DIFFERENTIAL DIAGNOSIS OF CHEST PAIN Prof Dr Muzaffer













")




 Afferent nerves to the same")





- Slides: 26
DIFFERENTIAL DIAGNOSIS OF CHEST PAIN Prof. Dr. Muzaffer Degertekin Kardiyoloji ABD
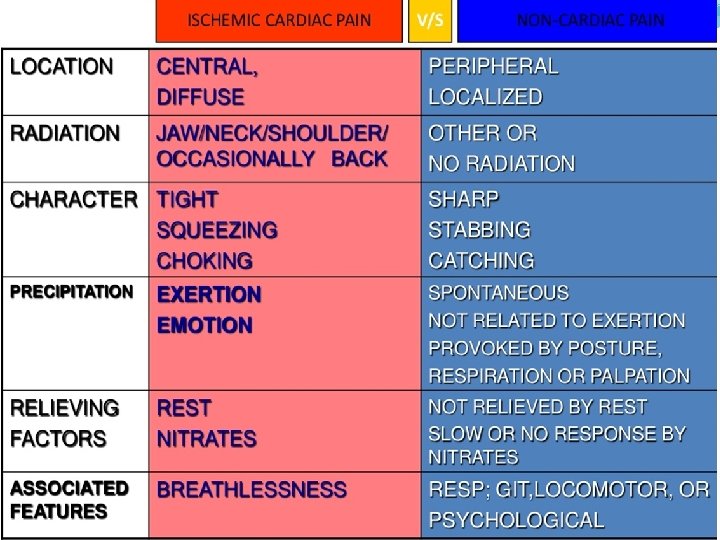
The differential diagnosis of patients presenting with chest pain is extensive, ranging from benign musculoskeletal etiologies to life-threatening cardiac disease.
CHEST WALL PAIN �Musculoskeletal pain �Isolated musculoskeletal chest pain syndromes (costosternal, posterior chest wall syndromes) �Rheumatic diseases �Non-rheumatic systemic diseases �Costochondritis �Chest wall pain occurring after CABG �Costovertebral joint dysfunction syndrome �Thoracic disk herniation �Sternalis syndrome, xiphoidalgia, and spontaneous sternoclavicular subluxation
�Rheumatic diseases �Involvement of thoracic joints in rheumatic diseases can be associated with musculoskeletal chest wall pain �rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and fibromyalgia �Non-rheumatic systemic diseases �stress fractures due to coughing, neoplasms including pathologic fractures, infections such as septic arthritis and osteomyelitis, and sickle cell anemia �Skin and sensory nerves �herpes zoster
CARDIOVASCULAR CAUSES OF CHEST PAIN �Ischemic chest pain syndromes �Coronary artery disease �Other ischemic chest pain conditions �Coronary vasospasm �Cardiac syndrome X: angina-like chest pain associated with normal coronary arteries; most commonly seen in premenopausal women �Valvular heart disease: Aortic stenosis �Congenital anatomic anomalies of the coronary arteries, spontaneous coronary artery dissection
Nonischemic cardiac chest pain syndromes �Pericarditis: � pleuritic in quality, pericardial friction rub � sudden onset and occurs over the anterior chest. � usually sharp and exacerbated by inspiration � may decrease in intensity when the patient sits up and can radiate, especially to the trapezius ridge. �Myocarditis: � chest pain is usually associated with concomitant pericarditis �Acute aortic syndromes : acute aortic dissection, intramural aortic hematoma, and penetrating aortic ulcer.
Aortic dissection �Pain typically is cataclysmic in onset �Intense, acute, searing, throbbing, or migratory �Radiate to the anterior chest, jaw, back, or abdomen depending on which segment of aorta is involved �Most common in men older than age 60 �Hypertension is the most important risk factor �Marfan's syndrome, congenital bicuspid and unicommissural aortic valves, aortic coarctation �Preexisting aortic aneurysm (due to vasculitic conditions such as giant cell arteritis, Takayasu arteritis, and others) and pregnancy
CHEST PAIN DUE TO HYPERADRENERGIC STATES �Catecholamines have various physiological actions in peripheral circulation (stimulation of heart rate and vasoconstriction) �Cocaine and amphetamine intoxication and pheochromocytoma may cause chest pain due to either increased demand or decreased delivery of oxygen �Tachycardia, hypertension, and evidence of vasospasm may be seen
GASTROINTESTINAL CAUSES OF CHEST PAIN �Esophageal hypersensitivity �Abnormal motility patterns and achalasia �Esophageal rupture, perforation, and foreign bodies �Other causes of esophagitis: medications, infectious causes
PULMONARY CAUSES OF CHEST PAIN �Acute pulmonary embolism �Pulmonary hypertension and cor pulmonale �Pneumonia �Cancer �Sarcoidosis �Asthma and COPD
