Diseases of aorta Jakub Honk Kardiologick klinika 2

Diseases of aorta Jakub Honěk Kardiologická klinika 2. LF UK a FN Motol
 Aneurysm of thoracic aorta Aortic dissection")
Overview Anatomy and physiology Abdominal aortic aneurysm (AAA) Aneurysm of thoracic aorta Aortic dissection

Anatomy Ascending aorta ◦ Aortic root ◦ ST junction ◦ Tubular part Aortic arch ◦ Aortic isthmus Descending aorta Abdominal aorta ◦ Suprarenal segment ◦ Infrarenal segment ◦ Bifurcation

Physiology Elasticity, pulse wave

Physiology Arterial stiffness Zieman SJ. Arterioscler Thromb Vasc Biol 2005; 25: 932 -943.

AAA Localized distension of aortic diameter >50% (>3. 0 cm in women, >3. 4 cm in men) 90 % subrenal Progresses over time 5 x more frequent in men Prevalence ↑ with age Multifactorial etiology Risk factors simillar to atherosclerosis, pathophysiology is different - aortic wall remodelling

AAA Clinical features Mostly asymptomatic! Rarely patient palpates pulsatile mass, or feels pulsations Mostly first smyptoms occur due to complications ◦ Peripheral thromboembolism ◦ AAA rupture (first sign in 40%!)

AAA rupture Emergent, life threatening situation Mortality 80– 90 % when optimally treated 90% retroperitoneal rupture Clinical triad ◦ PAIN (amdominal/lumbar, radiation to groins) ◦ PULSATILE MASS ◦ HYPOTENSION (circulatory shock)

AAA diagnostic imaging Duplex ultrasound ◦ Fast, cheap, screening of pts. in risk, follow-up CTA/MRA ◦ Optimal resolution, anatomy DSA ◦ Invasive treatment, luminography Screening ◦ Effective in risk groups (pts. With family history, CAD, PAD, male smokers >65 yrs…) ◦ Prevention of fatal complications, elective operation/inetervention
 Preventive operation/intervention Indication")
Treatment – stable AAA Lifestyle changes, follow-up, blood pressure control (beta-blockers) Preventive operation/intervention Indication based on AAA diameter: > 55 mm > 10 mm increase/year Modified by BSA, sex, comorbidities

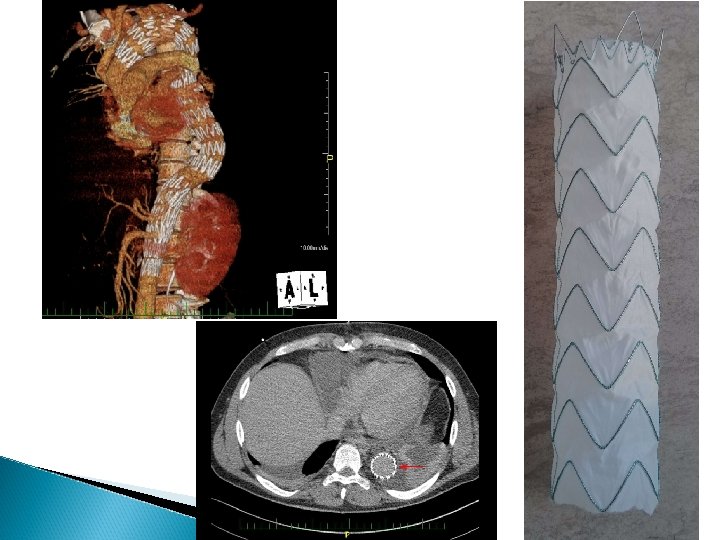
Treatment – stable AAA Surgery ◦ Resection of aneurysmal sac, implantation of vascular prosthesis Endovascular treatment ◦ Implantation of stentgraft ◦ Femoral approch ◦ Simila longterm results to surgery Conservative ◦ Follow-up, risk of rupture

