Disclosure I have no conflict of interest to


 • Obesity • Obstructive")






 – – – Polychondritis Ehlers Danlos Syndrome")












 INABILITY TO MOBILIZE SECRETIONS BRONCHOSPASM")









- Slides: 34
Disclosure • I have no conflict of interest to disclose concerning the information provided in this lecture
The Co-Morbid Asthma Condition Often Not Considered Phillip E. Korenblat MD Professor Clinical Medicine Washington University School of Medicine St. Louis, MO
Co-morbid Asthma Conditions • RHINITIS/Sinusitis • Allergic Bronchopulmonary Aspergillosis (ABPA) • Obesity • Obstructive Sleep Apnea (OSA) • Depression • Bronchiectasis • Gastroesophageal Reflux (GERD) • Dysfunctional Breathing • Paradoxical Closure of Vocal Cords • Cystic Fibrosis • COPD with Asthma • Continued Smoking
Tale of Two Patients • 70 yr old male w/ hx childhood asthma. Sx returned as adult, + skin test, FEV 1 reversibility, sx severe & could not practice as a trial lawyer. State of art care w/ well controlled asthma for years. Recent sx of cough and inability to mobilize secretions. Repeat requirement for oral steroids required for symptom relief. • 48 yr old female asthma dx as having asthma after pulmonary infection 6 yrs ago. Sx of expiratory dyspnea and cough w/an inability to mobilize secretions. Rx w/LTRA, LABA/ICS plus repeated oral steroid use. • Airway variability over time without FEV 1 12% & 200 cc reversibility post bronchodilator; neg. skin tests.
Tracheobronchomalacia Presenting as Either a Co-Morbidity or Masquerader of Asthma Phillip E. Korenblat , Andrew Bierhals, Robert Senior • Poorly controlled asthma, despite multiple medications, including combination therapies remains a serious problem • Asthma diagnosis and management can be confounded by other diagnoses or co-morbidities, one of which is tracheobronchomalacia (TBM) • Asthma diagnosis can incorrectly be assigned when a masquerader is present and diagnostic characteristics of asthma are not applied, such as appropriate airway reversibility, although this may be variable • Severity level assessment can be erroneous if co-morbid condition not detected when present
Assigning Severity • Severity level assessment can be erroneous if comorbid condition not detected when present • Severity has taken “ 2 nd seat” to control of asthma • However, severity assessment does include consideration of response to therapy • An unrecognized comorbidity may be the primary reason or complicating factor for poor asthma control
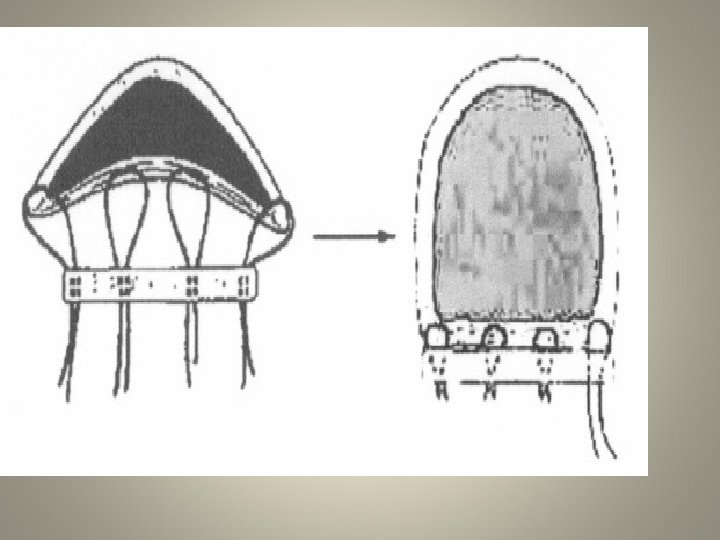
Tracheobronchialmalacia • TBM is defined as a structure of the tracheal & bronchial cartilage which results in any degree of collapse of the lateral cartilaginous walls concurrently producing a lengthening of the posterior smooth muscle membrane of the airway which bridges the C shaped ends of the cartilage
