Diseases of blood vessels By Dr Nisreen Dahi

Diseases of blood vessels By Dr. Nisreen Dahi Toni Assistant Professor of Pathology Faculty of Medicine

Arteriosclerosis • Definition: Arteriosclerosis is a general term used to include all conditions with thickening and hardening of the arterial walls. • Morphologic types are: I. Hypertensive arteriosclerosis. II. Monckeberg's arteriosclerosis (medial calcific sclerosis). III. Atherosclerosis.

I. Hypertensive Arteriosclerosis: • Term used to describe 3 morphologic forms of vascular disease affecting arterioles and small muscular arteries of patients with hypertension. • Hypertension is persistent elevation of blood pressure (more importantly diastolic pressure) above normal. It may be primary (may be benign or malignant) or secondary. Primary (essential) hypertension is much more common (95% of cases) than secondary and is associated with: a. Genetic factors. b. Environmental factors: - Stress. - Smoking. - Excess salt intake. - Obesity. - Low physical activity.

Types of hypertensive arteriolosclerosis: • Are hyaline arteriolosclerosis, hyperplastic arteriolosclerosis and necrotizing arteriolitis. All are common in hypertension but may occur due to other causes.

1. Hyaline Arteriolosclerosis: • It occurs in hypertensive and diabetic individuals. • Microscopic picture: • The thickened vessel wall shows structureless, eosinophilic and hyaline material in the intima and media.

2. Hyperplastic Arteriosclerosis: • - It is characteristic of malignant hypertension (markedly elevated blood pressure), other causes are scleroderma and toxemia of pregnancy. • • - In this type of arteriolosclerosis, the intima appears with increased thickness. Microscopic picture: Three types of intimal thickening may occur: a. Onion skin lesion consists of loosely placed concentric layers of hyperplastic intimal cells. • b. Mucinous intimal thickening is the deposition of amorphous ground substance. • c. Fibrous thickening of the intima.

3. Necrotizing Arteriolitis: • In cases of severe hypertension and malignant hypertension, parts of small arteries and arterioles show changes of hyaline sclerosis and parts of these show necrotizing process. • • Microscopic picture: - Fibrinoid necrosis of the vessel wall. - Acute inflammatory infiltrate of neutrophils in the adventitia. - Edema and hemorrhage often surround the affected vessels.
: • Definition: • - It is calcification of")
II. Monckeberg's arteriosclerosis (medial calcific sclerosis): • Definition: • - It is calcification of the tunica media of large and mediumsized muscular arteries, especially of the extremities and genital tract. • - The condition occurs as an age-related degenerative process, commonly seen in the elderly individuals. • - Has little or no clinical significance. • Pathogenesis: • Pathogenesis of this condition is unknown. It is considered as an age-related physiologic change due to prolonged effect of vasoconstriction.

III. Atherosclerosis • Definition: • - Atherosclerosis is a specific form of arteriosclerosis affecting primarily the intima of large and medium sized muscular arteries and is characterized by formation of fibrofatty plaques or atheromas. • - The most commonly affected arteries are the aorta, the coronary and the cerebral arterial systems. • Etiology: • - A number of risk factors are associated with increased risk of developing clinical atherosclerosis. • - These risk factors are divided into two groups: • I. Major risk factors. II. Minor risk factors.

• • • Risk Factors of Atherosclerosis: I. Major risk factors: A. Non modifiable: 1. Age (frequency increases with age): - Atherosclerosis is an age-related disease. - Usually appear in the 4 th decade and beyond. 2. Sex: - The incidence and severity of atherosclerosis are more in men than in women. - The lower incidence of IHD in women, especially in premenopausal age, is probably due to high levels of oestrogen and high-density lipoproteins, both of which have anti-atherogenic influence. • 3. Genetic factors. • 4. Familial and racial factors.

B. Modifiable: 1. Hyperlipidaemia: i. The atherosclerotic plaques contain cholesterol and cholesterol esters, largely derived from the apoproteins in the blood. ii. The lesions of atherosclerosis can be induced in experimental animals by feeding them with diet rich in cholesterol. iii. Individuals with hypercholesterolaemia, due to various causes such as in diabetes mellitus, nephrotic syndrome, and familial hypercholesterolaemia, have increased risk of developing atherosclerosis and IHD (ischaemic heart disease). iv. Populations having hypercholesterolaemia have higher mortality from IHD. - The major classes of lipoprotein particles are chylomicrons, very-low density lipoproteins (VLDL), lowdensity lipoproteins (LRL) and high-density lipoproteins (HDL). • Low-density lipoprotein (LDL) is richest in cholesterol and has the maximum association with atherosclerosis. • Very-low-density lipoprotein (VLDL) carries much of the triglycerides and has less marked effect than LDL. • High-density lipoprotein (HDL) is protective against atherosclerosis. - Many studies have demonstrated the harmful effect of diet containing larger quantities of saturated fat (e. g. in eggs, meat, milk, etc) which raise the plasma cholesterol level. - On the contrary, a diet low in saturated fat and high in poly-unsaturated fat (e. g. in fish, fish oils etc) lowers the plasma cholesterol levels.