Pleura and pleural space �Pneumothorax �Pleuritis �MEDIASTINAL CAUSES �PSYCHOGENIC/PSYCHOSOMATIC CAUSES
DIFFERENTIAL DIAGNOSIS Causes of life threatening chest pain �Acute coronary syndrome �Aortic dissection �Pulmonary embolism �Tension pneumothorax �Pericardial tamponade �Mediastinitis (eg, Esophageal rupture)
PATHOPHYSIOLOGY OF ANGINA �Angina is caused by myocardial ischemia, which occurs whenever myocardial oxygen demand exceeds oxygen supply.
Myocardial oxygen demand Heart rate � Systolic blood pressure (the clinical marker of afterload) afterload � Myocardial wall tension or stress (the product of ventricular end-diastolic volume or preload and preload myocardial muscle mass) � Myocardial contractility �
Myocardial oxygen supply �Coronary artery diameter and resistance �Collateral blood flow �Perfusion pressure �Heart rate
ETIOLOGY �Coronary atherosclerosis �Coronary artery vasospasm �Coronary artery fibrosis �Coronary artery embolism �Coronary artery dissection �Coronary arteritis
QUALITY �Angina is usually characterized more as a discomfort rather than pain, and may be difficult to describe. �Squeezing, tightness, pressure, constriction, strangling, burning, heart burn, fullness in the chest, band-like sensation, knot in the center of the chest, lump in throat, ache, heavy weight on chest (elephant sitting on chest), like a bra too tight, and toothache
QUALITY �Typically gradual in onset and offset, with the intensity of the discomfort increasing and decreasing over several minutes �Angina is a constant discomfort that does not change with respiration or position
Location and radiation �Corresponding dermatomes (C 7 -T 4) Afferent nerves to the same segments of the spinal cord as the heart �Upper abdomen (epigastric) �Shoulders, arms (upper and forearm) �Wrist, fingers �Neck and throat �Lower jaw and teeth �Back (specifically the interscapular region) Radiation to both arms is a strong predictor of acute myocardial infarction
Provoking factors �Activities and situations that increase myocardial oxygen demand �Physical activity �Cold �Emotional stress �Sexual intercourse �Meals �Cocaine use
Timing �More commonly in the morning due to a diurnal increase in sympathetic tone �Enhanced sympathetic activity raises heart rate, blood pressure, vessel tone and resistance �Increased platelet aggregability
Duration and relief �Angina generally lasts for two to five minutes �It is not a fleeting discomfort, which lasts only for a few seconds or less than a minute �Generally does not last for 20 to 30 minutes, unless the patient is experiencing an acute coronary syndrome, especially myocardial infarction
Associated symptoms �Angina is often associated with other symptoms. �shortness of breath, which may reflect mild pulmonary congestion �Belching, nausea, indigestion, diaphoresis, dizziness, lightheadedness, clamminess, and fatigue.
Noncardiac chest pain �Pleuritic pain, sharp or knife-like pain related to respiratory movements or cough �Primary or sole location in the mid or lower abdominal region �Any discomfort localized with one finger �Any discomfort reproduced by movement or palpation �Constant pain lasting for days �Fleeting pains lasting for a few seconds or less �Pain radiating into the lower extremities or above the mandible