Treatment – ruptured AAA Emergent surgery/endovascular tretament Patient stabilization, fast imaging Up to 50% pts. die before reaching hospital 30 -40% die before reaching op. Theatre 40 -50% of the operated die Overall mortality 80 -90%
 Same definition 60% ascending,")
Aneurysm of thoracic aorta Less frequent than AAA (10/100 000) Same definition 60% ascending, 5 -10% arch, 30 -35% descendning Anuloaortic ectasia
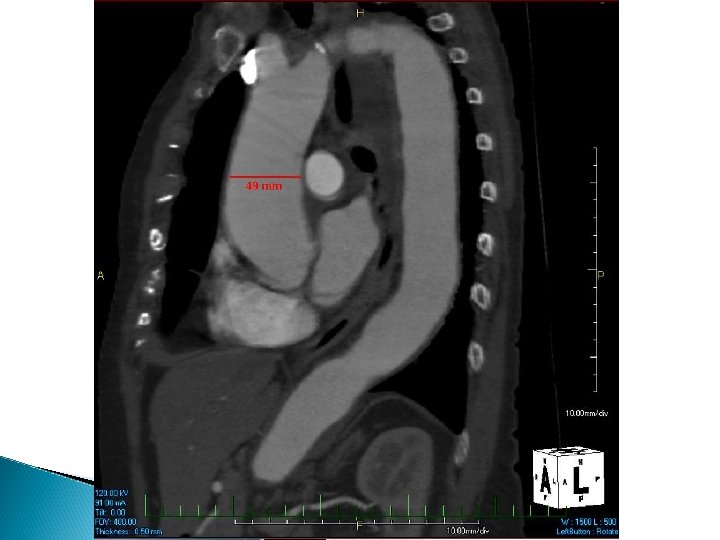

Aneurysm of thoracic aorta Multiple etiologies – genetic, degenerative, infectious, inflammatory Bicuspid aortopathy Cystic medial degeneration Mostly assymptomatic Symptoms of complications: Ao regurgitation, embolization, compression sy. , dissection, rupture Iamging: TTE, TEE, CTA, MRA, DSA

Aneurysm of thoracic aorta Treatment BP control Follow-up Elective surgery Bonow et al. Braunwalds heart disease.

Aortic dissection Incidence: 3/100 000 per year High mortality ◦ Untreated: 25%/24 h, 50%/week ◦ Optimal treatment: 20%/30 days Intimal tear – entry Intimal flap, false lumen Reentry

Aortic dissection risk factors Arterial hypertension Genetically triggered thoracic aortic disease Marfan syndrome Bicuspid aortic valve (bicuspid aortopathy) Ehlers-Danlos syndrome Congenital diseases Coarctation of aorta Tetralogy of Fallot Atherosclerosis of aorta Iatrogenic or blunt trauma Catheterisation or stenting Surgery (CABG, valve replacement, operation of aorta) Intraaortic balloon contrapulsation Trauma (road traffic accidents) Gravidity Cocaine abuse Inflammatory and infectious diseases Takayasu arteritis, giant cell arteritis, syphilis

Aortic Dissection - classification Stanford De Bakey Entry: 65% root, 20% isthmus, 15% other

Aortic dissection Clinical manifestation Pain ◦ severe, sudden, sharp – stabbing, tearing („stabbed in the chestwhit a knife“) ◦ Retrosternal (+radiation to neck, jaw), between scapulae, abdominal, back Acute heart failure, MI, syncope, stroke, paraplegia…

Aortic dissection Diagnostic approach Urgent situation – fast diagnosis Rare disease vs. Common diseases Physical exam, ECG, lab (D dimers) Ideal imaging test – fast, available, good resolution – CTA Trasthoracic echo - bediside


Aortic dissection Therapy Urgent situation, high mortality in first hours Multidisciplinary approach Initial management: BP control (beta blockers) Pain control Hemodynamic stabilization In type A – plan urgent surgery In type B – conservative/ surgery/endovascular

Aortic dissection Therapy
- Slides: 25