. • Resolves completely with appropriate treatment Etiology: Dental origin: Non-dental etiology: § Periapical abscess § Direct bacterial contamination § Infected dental cysts § Abnormal clearance mechanism § Oro-antral fistula § Immune deficiency § Peri-implantitis § Periodontal diseases
Clinical features Symptoms: § Fever, headache § Nasal blockage § Mucopurulent nasal discharge § Postnasal drip § Pain over affected sinus § Swelling over cheek Extra oral signs: § Tenderness § Anesthesia § Swelling Intra oral signs: § Presence of OAC § Fetor oris § Pus discharge in mouth
Investigations § Transillumination § Radiography – Water’s view: No changes in early stages, Radio-opacity of affected side – IOPA: Periapical / Pdl infection, OAC
§ Rhinoscopy – Pus draining – Edema & erythema of nasal mucosa § Lab Studies: Attaining sinus cultures - Endoscopic guidance or via puncture techniques
Management Medications • Antibiotics Erythromycin 250 -500 mg 6 th hourly 5 days Amoxicillin 250 -500 mg 8 th hourly 5 days • Decongestants eg. Ephidrine sulphate, Xylometazoline hydrochloride • Mucolytics (Tinc. Benzoin, steam inhalation) • Antihistamines • NSAIDs
Surgical drainage Indication: § When appropriate medical therapy has failed to control the infection § To obtain culture & sensitivity to guide antibiotic selection if empirical therapy has failed Aim: § Remove thick purulent sinus secretion § Enhance mucocilliary flow § Acquire material for culture & sensitivity Technique: § Inferior meatus § Canine fossa
Chronic maxillary sinusitis Prolonged inflammation of maxillary sinus lining of greater than 4 week duration. Etiology • Chronic focus of dental infection • Chronic rhinitis • Allergic condition
Pathophysiology Chronic inflammation Mucosal hyperplasia Loss of mucocilliary function (antral polyp) (fluid level in sinus)
Clinical presentation • • • Asymptomatic Pain & tenderness( in acute exacerbations) Post nasal drip Cacosmia Presence of : OAC, antral polyp
Radiographical picture • • Radio-opacity of the antrum Thickened lining membrane Presence of fluid levels Presence of: OAC, Tooth/Root
MANAGEMENT • MEDICAL MANAGEMENT • INVESTIGATION – Blood & urine – Antimicrobial drugs examination – Nasal decongestant drops (1% ephedrine) – Radiology • Waters view – Analgesics • Ultrasound – Steam inhalation • CT Scan • SURGICAL – Bacteriology – Antral lavage – Endoscopic examination 22 – Functional endoscopic sinus surgery
Antrostomy Surgical formation of opening between the maxillary antrum and the inferior nasal meatus, as treatment for chronic maxillary sinusitis.
Oro-antral communication Pathological communication between maxillary antrum & oral cavity
Etiology: § Extraction of teeth § Destruction of a portion of the floor of the sinus by Periapical lesion § Trauma § Surgery of maxillary sinus § Osteomyelitis of maxilla § Peri-implantitis § Teratomatous destruction of maxilla (gumma)
Symptoms of OAC Fresh OAC: • Escape of fluid from mouth to nose on side of OAC • Epistaxis at site of OAC • Enhanced column of air (Hyper resonant voice) • Excruciating Pain in & around region of sinus In late stages: • Pain ( mild & becomes negligible as the fistula becomes established) • Purulent nasal discharge • Post nasal drip • Popping out of Antral polyp
Diagnosis § Clinical features § Escape of fluid § Nose blowing test – Whistling sound – Escape of air bubbles – Deviation of cotton – Fogging of mirror
Management Purpose: • To protect the sinus from oral micro flora • To prevent escape the fluids & other contents through the communication • To eliminate existing antral pathology • Establish drainage through meatus
