Diseases of Large Bowel Diverticulosis of the Colon

Diseases of Large Bowel


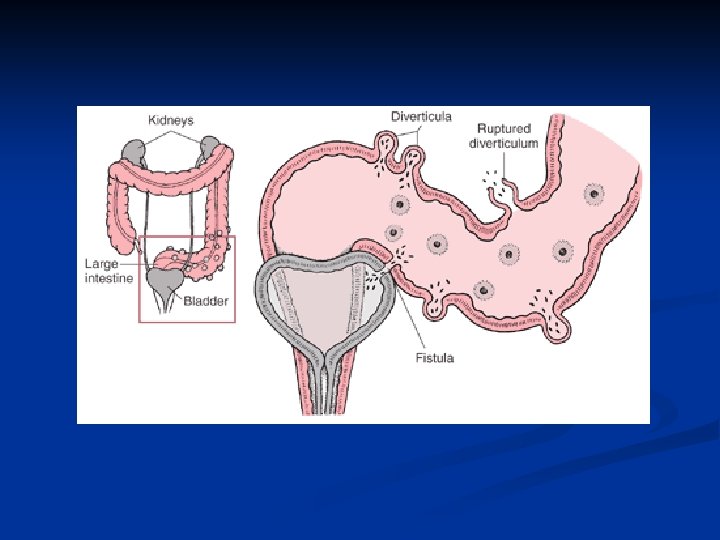
Diverticulosis of the Colon I. Diverticula of the colon are acquired herniations of colonic mucosa protruding through the circular muscle and the wall of large bowel. Localisation - usually in the left part of the large bowel ( sigmoid colon is involved in 90% cases), but they can occur everywhere in large bowel Ethiology - muscular incoordination and hypertrophy resulting in increasing segmentation and intraluminal pressure.

Diverticulosis of the Colon II. n Frequency of the disease is increasing with the age. n Clinical features - the disease is very often asymptomatic, or there are some non specific symptoms due to disordered colonic function ( f. e. distension, flatulence ) n But the symptoms of the complications are usually very serious.

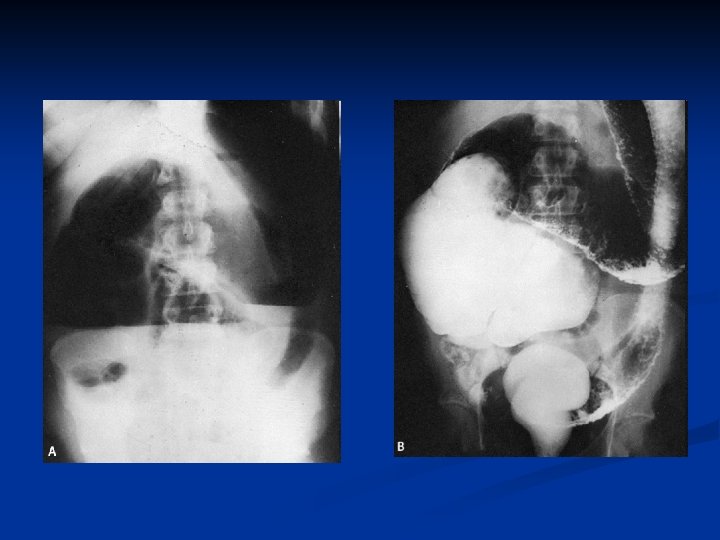
Diverticulosis of the Colon III. Diagnosis n n n clinical examination X-ray picture with barium enema Ultrasonography Colonoscopy Cystoscopy, gynecological examination
 perforation")
Diverticulosis of the Colon IV. Complications: n n n inflammation ( diverticulitis ) perforation bleeding postinflammatory stenosis obstruction fistula with the surrounding organs ( urinary bladder, vagina )

