Disability Health Network Presentation Resource Resource Overview This

Disability Health Network: Presentation Resource

Resource Overview • This resource allows you to mix and match slides for your own presentations regarding disability, depending on your audience. • The slides are grouped into the following sections: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Disability Health Network Disability definitions and key messages WA Disability Health Framework Commitment to Inclusive Engagement Shared attitudes and behaviours in health care: a core capabilities resource for disability health Care Coordination Hospital Stay Guidelines Disability Liaison Officer Project Disability Access and Inclusion Plans Community of Practice National Disability Insurance Scheme • Please reference the Disability Health Network when using these slides.

Our purpose today… • X • Y • Z

Contacts and information Co-leads • Fiona Payne and Jenny Campbell Supported by • Health Networks Directorate and Department of Communities – Disability Services Email healthpolicy@health. wa. gov. au Phone 9222 0200 Find out more: join Health Networks! www. health. wa. gov. au/healthnetworks 4

5

Section 1: Disability Health Network

Disability Health Network aim The Disability Health Network aims to improve health outcomes for people living with disability by enabling consumers and carers, health professionals, hospitals, health services and the WA Department of Health to engage and collaborate effectively to facilitate health policy and increased coordination of care across the State.

Disability Health Network Establishment • Critical Incidents • Clinical Senate Debate 2011 • Disability Health Consultative Group 2012 • Department of Health and Department of Comminutes – Disability Services partnership • Disability Health Network launch 2012

What drives us United Nations Convention on the Rights of Persons with Disabilities Health disparities for people with disability National Disability Strategy 20102020 WA Disability Services Act 1993 Patient stories Clinical Senate recommendations

What we want to achieve • A better health experience for people with disability, their families and carers • Better health outcomes for people with disability by: – access to appropriate services – delivering health services that meet individual needs – coordinated care.

Making the aim a reality… • Co-leads • Executive Advisory Group Department of Communities – Disability Services • DAIP Community of Practice • Champions of change • Health Networks Directorate • Network members staff • WA health system and

Executive Advisory Group • Aboriginal health • • Aged care • • Disability service provider- • residential care • • Carers WA • • Consumer • • Dental Health Services • Local Area Coordination Mental health Primary care Nursing Allied health Paediatrics Medicine 5 Health Service Providers

How the Network operates • Collective wisdom • Overcome barriers • Key influencers • Systemic change • Shared vision • Multi level approach

The role of other networks • Share – raise awareness of the WA Disability Health Framework within their Networks • Connect – expressions of interest from those interested in working together • Improve – identify priority areas for measuring impact in practice

And so… We listen… We learn… We act… We connect… We share We influence… We partner…and We make a difference

Section 2: Disability definitions and key messages

Social Model of Disability 17

Impact of disability Disabilities can result in a person having a substantially reduced capacity for communication, social interaction, learning or mobility and a need for continuing support services in daily life. BUT, with the assistance of appropriate aids and services, the restrictions experienced by many people with a disability may be overcome.

Statistics Source: Australian Bureau of Statistics, Survey of Disability, Ageing and Carers 2012.
")
Health disparities Table 1: Disability health in Australia 15 -64 years (AIHW 2011 -12) Health condition/behaviour Severe/profound disability Typical adult population Diabetes 6% 2% Arthritis 21% 5% Osteoporosis 4% 1% 3/+ long term health conditions 74% 23% Mental health problems 50% 8% Psychological distress 22% 1% Childhood onset of mental health issues 8% 0. 2% Obesity 43% 25% Low exercise 46% 31%

Use of health services

Remembering Carers

Facts • ‘People with disability experience significantly poorer health than people without disability. ’ • ‘People with (disability) are 3. 3 times as likely as those without disability to have 3 or more long-term health conditions (74% versus 23%). ’ • ‘Half (50%) of people (with disability) had mental health conditions, compared with 8% for those without disability. ’ • People with disability use hospital services, both inpatient and emergency, more than the general population, and this increased rate of hospitalisation is exacerbated by lengths of stay up to six times the general population. • ‘There are multiple access barriers to appropriate health care for PWD. ’