2. Hypertension: acts probably by mechanical injury to the arterial wall due to increased blood pressure. 3. Diabetes mellitus: the causes of increased severity of atherosclerosis are numerous which include increased aggregation of platelets, increased LDL and decreased HDL. 4. Smoking: the increased risk and severity of atherosclerosis in smokers is due to: a. Reduced level of HDL. b. Accumulation of carbon monoxide in the blood that produces carboxyhaemoglobin and hypoxia in the arterial wall favoring atherosclerosis. II. Minor risk factors: 1. Physical inactivity. 2. Obesity. 3. Oral contraceptives. 4. Lack of exercise. 5. Stress. 6. Consumption of alcohol. 7. High carbohydrate intake. 8. Postmenopausal estrogen deficiency.

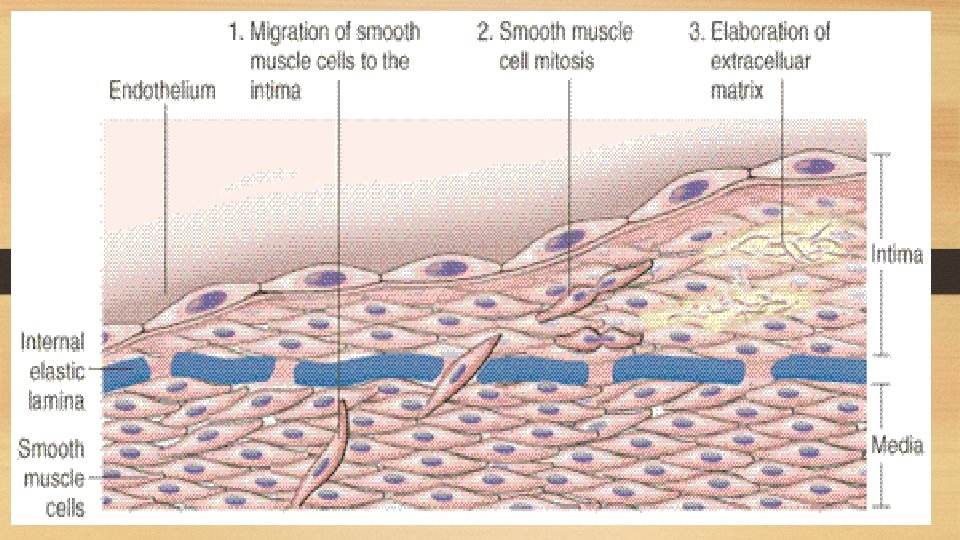
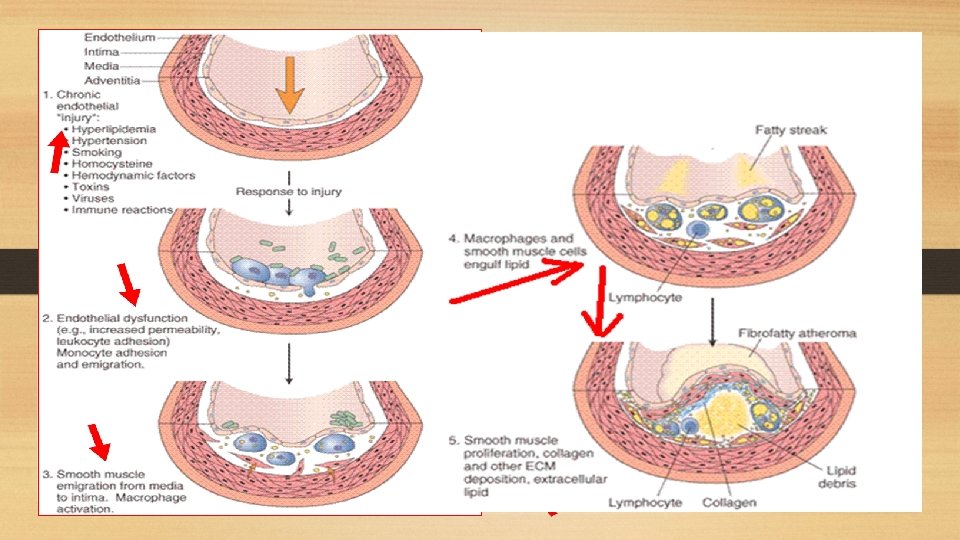
Pathogenesis of Atherosclerosis: i. Endothelial injury: - Is the initial triggering event in the development of lesions of atherosclerosis. - Risk factors such as hypertension, cigarette smoking and chronic hyperlipidemia can cause endothelial damage. ii. Role of blood monocytes: - Plasma LDL on entry into the injured intima undergoes oxidation. - The 'oxidized LDL' performs the following functions on monocytes and endothelium: a. For monocytes, oxidized LDL acts to attract, proliferate, immobilize and activate them to transform it to a lipid-laden foam cell after LDL engulfment. Death of foam cell by apoptosis releases lipid to form lipid core of plaque. b. For endothelium, oxidized LDL is cytotoxic. iii. Smooth muscle cell proliferation: - Endothelial injury causes adherence, aggregation and platelet release reaction at the site of exposed subendothelial connective tissue. - Migration of smooth muscles from media to intima occurs first, followed by Proliferation of smooth muscle cells which is stimulated by various mitogens, the most important of which is platelet-derived growth factor (PDGF).

