DISEASES OF BUCCAL CAVITY STOMATITIS n It is

DISEASES OF BUCCAL CAVITY

STOMATITIS n It is the general term used for inflammation of oral mucosa, resulting from local or systemic causes. .
 TRAUMATIC STOMATITIS Physical - Ill fitting dentures , Tooth brush Jagged teeth Thermal")
A) TRAUMATIC STOMATITIS Physical - Ill fitting dentures , Tooth brush Jagged teeth Thermal & radiation injury Chemical injury.
 INFECTIVE STOMATITIS Viral – H. simplex, H. zoster ( small multiple, painful vesicles")
B) INFECTIVE STOMATITIS Viral – H. simplex, H. zoster ( small multiple, painful vesicles on lips, buccal mucosa, palate) Bacterial – Vincent’s angina, syphilis, streptococcal Fungal – Candidiasis
 IMMUNE DISORDERS – Aphthous Stomatitis (recurrent ulcerative stomatitis) Behcet’s syndrome D) STOMATITIS WITH")
C) IMMUNE DISORDERS – Aphthous Stomatitis (recurrent ulcerative stomatitis) Behcet’s syndrome D) STOMATITIS WITH CUTANEOUS DISORDERS Erythema multiforme Lichen planus Lupus Erythematosus Bullous Pemphigoid.
 STOMATITIS DUE TO SYSTEMIC CAUSES Vitamin deficiency Malabsorption syndrome Pernicious anaemia Leukaemia Agranulocytosis")
E) STOMATITIS DUE TO SYSTEMIC CAUSES Vitamin deficiency Malabsorption syndrome Pernicious anaemia Leukaemia Agranulocytosis Pancytopenia.
 DRUG ALLERGY Systemic antibiotics Barbiturates Phenytoin Lozenges Tooth paste Mouth washes Dental prosthesis.")
F) DRUG ALLERGY Systemic antibiotics Barbiturates Phenytoin Lozenges Tooth paste Mouth washes Dental prosthesis.

Aphthous Stomatitis n n n Small, shallow, very painful ulcers with clean base & surrounding erythema. Usually involve moveable mucosa Two Types – Minor – 2 to 10 mm Multiple ulcers with central necrotic area and red halo Major – 2 to 4 cm ulcer heals with scar. .

n Aetiology : Unknown n Nutritional deficiency Viral/Bacterial infection Psychogenic Autoimmune Food allergy Treatment : Orodental hygeine Vit. B complex & C Local steroid gel Cauterisation with 10% Ag. No 3 Analgesic lozenges.


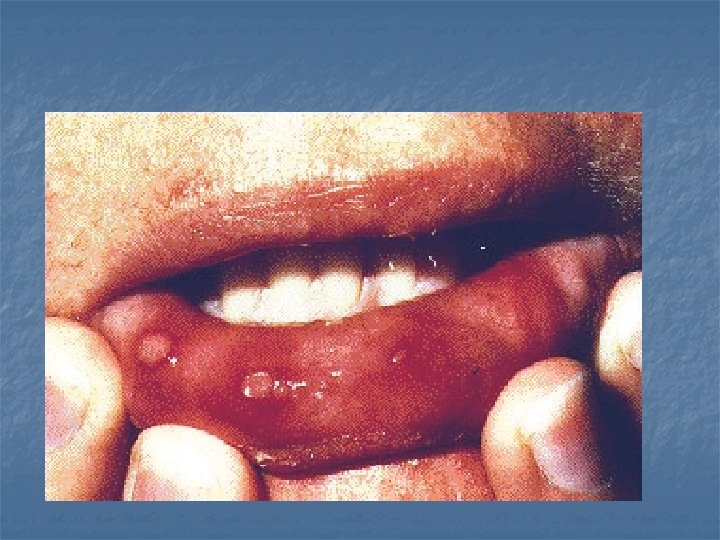
Erythema multiforme Involves skin and mucous membrane n Aetiology- Drug allergy H. simplex Idiopathic n Clinical features- vesicles appear on mucosa , rupture to form ulcers covered with pseudomembrane , bleed easily Common sites – Lips, Buccal mucosa, Tongue - Skin lesion on palms, soles, extremities.

n Treatment- withdraw causative drug steroids antihistaminics.

PREMALIGNANT LESIONS Lichen planus n Premalignant condition of unknown etiology. n Types Reticular- white striae arranged in lace-pattern Erosive- Painful ulcers with keratotic periphery n Treatment- Topical steroids.