Tracheobroncholmalacia • The incursion of the pars membrane into the airway of the trachea can compromise the air flow from partial airway occlusion and when it occupies ≥ 50% of the airway it meets the consensus definition of tracheal malacia • Recent data by Boiselle et al would challenge the above since they have shown 75% of normal males exceed 50% incursion into the tracheal airway with sustained forceful exhalation • Closure of the main steam bronchi may be present without tracheal malacia
Differential Diagnosis and Considerations Pediatric Tracheomalacia • Congenital – Ehlers-Danlos Syndrome – Trisomy 21 Syndrome – Mounier-Kuhn syndrome (congenital tracheobronchomegally) – Di. Georges Syndrome – Larsen Syndrome – William-Campbell Syndrome • Preterm newborn Chronic Lung • Secondary – Pectus excuvatum/mass causing mechanical compression – TE fistula – Vascular mal-formations – Sequela of intubation – Radiation therapy – Any process causing chronic irritation/inflammation Adapted from Doshi J. Krawlec ME. JACI 2007; 120: 1276 -8
Considerations in Adult Tracheomalacia • Primary (Congenital) – – – Polychondritis Ehlers Danlos Syndrome Trisomy 21 Syndrome TE fistula Tracheomegally (Mournier -Kuhn Syndrome) • 75%diagnosed after age 28 – Vascular Rings – Double Aortic Arch • Secondary (Acquired) – – – – COPD Post Traumatic Radiation therapy External Compression Chronic Infection Chronic Inflammation Amyloidosis
Diagnosis of TBM • Traditionally diagnosed by bronchoscopy and not unusual to see dynamic collapse<50%
Dynamic Trachea & Bronchi CT • 3 sets of images – Inspiration – Forced Expiration – Sustained Expiration • Low radiation dose – 1 to 2 m. Sv (typical chest CT 5 to 7 m. Sv) • 3 D reconstructions to evaluate distribution – Virtual bronchoscopy • Evaluate lung parenchyma
1 2 3 4 5 6 A Inspiration B End Expiration Figure 1. Inspiration and Expiration Views of Tracheobronchomalacia Measurements of the trachea (Case 10, age 74) were made in both inspiration and expiration at the thoracic inlet (1), mid trachea (2), at the carina (3), right main stem bronchus (4), bronchus intermedius (5) and left main stem bronchus (6). Image B. depicts collapse of the trachea and bronchi, retraction of the trachea and air trapping (Red arrow). There is no evidence of emphysema.
Normal TBM Inspiration Expiration • Exaggerated movement of the membranous portion of trachea • Lateral displacement of cartilaginous rings • Great than 50 % loss of cross-sectional area
Tracheal Reconstruction in TBM Inspiration Expiration
Virtual Bronchoscopy Inspiration Expiration
Criteria for Patient Selection to Have 3 D Chest CT Cough which may resemble a seal bark Inability to mobilize secretions Expiratory dyspnea with or without wheezing Prolonged or frequent systemic corticosteroid use • Prolonged (beyond expected asthma exacerbation recovery) or repetitive hospital stays • •
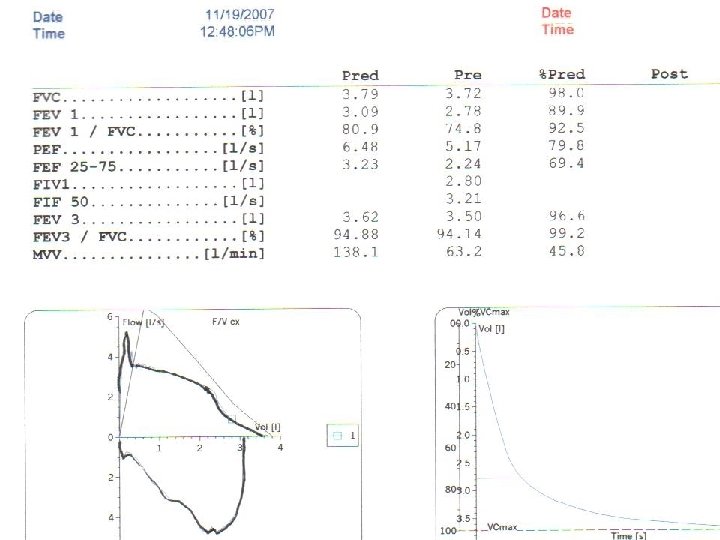
Patient Selection • Pulmonary Function findings that may be present – Decrease in mid flows (MMEF 25 -75%) – Post bronchodilator reversibility reaching or not reaching 12% and 200 cc improvement (i. e. variability without reversibility) – “Birds Beak” or “Double Notch” at peak of full expiration