Pathologic changes: A. Fatty streaks and dots: - The atherosclerotic process occurs gradually within long duration (begins in young age) and starts with formation of what is called fatty streaks and dots on the intima. - By themselves, fatty streaks and dots are harmless but may be the precursor lesions of atheromatous plaques. Gross picture: - The lesions may appear as flat or slightly elevated and yellow. - They may be either in the form of small, multiple dots, about 1 mm in size, or in the form of elongated, beaded streaks. Microscopic picture: - Fatty streaks lying under the endothelium are composed of closely-packed foam cells, lipid-containing elongated smooth muscle cells and a few lymphoid cells. - Small amount of extracellular lipid, collagen and proteoglycans are also present.

B. Atheromatous plaques: - Is a fully developed atherosclerotic lesion, also called fibrous plaque, fibrofatty plaque or atheroma. - Most affected is the abdominal aorta, however it may be seen in descending thoracic aorta and aortic arch. Gross picture: -Are white to yellowish-white lesions, varying in diameter from 1 -2 cm and raised on the surface. - Cut section of the plaque reveals the luminal surface as a firm, white fibrous cap and a central core composed of yellow to yellow-white, soft material.

Microscopic picture: - The appearance of plaque varies depending on the age of the lesion. However, the following features are invariably present: 1. The superficial luminal part of fibrous cap is covered by endothelium, and is composed of smooth muscle cells, dense connective tissue and extracellular matrix containing proteoglycans and collagen. 2. The cellular area under the fibrous cap is formed of a mixture of macrophages, foam cells, lymphocytes and a few smooth muscle cells which may contain lipid. 3. The deeper central soft core consists of extracellular lipid material, cholesterol clefts, fibrin, necrotic debris and lipid-laden foam cells. 4. In older and more advanced lesions, the collagen in the fibrous cap may be dense and hyalinized, smooth muscle cells may be atrophic and foam cells are fewer.