Treatment of early cases • Immediate surgical repair to achieve primary closure • Supportive therapy: – Antibiotic prophylaxis – Nasal decongestants – Analgesics
Surgical closure of OAC I. Flaps • Local advancement flaps – Buccal advancement flap – Modified buccal advancement flap (Reherman’s flap) – Palatal rotation flap (Ashley’s operation) • Distant flaps (Tongue flap, buccal pad fat, nasolabial flap) II. Alloplastic material • Gold foil Grafts • Tantalum • PMMA III. Bone grafts
Buccal advancement flap Von Reherman (1936)
Palatal rotational/pedicled flap (Ashley’s operation)
Advantages: • Thicker flap • Adequate Vascularity (better healing) • Do not obliterate vestibular depth Disadvantages: • Palatal tissue less elastic • Risk of hemorrhage • Exposed palatal bone (Increased healing time, Rarely bone necrosis) • Kinking of Greater palatine artery Modifications: • Kruger’s modification • Modified pedicled palatal flap (Iatro & Hara) • Palatal island flap
Modified pedicle palatal flap
Palatal island flap
2. 5 – 3 cm Tongue flap 5– 6 c m 5 – 7 mm
Pedicled buccal fat pad
Naso-labial flap
Root/tooth in the antrum Cause: • Inadvertent use of elevator • Excessive Periapical pressure • Severe Pneumatization of sinus • Impacted maxillary third molars
Diagnosis: • Clinical examination • Radiograph Complications: • Chronic maxillary sinusitis • Discharge of root through antronasal duct (risk of aspiration) • Subdural empyema (death or permanent disability eg: hemiplegia)
Surgical removal: Two approaches § Removal through the tooth socket § Caldwell-luc approach Area of bone removal for caldwell-luc approach and socket approach
Caldwell-Luc procedure Luc (1855) , Caldwell (1866) § § § § Indications for Caldwell-Luc operation: Retrieval of root/tooth from the sinus Enucleation of cyst / mucoceles from sinus Removal of sinus tumors Treatment of acute sinusitis resistant to medical therapy Treatment of chronic sinusitis Management of OAF Repair of fracture of antrum or zygoma
advantages Easy access Thin bone No vital structures surgical procedure 1. Anesthesia 4. Removal of lining, root, cyst etc 2. Incision 5. Hemostasis 3. Bony window 6. Closure
Incision
Bony window
Antral packing Nasal antral window
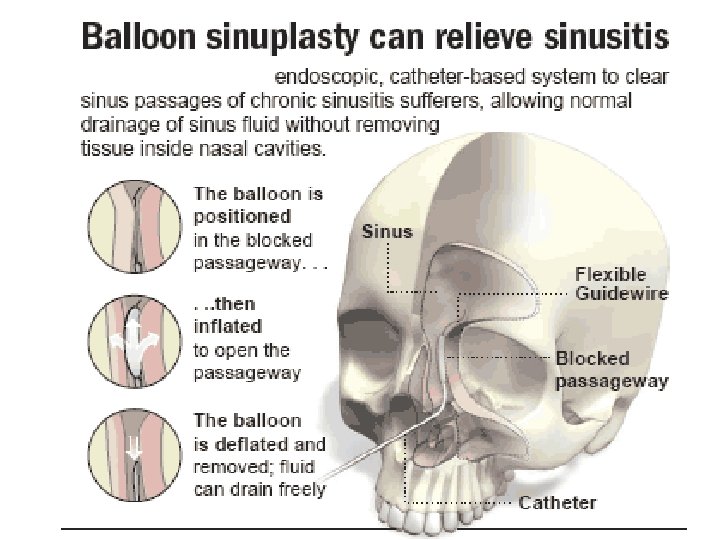
Functional Endoscopic Sinus Surgery (FESS) • Minimally invasive technique in which sinus air cells and sinus ostia are opened under direct visualization. • The goal : restore sinus ventilation and normal function Indication • Chronic sinusitis • Recurrent acute sinusitis
Sinus endoscopy
Surgical Technique
Complications § Blindness resulting from damage to the optic nerve § Cerebrospinal fluid leak § Orbital hematoma § Nasolacrimal duct stenosis
Cysts of maxillary antrum Classification: § Cyst arising from antral lining § Cyst arising from odontogenic epithelium Cyst arising from antral lining: § Secretory § Non-secretory type
Etio-pathogenesis Chronic infection (bacterial/allergic) of antral mucosa Obstruction of gland outlet Mucosal hypertrophy Antral polyp Mucous retention Secretory cyst Cystic degeneration of central portion of polyp Non-secretory cyst
Clinical presentation • • • - Incidence = 2 -10 % Asymptomatic Vague symptoms Facial pain - Neurological sensations Fullness cheeks - Antro-nasla polyp
Radiology: - Dom shaped radiopacity arising from floor/ lateral wall of the sinus - Size = 1 - 4 cm - no bony expansion Aspiration: - Thin yellowish clear fluid which contain protein & cholesterol