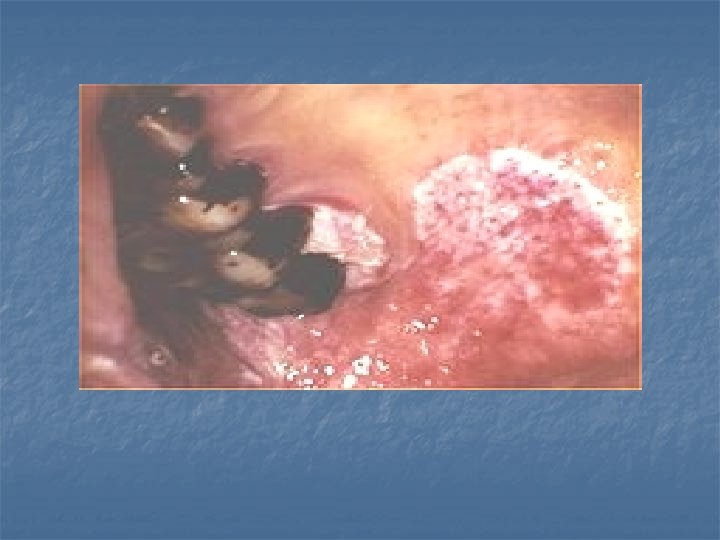
LEUKOPLAKIA n n White patch that cannot be rubbed off & cannot be clinically or pathologically diagnosed as any other disease. Commonest sites- buccal mucosa & oral commisures M: F- - 3: 1, 4 th decade Malignant potential – 1 to 17. 5%.


n n Histologically- hyperkeratosis parakeratosis Aetiology - Chronic irritation Smoking Spirits Spices Syphilis Sharp teeth Sepsis Vitamin deficiency.
Homogenous (b)Nodular (c) Erythroleucoplakia- 25% chances of malignant transformation. n")
Types (a)Homogenous (b)Nodular (c) Erythroleucoplakia- 25% chances of malignant transformation. n

n Treatment – Elimination of irritating factor Biopsy to rule out malignancy & regular follow up Small lesions : surgical/ laser/ cryo excision.

ERYTHROPLAKIA n n n Reddish valvety, macular, flat patches Red colour is due to decreased keratinization of mucosa through which submucosa shines. Histologically- severe dysplasia, CA in situ, invasive carcinoma High malignant potential - 91% Should always be biopsied.

ORAL SUBMUCOUS FIBROSIS Ch. Insidious process characterised by deposition of fibrous & hyaline tissue in sub mucosa of oral cavity & pharynx.

n Aetiology: Tobacco chewing Poor socioeconomic status Alcohol Immune – OSF is cell mediated immune reaction to arecoline in arecanuts Arecoline an alkaloid found in betel nuts stimulates fibroblasts to increase production of collagen Poor dental hygiene Vit. deficiency - A, B-complex , Iron Localized collagen disorder.

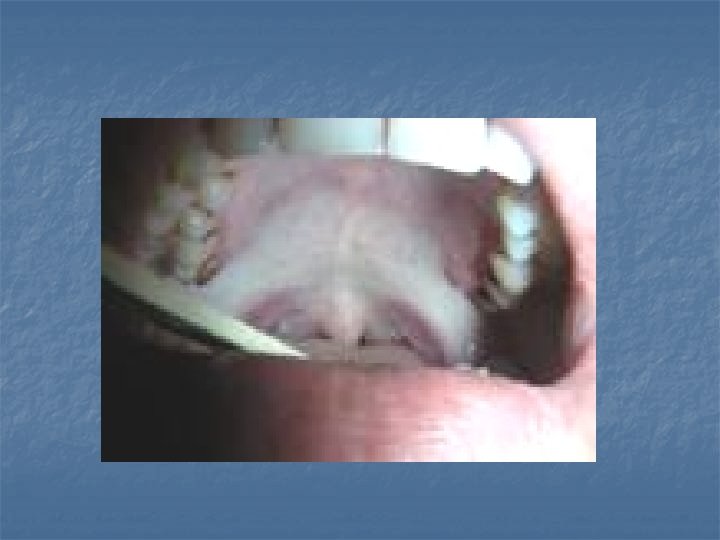
n Clinical Features Whitish bands Difficulty to open mouth & protrude tongue Soreness & Burning sensation of mouth Vesicular eruptions on soft palate Lymphadenitis due to dental infection Malignant transformation in 3 - 7. 6% cases.

n n Changes of OSF are seen in soft palate , pillars & buccal mucosa Initially - Redness with vesiciles formation - Ulceration & Fibrosis Later stages – Blanching & Loss of Suppleness of mucosa due to fibrosis Fibrosis & Scarring of muscles Progressive trismus Poor Oro-Dental Hygiene.

Treatment Medical - Inj. of hyaluronidase with triamcilone / hydrocortisone - Antioxidants - Avoidance of irritant - Treatment of Nutritional deficiencies - Jaw opening exercises.

Surgical - Fibrosis release with KTP or CO 2 lasers & skin grafting - Flaps Bil. tongue flap Nasolabial flap Forearm flap Sup. temporal facia flap & skin graft Surgical excision & buccal pad of fat. - Coronoidectomy & temporal muscle myotomy.
 GEOGRAPHICAL TONGUE Reddish bald patch on tongue")
LESIONS OF TONGUE n n n A) GEOGRAPHICAL TONGUE Reddish bald patch on tongue due to loss of papillae. Irregularly shaped patches are surrounded by keratotic margin (map) Changes position ( migratory glossitis) Asymptomatic, requires no treatment. .