Phenotypic Determinates of Uncontrolled Asthma • Uncontrolled asthma more frequent in: – ICS users (27. 6%, 35%, 37. 4% well controlled, partly controlled & uncontrolled vs non-ICS users (60%, 23. 9%, 16. 1%) – In ICS users chronic cough or phlegm and female sex most common – In non-ICS users elevated Ig. E and sensitization to mold were associated w/ asthma control – Smoking & rhinitis not associated w/ control Siroux V et al. JACI Oct. 2009; 124; (4) 681 -687
Current Clinical Trial • 59 subjects with physician diagnosed or treated as difficul- to-control asthma • 12 with asthma no TBM (asthma control group) – 6 male 6 females mean age 66. 2 • 27 without 12% & 200 cc reversibility with TBM – 9 males 18 females mean age 58. 2 • 20 with 12% & 200 cc reversibility and TBM or BM – 8 males 12 females mean age 52. 9
CONTROL TBM with Asthma TBM without Asthma Cough 100% Wheeze 100% 95% 90% Mucus 66. 6% 95% 92. 5% Dyspnea 95% 90% 81% Current smoker 0 0 0 Months prior smoker 3/12 17 pk/yrs 6/20 134. 5 pk/yrs 11/27 242 pk/yrs Rhinosinusitis 66. 7% 85% 77. 7% GERD 58% 40% 55. 5% Average Months Symptoms prior Dx 23. 8 78. 2 81. 8 Intubation /surg 66. 6% 80% 77. 7% 58% 50% 55. 5% Months ICS (Average) 2, 079 (173) 2, 776 (138. 8) 2, 449 (90. 7) Months oral steroid 707. 8 (35. 4) 406 (15) Previous chest CT 615 (51)
Tracheal Collapsibility in Healthy Volunteers During Forced Expiration : Assessment with Multidetector CT • Data from Boiselle et al (Radiology 2009; 252(1): 255262) has demonstrated in 25 healthy volunteers (25 men and 26 women) mean age 50 yrs had mean % expiratory reduction in tracheal lumen cross sectional area of 54. 34% in upper trachea and 56. 14% in the lower trachea • Forty (78%) exceeded current diagnostic criterion for tracheomalacia • We have demonstrated trachea collapsibility of ≥ 70% is associated with higher level of malacia in smaller airways
Symptoms May Be Persistent or Intermittent COUGH (“SEAL BARK”) INABILITY TO MOBILIZE SECRETIONS BRONCHOSPASM SYSTEMIC STEROIDS PROLONGED/FREQUENT HOSPITAL STAYS PULMONARY FUNCTION 12% & 200 cc FEV 1 Reversibility & Airway Variability May or may not have “Bird’s Beak” 12% & 200 cc Improvement In FEV 1 Post Bronchodilator Symptoms greater than PFTs reveal Decreased MMEF 25 -75% Minimal Reversibility But Airway Variability
FEV 1 REVERSABILITY 12% & 200 cc Post Dilator MITAGATE ETIOLOGY & EXACERBATING FACTORS TBM DIAGNOSED GO TO MANAGEMENT PROVIDE STATE OF ART ASTHMA MANAGEMENT DYNAMIC 3 D INSPIRATORY EXPIRATORY CHEST CT CONTINUED SYMPTOMS
Treatment When a TBM Co-morbidity of Asthma • Evaluate the etiology of their asthma Ig. E non-Ig. E Infectious Other • Determine causative factors for continued symptoms • Mitigate exacerbating factors and comorbidities, especially GE reflux • Institute state of the art asthma management
AIRWAY VARIABILITY WITHOUT FEV 1 Reversability 12% & 200 cc Post Bronchodilator DYNAMIC 3 D CHEST CT TBM DIAGNOSED Go To Management
