Discussion 2 B 8501061 The Intubation Laryngeal Mask

Discussion 2 B 8501061 李又文

The Intubation Laryngeal Mask Airway after induction of General Anesthesia versus Awake Fiberoptic Intubation in patients with difficult airways ANESTH ANALG 2001; 92: 1342 -6 Hwan S. Joo, etc.

Abbreviations TI: Tracheal intubation n AFOI: Awake fiberoptic intubation n ILMA: Intubation laryngeal mask airway n

AFOI

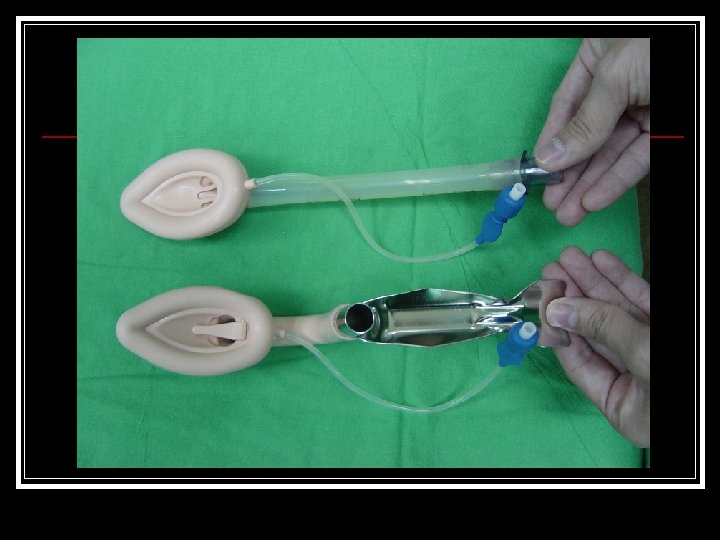
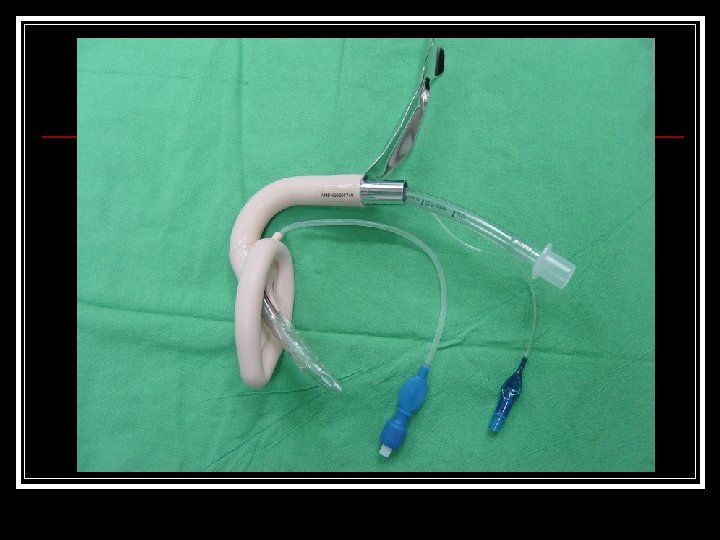
Intubation Laryngeal Mask Airway

AFOI n n n AFOI is the “gold standard” for p’t with suspected or proven difficult airways. ASA “difficult airway algorithm” suggests difficult airways should be intubated awaked. What should we do for patients who are not cooperative or those who refuse AFOI?

Disadvantages of AFOI n n n Oxygen desaturation Tachycardia Hypertension Life threatening AFOI requiring emergency surgical airway has been reported 55% incidence of patient discomfort

ILMA allows confirmation of oxygenation and ventilation before tracheal intubation. n Normal airways: 99% ventilation success rate 97 -99% TI success rate n Difficult airways: Numerous case reports after failed laryngoscopy and failed FOB intubation n

Hypothesis Patients with difficult airways could be successfully and safely intubated after induction of anesthesia using ILMA n Patients would be more satisfied with TI after induction of anesthesia n

Material and Method Prospective and randomized study n ASA class I-III n Patient who required AFOI based on clinical predictors or history of prior difficult intubations n AFOI: 18 ILMA: 20 n

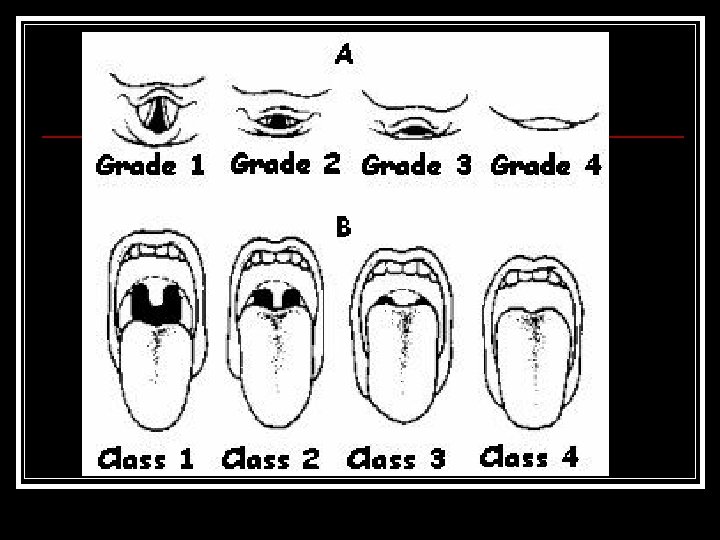
Including Multiple and failed laryngoscopies n Cormack > Grade 3 n Mallampati > Grade 3 n Retrognathia n Thyromental distance < 6 cm n Limited c-spine movement n
 n History of difficult ventilation n At")
Excluding Unstable c-spine n Morbid obesity (BMI>35) n History of difficult ventilation n At risk for aspiration of gastric contents n Mouth opening < 2. 5 cm n Pathological abnormalities of the airway n

n n n Primary anesthesiologist: fully trained anesthesiologist Study investigators experienced with both AFOI and ILMA(>50 cases of each) Study investigators intervened when patient became hemodynamically unstable or primary anesthesiologist was unsuccessful after 20 min using either method or if 4 TI attempt was required in the ILMA group.

ILMA group First: a single blind TI attempt n Second: FOB guidance without ILMA adaptation n Third: Reinsert the ILMA and with FOB guidance n Fourth: study investigator take over with and ILMA reinserted with FOB guide n Fifth: ILMA failure, awake patient for FOI n
 than AFOI group (972")
Results Faster induction times in ILMA (672 ± 545 s) than AFOI group (972 ± 331 s) n AFOI group : all successfully intubated n ILMA group : all successfully ventilated; 50% blind TI ; 25% intubated with FOB guidance without changing ILMA; 15% changing ILMA with FOB guidance; 10% intubated by study investigator n

Oxygenation Minimum oxygen saturation was higher in ILMA at 97. 5 vs AFOI at 94. 5 n AFOI group : oxygen saturation decreased to 62% and 84% in two patients in the n ILMA: one patient decreased to 85% n

Questionnaire Primary anesthesiologist : More comfort with the method of AFOI More experienced with AFOI Predict higher patient satisfaction in ILMA group n Postoperative patients : more satisfied with ILMA induction no recall of TI in ILMA no difference in sore throat and hoarseness n

Conclusion For calm and cooperative patient: no definite advantages other than patients comfort for using ILMA over AFOI n Patient who refuse AFOI or not cooperate may be candidates for TI with ILMA n Experience should be gained before attempting to use ILMA in patient with difficult airways n

Thank you very much!
- Slides: 22