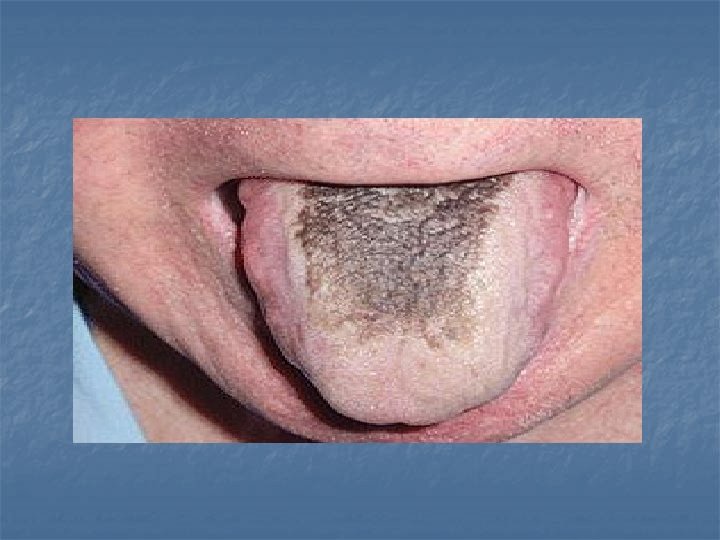
 HAIRY TONGUE Hyperkeratosis of filiform papillae of tongue & the")
n n n B) HAIRY TONGUE Hyperkeratosis of filiform papillae of tongue & the papillae become elongated Papillae become coloured due to bacteria Smoking is causative Treatment – Cessation of smoking Scraping with tongue cleaner Application of diluted H 2 O 2.
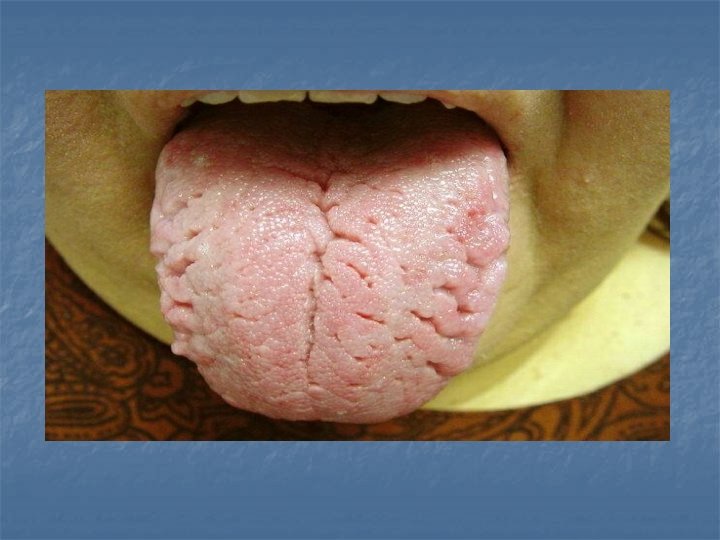
 FISSURED TONGUE n n n Congenital Vit. Deficiency, anaemia, syphilis Melkersson–Rosenthal syndrome :")
C) FISSURED TONGUE n n n Congenital Vit. Deficiency, anaemia, syphilis Melkersson–Rosenthal syndrome : fissured tongue, recurrent facial palsy & swelling of lips.
 TONGUE TIE n n n Ankyloglossia Short frenulum Tongue cannot be protruded beyond")
D) TONGUE TIE n n n Ankyloglossia Short frenulum Tongue cannot be protruded beyond lower incisors Difficulty in pronouncing letters where tongue has to touch upper teeth. Treatment- Transverse release with vertical closure.


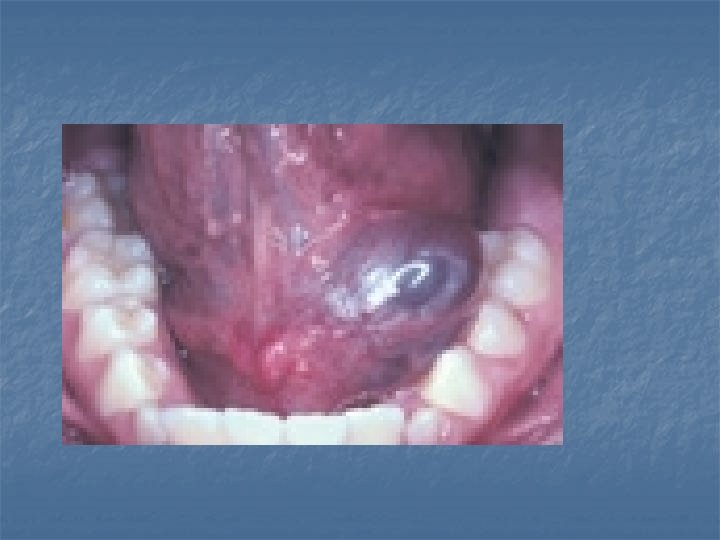
RANULA n n n A painless cystic translucent lesion in floor of mouth on side of frenulum. It’s a retention cyst of sublingual salivary gland due to obstruction of duct by debris present in the floor of mouth. If extends beyond myelohyoid muscle, present as a swelling in submandibular region ( plunging ranula).

Treatment n Marsupilization n Complete excision .

- Slides: 43