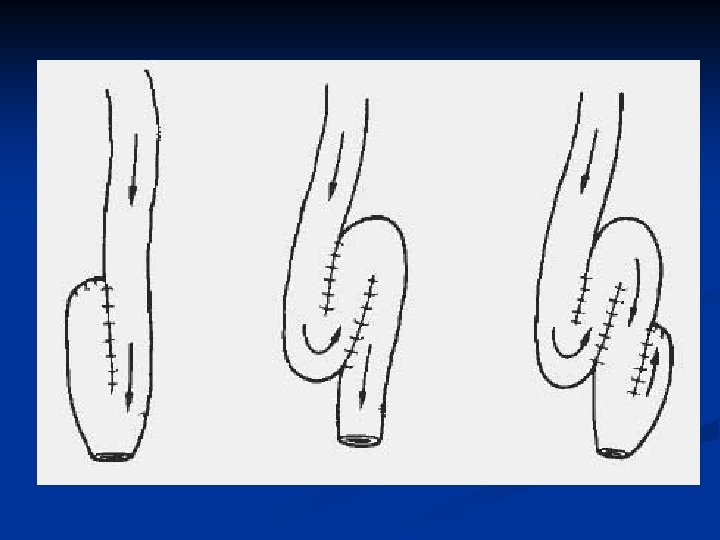
Diverticulosis of the Colon V. Treatment antibiotics, bed rest, liquid diet, spasmolytics ( acute attack of diverticulitis ) operation – 10% patients require operation one stage resection two stage procedures - colostomy - exteriorisation of the affected bowel - Hartman´s procedure - fistulas – resection of the bowel and closure of the fistula


Ulcerative Colitis I. n n Aethiology is inknown – possibly is linked with emotional stress, maybe it is autoimmune disease, secondary infection maybe plays some role. young people Pathology – in 95% cases the disease starts in rectum and spreads proximally. the disease is characterised by appearance of multiple ulcers, sometimes they are discrete sometimes there is a lot of ulcers.

Ulcerative Colitis II. Clinical features : watery diarhoe occuring day and night, rectal discharge of mucus pain, bleeding 2 types : 1. fulminating type 5% temperature, diarhoe containing blood mucus and pus 2. chronic type 95%
")
Ulcerative Colitis III. Treatment : medicaments (antibiotics, corticosteroids, imunossupresive drugs , Remicade ? ) Indications for surgical treatment: 1. to save life ( perforation, toxic megacolon ) 2. local complications, general complications ( liver changes, skin lesions, renal disease, sclerosis cholangitis) 3. risk of carcinoma The method of choice is restorative proctocolectomy

Toxic megacolon I. Clinical term for an acute toxic colitis with nonobstructive colonic dilatation larger than 6 cm and signs of systemic toxicity The dilatation can be either total or segmental. - potentially lethal condition The inflammation extending beyond the mucosa into the smooth-muscle layers and serosa.

Toxic megacolon II. Symptoms: n n High fever Abdominal pain and tenderness Tachycardia Dehydration Mortality : 5 – 10 %

Toxic megacolon III. Three main goals: 1. reduce colonic distension to prevent perforation 2. correct fluid and electrolyte disturbances 3. treat toxemia and precipitating factors Conservative treatment: fluid replacement, antibiotics, steroids, remicade, nasogastric tube, bowel rest Surgical treatment : subtotal or total colectomy.



Tumors of Large Bowel A. Benign tumors B. Malignant tumors

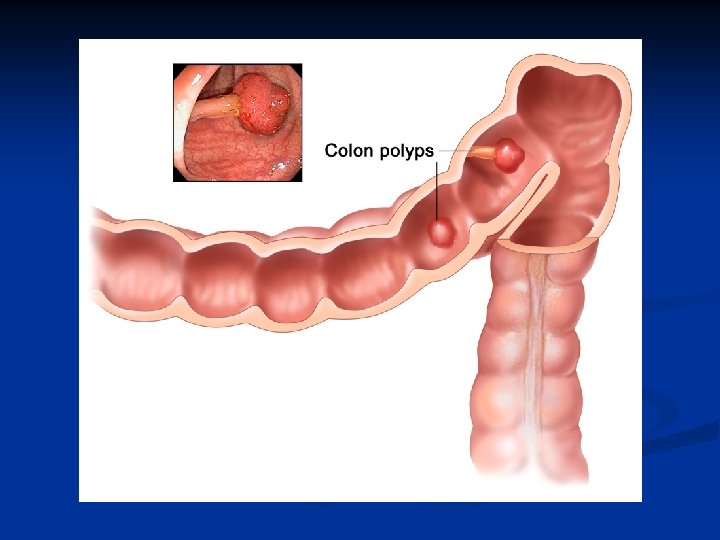
Benign tumors I. n 2 types - tubular adenoma - pedunculated villous adenoma - sessile n They have malignant potential , so they should be removed. Malignancy depends on size and type of adenoma. More dangerous are large and villous adenomas n n