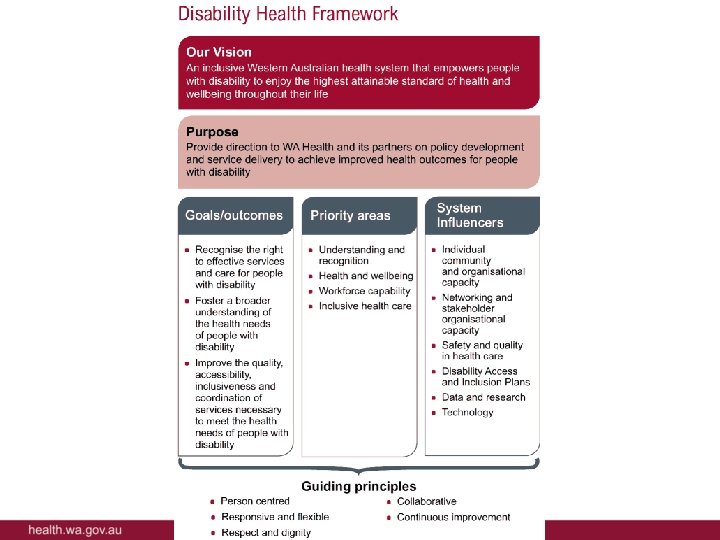
Section 3: WA Disability Health Framework 2015 -2020

Disability Health Framework Giving people with disability the best chance at their best health. • Values based with Guiding Principles • Social model of disability places the person at the centre of improvement initiatives • Underpinned by legislative obligations • Priorities provide a common focus for all stakeholders to share the responsibility • Opportunities for partnerships and collaboration through common enablers.

Making it real • Engagement Plan – July to December 2017 • Toolkit for Change • 2017 International Day of People with Disability • Champions of change

What we DON’T want…

Framework structure Purpose Provide direction to the WA health system and its partners on policy development and service delivery to achieve improved health outcomes for people with disability. Goals/outcomes Priority areas System influencers 29

Goals • Recognise the right to effective services and care for people with disability Rights • Foster a broader understanding of the health needs of people with a disability Needs • Improve the quality, accessibility, Access inclusiveness 30

Person Centred Continuous improvement Guiding Principles Collaborative Responsive and flexible Respect and Dignity 31

Priority Areas 1 2 3 4 • Understanding and recognition • Health and wellbeing • Workforce capability • Inclusive health care 32

Priority area 1: Understanding and recognition • Can be achieved by: – Improved awareness and understanding – A collaborative approach to health care for people with disability – Tailored evidence-based approaches 33

Priority area 2: Health and wellbeing • Can be achieved by: – Self management and empowering individuals – Effective communication – Timely access to health information and care 34

Priority area 3: Workforce capability • Can be achieved by: – Training and education for the health workforce – Collaboration in the workforce – Role of people with disability in workforce capability 35

Priority area 4: Inclusive health care • Can be achieved by: – Inclusive information and communication – Continuity of care across the continuum – Addressing barriers to access 36

Individual Community and organisational capacity Networking and engagement with stakeholders Disability Access and Inclusion Plans System influencers Safety and quality in health care Data and research Technology 37

Influencing the implementation of the WA Disability Health Framework System Manager Health Service providers Disability Sector Consumer Groups

What we learnt

Section 4: Commitment to Inclusive Engagement

Background

How the DHN has used the Commitment 42

How you can use the Commitment 43

Section 5: Shared attitudes and behaviours in health care: A core capabilities resource for disability health

What is the Resource? Support the best possible healthcare for individuals with disability Articulate expected attitudes and behaviours of the health care workforce Increase awareness of workforce requirements across the disability and health sectors Build on the capacity of the current health care workforce Improve continuity and collaboration across the range of health care settings Support development of new roles and functions Provide defined attitudes/ behaviours to inform development of future health care workforce. 45