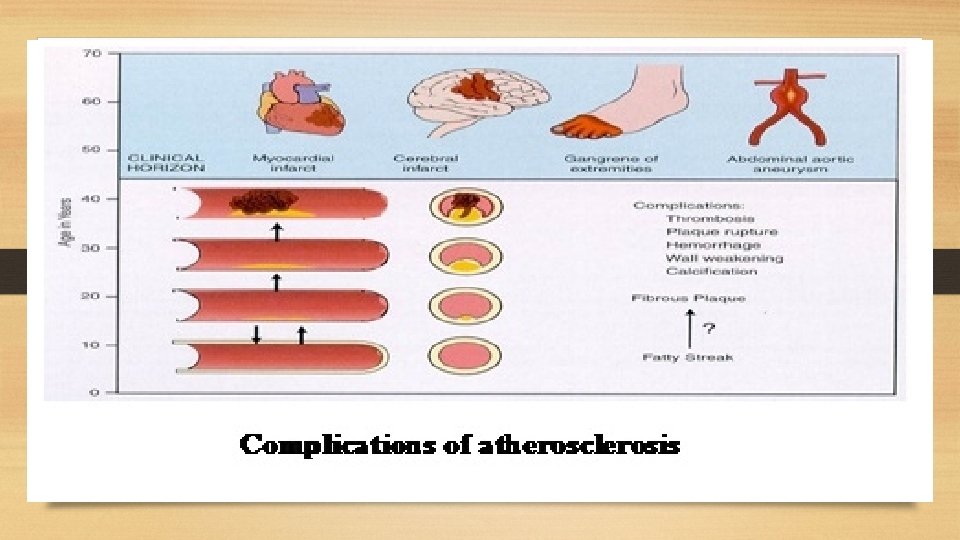
Complications of atherosclerosis: - These account for the most serious harmful effects of atherosclerosis and even death. - It is not uncommon to see more than one form of complication in a plaque. - These changes include: 1. Luminal narrowing: - Causing ischemia or infarction if complete vessel occlusion occurs. 2. Calcification. 3. Ulceration: - The layers covering the soft material of an atheroma may ulcerate. - This results in discharge of emboli composed of lipid material and debris into the blood stream leaving a shallow ulcer with yellow lipid debris in the base of the ulcer. 4. Thrombosis: - The ulcerated plaque and the area of endothelial damage are vulnerable sites formation of superimposed thrombi. 5. Hemorrhage: - Occurs either from the blood in the vascular lumen through an ulcerated plaque or from rupture of thin walled capillaries that vascularize the atheroma. 6. Aneurysm formation: - Due to atrophy, thinning and fragmentation of the internal elastic lamina.

Aneurysms

Definition: An aneurysm is defined as a permanent abnormal dilatation of a blood vessel occurring due to congenital or acquired weakening or destruction of the vessel wall.

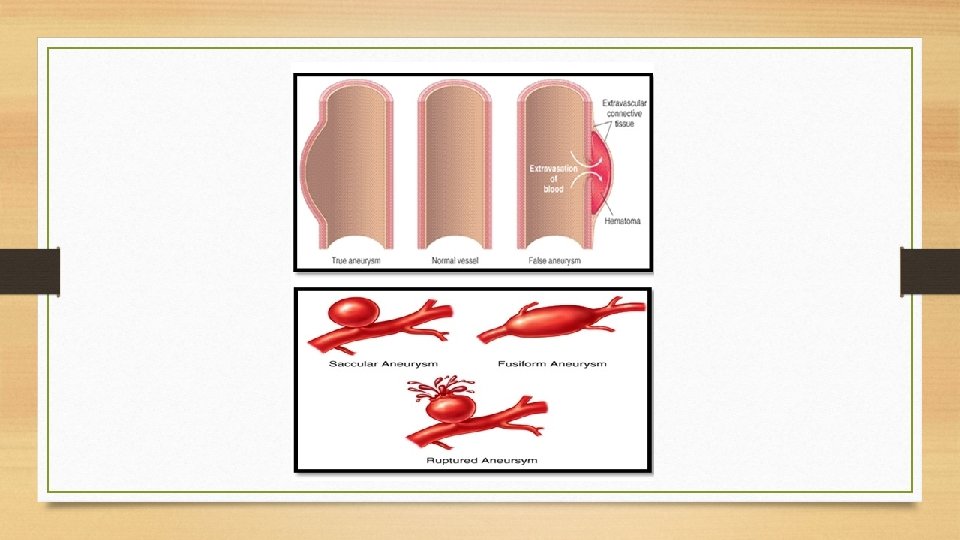
Classification: Aneurysms can be classified on the basis of various features: A. Depending upon the composition of the wall: 1. True aneurysm: composed of all layers of a normal vessel wall. 2. False aneurysm: having fibrous wall and occurring often from trauma to the vessel. B. Depending upon the shape: 1. Saccular having large spherical out pouching. 2. Fusiform having slow spindle-shaped dilatation. 3. Cylindrical with a continuous parallel dilatation. 4. Serpentine or varicose which has tortuous dilatation of the vessel. 5. Berry aneurysms which are small dilatations especially affecting the circle of Willis in the base of the brain. C. Based on pathogenic mechanisms: 1. Atherosclerotic (arteriosclerotic) aneurysms are the most common type. 2. Syphilitic aneurysms found in the tertiary stage of the syphilis. 3. Dissecting aneurysms (Dissecting Hematoma) in which the blood enters the separated or dissected wall of the vessel. 4. Mycotic aneurysms which result from weakening of the arterial wall by microbial infection. The three common types of aortic aneurysms, atherosclerotic, syphilitic and dissecting, are described below.