Benign tumors II. Complications - bleeding, - diarrhoe, hypokalaemia / villous / Treatment - fibre endoscopic removal - operation - partial colon resection (very large polyps )


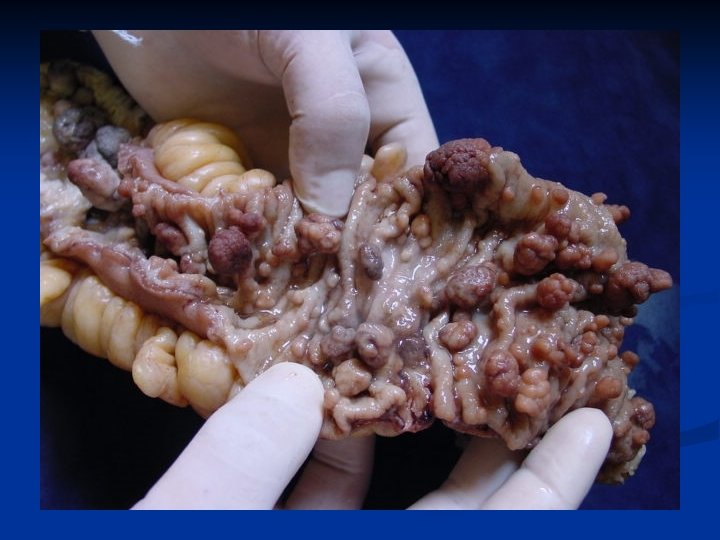
 n hereditary disease. The gene for FAP is on the")
Familial adenomatous polyposis (FAP) n hereditary disease. The gene for FAP is on the long arm of chromosome 5 and is called the APC gene. There a lot of polyps / hundreds/ at the colon and rectal mucosa n very strong malignant potential n Diagnosis : colonoscopy, genetic tests

Familial adenomatous polyposis II. Treatment is surgical 1. colectomy + ileo-rectal anastomosis 2. total colectomy with permanent ileostomy ( cancer ) 3. „ restorative proctocolectomy“ - proctocolectomy with ileal pouch – anal anastomosis




Carcinoma of the Colon I. n n n Colon carcinoma originating in the epithelial cells of the colon M: W=3: 2 25 % of cases present as emergencies with intestinal obstruction or perforation and peritonitis The spread of carcinoma – local spread ( penetration through intestinal wall to surrounding organs ) lymphatic spread to regional or distant lymphonodes spread by the blood-stream to liver

Carcinoma of the Colon II. Typing, Grading, Staging n Typing - the type of tumor – adenocarcinoma - 90% „Signet ring cell “ carcinoma n Grading - well differential carcinoma - moderate differential - poor differential n Staging - spread of the carcinoma Dukes classification TNM classification

Carcinoma of the Colon III. n n n Clinical Features carcinoma of the left side (75% cases): pain, alteration of bowel habit ( irregularity ), palpable tumor, bleeding carcinoma of the right side : aneamia, the presence of a mass in the right iliac fossa Diagnosis endoscopy - sigmoidoscopy, colonoscopy radiography with the barium enema ultrasonography CT

Carcinoma of the Colon IV. Complications - obstruction - perforation with stercoral peritonitis - bleeding Treatment - operation A. radical B. paliative : intestinal by-pass, colostomy Clasic or laparoscopic procedures



Right side hemicolectomy

Left side hemicolectomy

Resection of rectum

Abdominoperineal rescetion of rectum
- Slides: 42