Treatment When a Masquerader of Asthma • Only when appropriate include measures usually employed with asthma (some may have a degree of reversibility) • Recognize that corticosteroids may have adverse effect due to drying and increase mucus viscosity • Management measures common to TBM regardless if co-morbidity or the primary diagnosis: adequate hydration, mucus clearing flutter valve, chest percussion device, bronchoscopy, temporary stent, tracheoplasty
Enter the Surgeon
INTERVENTION CASE #1 FECV 1 REVERSABILITY • DYNAMIC 3 D CT DIAGNOSED TBM • LABA/ICS • ADEQUATE HYDRATION • DAILY PERCUSSION VEST • ORAL CORTICOSTEROIDS HALTED CASE #2 FEV 1 VARIABILITY • DYNAMIC CT DIAGNOSED TBM • PRESERVED LUNG FUNCTION (without FEV 1 12%/200 cc reversibility) • DAILY SYMPTOMS • SURGICAL REPAIR OF TRACHEA & MAINSTEAM BRONCHI • NO FURTHERAPY REQUIRED
Conclusion • TBM is not rare. It should be considered in asthma-like situations that have atypical features, especially the need for repeated use of systemic corticosteroids to help with airway mucus clearance • Normal or near-normal spirometry does not exclude the diagnosis of TBM • TBM may be a significant co-morbid condition with asthma or the primary diagnosis of symptoms which may be (a masquerader) confused with asthma • Trachea collapsibility of ≥ 70% is associated with higher level of malacia in smaller airways • 3 D chest CT is a precise means of imaging the airways for TBM. However, the current criteria for diagnosis of tracheomalacia of 50% airway collapse will need to be revisited given data from Boiselle and Limanovich group
Conclusion • TBM is not rare. It should be considered in asthma-like situations that have atypical features, especially the need for repeated use of systemic corticosteroids to help with airway mucus clearance • Normal or near-normal spirometry does not exclude the diagnosis of TBM • TBM may be a significant co-morbid condition with asthma or the primary diagnosis of symptoms which may be (a masquerader) confused with asthma • Trachea collapsibility of ≥ 70% is associated with higher level of malacia in smaller airways • 3 D chest CT is a precise means of imaging the airways for TBM. However, the current criteria for diagnosis of tracheomalacia of 50% airway collapse will need to be revisited given data from Boiselle and Limanovich group
References • Lee K, Sun M, Ernst A, et. al. Comparison of Dynamic Expiratory CT With Bronchoscopy for Diagnostic Airway Malacia. Chest 131, 2007. • Hunter HH, Stanford W, Grillo HC, Wiler JM. Collapse of the Trachea Presenting as Worsening Asthma. Chest 1993; 104: 633 -35 • Boiselle PM, O’Donnell CR, Baniker AA. et. al. Tracheal Collapsibility in Healthy Volunteers during Forced Expiration: Assesment with Multidetector CT. Radiology 2009; 252(1): 255 -262 • Litmanovich D, O’Donnell, Baniker AA. et. al. Bronchial Collapsability in Healthy Volunteers during Forced Expiration: Assesment with Multidetector CT. Radioligy 2010; 257(2): 560 -567 • Doshi J. Krawlec ME. JACI 2007; 120: 1276 -8