I. Atherosclerotic Aneurysms: - Atherosclerotic aneurysms are the most common form of aortic aneurysms. - They are most common in the abdominal aorta. Pathogenesis Severe atherosclerotic lesions cause thinning and destruction of the medial elastic tissue resulting in atrophy and weakening of the wall. Pathologic changes - Atherosclerotic aneurysms of the abdominal aorta are most frequently infra-renal. - Atherosclerotic aneurysm is most frequently fusiform in shape and the lumen of aneurysm often contains mural thrombus.

Microscopic picture - The wall of atherosclerotic aneurysm loses its normal arterial structure. - Instead, there is predominance of fibrous tissue in the media and adventitia with mild chronic inflammatory reaction, the intima and inner part of the media show remnants of atheromatous plaques and mural thrombus. Effects: The clinical effects of atherosclerotic aneurysms are due to complications. These are as under: 1. Rupture: the risk of rupture depends on the size and duration of the aneurysm and the blood pressure. 2. Compression: the atherosclerotic aneurysm may press upon some adjacent structures such as compression of ureter. 3. Arterial occlusion: atherosclerotic aneurysms of the abdominal aorta may occlude the inferior mesenteric artery.
 Aneurysms: Pathogenesis - The process begins from inflammatory infiltrate around the")
II. Syphilitic (Luetic) Aneurysms: Pathogenesis - The process begins from inflammatory infiltrate around the vasa vasorum of the adventitia, followed by endarteritis obliterans. - This results in ischaemic injury to the media causing destruction of the smooth muscle and elastic tissue of the media and scarring. - Since syphilitic aortitis is found most frequently in the ascending aorta and in the aortic arch. Pathologic changes Occurring most often in the ascending part and the arch of aorta are saccular in shape and usually 3 -5 cm in diameter. Effects The clinical manifestations are found much more frequently in syphilitic aneurysms than in atherosclerotic aneurysms. The effects include the following: 1. Rupture. 2. Compression. 3. Cardiac dysfunction.

Comparison between atherosclerotic and syphilitic aneurysms:

III. Dissecting Aneurysms and Cystic Medial Necrosis: - Is applied for a dissecting hematoma in which the blood enters the separated (dissected) wall of the vessel and spreads for varying distance longitudinally. Pathogenesis: - is explained on the basis of weakened aortic media. Hypertension predisposes such patients to degeneration of the media in some questionable way. Pathologic changes: - Dissecting aneurysm differs from atherosclerotic and syphilitic aneurysms in having no significant dilatation. - Therefore, it is referred to as 'dissecting hematoma”. - The dissection is seen most characteristically between the outer and middle third of the aortic media so that the column of blood in the dissection separates the intima and inner two-third of the media on one side from the outer one-third of the media and the adventitia on the other.

Diseases of Veins

I. Varicose Veins: Varicosities are abnormally dilated and tortuous veins called varicose veins. -The veins of lower extremities are involved most frequently. -The veins of other parts of the body which are affected are the lower oesophagus (oesophageal varices), the anal region (haemorrhoids). Etiopathogenesis: i. Familial weakness of vein walls and valves is the most common cause. ii. Increased intraluminal pressure due to prolonged upright posture e. g. in nurses, policemen, surgeons, etc. iii. Compression of iliac veins e. g. during pregnancy, intravascular thrombosis, growing tumor. iv. Hormonal effects on smooth muscle. v. Obesity. Pathologic changes: The affected veins are dilated, tortuous, elongated and nodular. Intraluminal thrombosis and valvular deformities are often found. Microscopic picture: There is variable fibromuscular thickening of the wall of the veins due to alternate dilatation and hypertrophy.

II. Phlebothrombosis and thrombophlebitis: Etiopathogenesis: Venous thrombosis that precedes thrombophlebitis is initiated by triad of changes: 1. Endothelial damage. 2. Alteration in the composition of blood. 3. Venous stasis.

Tumors of Blood and Lymphatic Vessels
: 1. Haemangioma (see general). 2. Lymphangioma. 3. Glomus tumor")
A. Benign Tumors (never metastasize): 1. Haemangioma (see general). 2. Lymphangioma. 3. Glomus tumor (glomangioma). B. Intermediate Grade Tumors (rarely metastasize but recurrence is common): 1. Haemangioendothelioma. 2. Kaposi's sarcoma. C. Malignant Tumors (frequent and early metastasis): 1. Angiosarcoma. 2. Lymphangiosarcoma. N. B. Diagnosis of vascular neoplasms may require the use of endothelial cell markers such as Factor VIII or CD-31, especially if clear cut vascular spaces are difficult to see , especially if the tumor is undifferentiated enough to the degree that endothelial lined spaces are not clearly seen.