Why we need the Resource • Framework Priority Area 3 – Workforce Capability • Clinical Senate recommendation 9: SHEF to direct the Do. H to develop a living with disability awareness and training program for all Do. H staff to change the service model to one of partnership with people with disabilities and their carers. 46

Key features • Social model of disability • Applicable across range of health care settings • Underpinned by guiding principles from the Framework • Six domains of common health care activity • Articulates values, knowledge, behaviour and skills that characterise quality health care • Extensive resources • Guided by: – Health Workforce Australia’s National Common Health Capability Resource: shared activities and behaviours in the Australian health workforce – National Mental Health Core Capabilities 47

Benefits The Resource supports: • Workers • Teams in services • Education and training providers/services • People using health services and the person/s providing support • Managers, planners and funders • Other sectors 48

Domains 1. Values 6. Life-long learning 5. Provision of care Sustainable, high quality, responsive services for all Western Australians 4. Collaborative and coordinated practice 2. Diversity and whole person focus 3. Professional, ethical and legal approach 49

Domain 6 – Life-long learning Graeme, Nurse: “I have just completed the new disability awareness online training. I was across most of the content but the personal stories made it real and reminded me to refocus. ” Suzie, teenager with Cerebral Palsy: “It’s a bit scary speaking to the medical students about providing health care for people with cerebral palsy…but then I remember they are only a few years older than me and probably just as scared as me. Who knows, I might be in their shoes one day!” 6. 1 Scope of practice, safety and accountability Values and attitudes Knowledge and understanding Skills and behaviours Resources Commitment to life-long learning. Individuals with disability have the right to best practice health care, delivered by competent workers. Self-reflection is a learning tool to improve individual practice and service delivery outcomes. Different methodologies and techniques to enhance learning. Contemporary practices in relevant disability health service. Engage in feedback processes and act as appropriate to improve competence. Identify and seek out personal and professional development needs. Use a variety of learning methodologies and techniques. Ensure training in the provision of health care to individuals with disability remains contemporary. Influence organisational learning and the development of strategies to support the workforce. United Nations Convention on the Rights of Persons with Disabilities 8 Australian Health Practitioner Regulation Agency. Australian Commission on Safety and Quality in Health Care: National Standards Professional and peer-reviewed journals, reports and websites Organisational standards and guidelines. 50

Section 6: Care Coordination

What is care co-ordination? Consistent systems and processes across the continuum of care, including: Effective care transition In- and outpatient care Holistic perspective Self/carer manageme nt Community/ residential care Communication Primary care

Issues • Difficulty navigating systems and coordinating services/supports across health, disability, primary health and mental health • Lack of connectivity between systems • Result: – Poorer health outcomes for people with disability – Increased costs (staff, tests, equipment, opportunity) – Time delays

Why care co-ordination is important • ‘Co-ordination of care is important for the increasing numbers of people, often aged or with chronic conditions, who require complex care from an often fragmented and highly specialised health system. ’ • ‘…strategies that involved providing systems and structures to support coordination were the most successful in achieving significant health outcomes, and those that involved communication and individual support were most successful in achieving patient satisfaction…’ • Significant benefit for health through reduced length of stay and reduction in avoidable hospital admissions

Work to date • DHN Care Co-ordination Working Group – Care Coordination Framework Project Group – Hospital Stay Guidelines Project Group • Explore current understanding/delivery of care coordination to people with disability in WA – Survey of providers of health and support services – Consumer/carer focus groups

Ongoing work • Hospital Stay Guidelines • Developmental Pathways Group of DGs – Using linked data to reduce Costs and Improve Health Outcomes

Rare Diseases Research • People living with rare diseases are likely to have multi -systemic dysfunction and require complex health care and access to a wide range of health services across tertiary, secondary and primary sectors • Focus groups across WA • Participants were mainly coordinating their own care (or their child’s care), including medical care • Described as “exhausting” & “all consuming” • Strong need for support with care coordination • Survey of healthcare experiences of Australian adults living with rare diseases