Treatment • Asymptomatic maxillary mucosal cyst do not require treatment • Symptomatic cysts may be decompressed By antral puncture • Large cysts may be removed via canine fossa approach
Tumor of maxillary sinus Incidence: • Rare (0. 2 -0. 8% of all malignant disease) • M: F =2: 1 • Age = elderly (above 40 yrs) • More common in south African blacks Etiology: • Chronic infection (sinusitis) • Occupational hazards (Inhaled carcinogens Furniture makers, Foot ware industry)
Signs & symptoms ORAL: swelling, Ulceration, mobility of teeth, ill-fitting denture NASAL: nasal obstruction, epistaxis, epiphora ORBITAL: proptosis, diplopia, eye pain, visual loss INFRATEMPORAL: trismus, pain, paresthesia of mandibular nerve
Investigation Radiology: • Appearance: Cloudy antrum, diffuse opacity or irregular soft tissue outline • Views: Water’s view, OPG, CT scan Biopsy: • Approaches: Caldwell-luc approach, Intranasal antrostomy
WATERS VIEW SHOWING WELL DEFINED OPACITY ENTRAPPED IN SOFT TISSUE SHADOW IN THE RIGHT MAX SINUS
Treatment • Surgery § Partial maxillectomy § Total maxillectomy § Extended maxillectomy with pterygoid fossa dissection Reconstruction of surgical defect: § Mucocutaneous flap § Prosthesis • Radiation • Combination therapy APPROACH
Developmental disorders Cleft palate • Altered nasal air stream • Increased likelihood of Mucosal infection • Thickening of antral lining DNS • Compensatory hyperplasia of Contralateral inferior tribunate & mucosa covering it • Blockage of osteum • Increased chances of sinusitis
Crouzon syndrome • Eary snostosis of sutures • Hypoplasia of maxilla & antrum • High arched palate Treacher collins syndrome • Mandibulofacial dysostosis • Underdeveloped maxillary sinus & malar bone Binders syndrome • Hypoplasia of middle third of the face • Maxillary sinus hypoplasia
Diseases of bone § Fibrous dysplasia § Cherubism § Giant cell lesion Fibrous dysplasia of the right maxillary sinus, displacing the floor of the orbit and causing proptosis of the right eye.
Conclusion
References § The maxillary sinus & its dental implications- David Mac. Gowan § Surgery of the mouth & jaws- J R Moore § Principles of oral & maxillofacial sugery- Robert D Marciani § Textbook of oral & maxillofacial surgery. Neelima Anil Malik § Internet sources
Kartagener syndrome (KS Siewert first described the combination of situs inversus, chronic sinusitis, and bronchiectasis in 1904. However, Manes Kartagener 1 first recognized this clinical triad as a distinct congenital syndrome in 1933. Because Kartagener described this syndrome in detail, it bears his name. Kartagener syndrome (KS) is inherited via an autosomal recessive pattern. Symptoms result from defective cilia motility.
Staging ‘T’ stages of maxillary sinus cancer There are 4 main ‘T’ stages for maxillary sinus cancer • T 1 means the tumour is only in the innermost moist tissues lining the sinus. It has not grown into the bone. • T 2 means the tumour has begun to grow into the bone surrounding the maxillary sinus. (If the tumour is in the bone in the back part of the sinus - the posterior wall - it is T 3. ) • T 3 means the tumour has begun to grow into the back (posterior) wall or into bones of any of the other sinuses. • T 4 means the tumour has grown into any other nearby structures such as the eye, skull, skin of the cheek, the tissues below the temple, the area connecting the back of the nose to the back of the mouth (nasopharynx) , sphenoid or frontal sinuses or up into the brain