Lymphangiomas are congenital lesions which are classified as capillary and cavernous. I. Capillary lymphangioma: It is a small, circumscribed, slightly elevated lesion measuring 1 to 2 cm in diameter. The common locations are the skin of head and neck, axilla and mucous membranes. Microscopic picture: Resembles capillary haemangioma but the vascular spaces contain pink colored lymph instead of blood. II. Cavernous lymphangioma: - The common sites are in the region of head and neck or axilla. - A large cystic variety called cystic hygroma occurs in the neck of infants producing gross deformity in the neck. Microscopic picture: Cavernous lymphangioma consists of large dilated lymphatic spaces lined by flattened endothelial cells and containing lymph. Scanty intervening stromal connective tissue is present.

 - These tumors are found most often in the dermis of")
Glomus Tumor (Glomangioma) - These tumors are found most often in the dermis of the fingers or toes under a nail; other sites are mucosa of the stomach and nasal cavity. - These lesions are characterized by extreme pain. Microscopic picture: - They are composed of small blood vessels lined by endothelium and surrounded by aggregates, nests and masses of glomus cells. - The glomus cells are bland round to cuboidal monomorphic cells with scanty cytoplasm.


Haemangioendothelioma It is found most often in the skin and subcutaneous tissue in relation to medium-sized and large veins but can be found in internal organs as liver and lung. Gross picture: The tumor is usually well-defined, greyish red, polypoid mass. Microscopic picture: There are proliferated endothelial cells forming several layers around the blood vessels so that vascular lumina are difficult to identify.

Kaposi's Sarcoma It frequently occurs in patients with AIDS. Classification: Four forms of Kaposi's sarcoma are described: 1. Classic (European) Kaposi's sarcoma: The disease is slow and appears as multiple small purple dome-shaped nodules or plaques in the skin, especially on the legs of elderly males. 2. African (Endemic) Kaposi's sarcoma: This form is common in equatorial Africa. It is found in younger age, especially in boys and in young men and has a more aggressive course than the classic form. The disease begins in the skin but grows rapidly to involve other tissues, especially lymph nodes and the gut. 3. Epidemic (AIDS-associated) Kaposi's sarcoma: The cutaneous lesions are not localized to lower legs but are more extensively distributed involving mucous membranes, lymph nodes and internal organs early in the course of disease. 4. Kaposi's sarcoma in renal transplant cases: - This form is associated with recipients of renal transplants who have been administered immunosuppressive therapy for a long time. - The lesions may be localized to the skin or may have widespread systemic involvement.

Pathologic changes: All forms of Kaposi's sarcoma are similar. Gross picture: The lesions in the skin, gut and other organs form prominent irregular purple dome-shaped plaques or nodules. Microscopic picture: The changes are nonspecific in the early patch stage and more characteristic in the late nodular stage. • In the early patch stage, there are irregular vascular spaces separated by interstitial inflammatory cells and extravasated blood and hemosiderin. • In the late nodular stage, there are slit-like vascular spaces containing red blood cells and separated by spindle-shaped plump tumor cells.


Diagnosis of vascular neoplasms may require the use of endothelial cell markers such as Factor VIII or CD-31, especially if clear cut vascular spaces are difficult to see, especially if the tumor is UNDIFFERENTIATED enough to the degree that endothelial lined spaces are NOT clearly seen.

Angiosarcoma - Malignant vascular tumor occurring in skin or other internal organs. - It is an aggressive tumor and has a poor prognosis. More in old age. Gross picture: Variable appearance ranging from red or violet tumors with multiple vascular spaces to solid tumors with marked hemorrhage and necrosis. Microscopic picture: - Well differentiated angiosarcomas appear as multiple communicating vascular channels lined by malignant cells while poorly differentiated tumors show extensive hemorrhage and necrosis and solid sheets of highly anaplastic cells. - In poorly differentiated angiosarcomas, blood vessels may not be seen and thus vascular markers can be used for diagnosis.

Lymphangiosarcoma - Malignant tumor arising from lymphatic vessels. - It is composed of lymphatic vessels lined by malignant cells. - It may need lymphatic markers as D 2 -40 for diagnosis.

Thank You
- Slides: 47