Section 7: Hospital Stay Guidelines

About the Hospital Stay Guidelines • Best practice approach for disability service organisations and hospitals when managing the hospital experience of individuals with disability • Better engagement and planning when an individual with disability is: 59

Applicability • Primarily targeted to towards hospitals and disability service organisations providing supported accommodation • Also applicable to individuals, carers and families
 2. Planned admission to")
How to use the Guideline 1. Emergency Department admission (flowchart) 2. Planned admission to ward (flowchart) 3. Hospital stay 4. Discharge from hospital 61

Going to the emergency department • Transport to emergency department • At the emergency department • Triage • Post-triage • Case conference • Transport back from the emergency department

Planned admission • Admission via regular GP • Admission via specialist • Pre admission clinic

Admission into hospital • Planning and preparation for admission to hospital • Providing equipment • Period of admission

Being discharged from hospital • Planning discharge • Consideration for successful discharge • Proposed long term accommodation options

Section 8: Disability Liaison Project

About the DLO Project • 2011 Clinical Senate debate: Clinician – do you see me? The Department of Health introduces Disability Liaison Officers in all adult tertiary/secondary health services. • 3 phases from April 2013 to June 2016 over North and South Metropolitan Health Services • Sites included Armadale, Fiona Stanley and Sir Charles Gairdner Hospitals.

Key findings • Dedicated DLO position not most sustainable/effective option • Embed system and process change through existing infrastructure e. g. Disability Access and Inclusion Plans, site processes • Summary report 68

Phase 1 • Extensive consultation to describe hospital experience of people with disability • Key issues raised: – No central point of patient information – Disability profile – Service integration – Resource limitations – Disability education and training. – Disability service delivery models. 69

Phase 1 recommendations NMHS • Implement DLO pilot position at Sir Charles Gardiner Hospital within inpatient complex care team SMHS • Implement DLO pilot position at Armadale Health Service • Linkages to Co. Ne. CT and DLO Steering Group 70

Phase 2 NMHS • Pilot various approaches to address service needs – Screening tools e. g. “disability checklist” – Admissions and discharge planning – Staff education sessions SMHS • Patient journey study • Focus on disability forum • Resource directory development 71

Phase 2 recommendations NMHS and SMHS • Focus on embedding disability screen processes • Enable sustainable changes • Improve processes for people with disability at hospital and service provider level • Project team did not find sufficient evidence for a standalone Disability Liaison Officer position 72

Phase 3 NMHS • Early identification of complex needs • Internal and external engagement • Education and training resources including elearning package SMHS • Patient journey study • Process mapping workshops • Survey of Fiona Stanley Hospital staff for DAIP input 73

Resources developed • Hospital posters • NMHS e-learning • Education presentation

Section 9: Disability Access and Inclusion Plans Community of Practice

About the DAIP Co. P • Representatives from Health Service Providers and Department of Communities – Disability Services • Convened by the DHN to be a self sustaining group • Aim to work collaboratively to share knowledge and expertise to develop system wide approach to DAIPs 76
 • HSP representatives DAIP")
Membership • Co-leads and staff of the DHN (Interim measure) • HSP representatives DAIP area and site leads (North, South, East, WACHS and Child and Adolescent) • Do. H member who is responsible for the DAIPs within Royal Street (System Manager) • Department of Communities – Disability Services DAIP officers • Carer representation 77

Section 10: National Disability Insurance Scheme
 • Human Rights • Economic & Social Reform")
The National Disability Insurance Scheme (NDIS) • Human Rights • Economic & Social Reform • NDIA Strategic Plan • Pillars – Choice and Control – Insurance Based Approach – Community and Mainstream • Insurance Principles – Actuarial analysis – Lifetime focus – Research and innovation – Community focus

Key resources • NDIS home page • NDIS in Western Australia • Department of Communities – Disability Services: WA NDIS information hub 80
- Slides: 80