DIFFERENTIAL DIAGNOSIS AND TREATMENT OF EDEMATOUS SYNDROME Associate








 hormones (corticosteroids, female sex hormones, estrogen, progesterone,")
. The overload")
.")


: I-class patients with heart disease,")






, which can cause a")









 - Skin is")




. - Mainly develop between 10")












- Slides: 57
DIFFERENTIAL DIAGNOSIS AND TREATMENT OF EDEMATOUS SYNDROME. Associate professor Rakhimov M. E.
swelling of the excessive accumulation of fluid in body tissues and serous cavities. increased tissue volume and body weight. capacity decrease of serous cavities disorders of the swollen tissues and organs.
Peripheral edema are recognized by the increase in the volume of a limb or part of the body, swelling of the skin and subcutaneous tissue, reducing their elasticity. On palpation there is a doughy consistency of the skin, after pressing a finger on her left fossa. If, after pressing a finger on the edematous skin is left fossa, the swelling can be attributed to false.
Increased hydrostatic pressure in the capillaries. Increased permeability of the capillaries Increased interstitial fluid oncotic pressure. The main factors leading to the violation of the local water balance Reduced tissue mechanical pressure. Reduced oncotic pressure of the blood plasma. Violation of lymph drainage
Swelling common or widespread edema, testifying to an abuse of water-salt metabolism in the body as a whole local or localized swelling that occurs as a result of fluid retention in a limited area of the body
The main causes of edema syndrome heart disease kidney disease General swelling liver disease Gipoproteinemi cheskie swelling diopathic edema
Venous edema: 1. Acute deep vein thrombosis, 2. Chronic venous insufficiency, 3. venous obstruction Lymph edema: 1. Idiopathic: a) birth b) early. 2. Inflammatory. 3. Obstructive. local swelling Fatty swelling. Other types of edema
D. Other types of edema: swelling 1. Ortostaticheskie 2. Arterio-venous edema 3. Oteki after vascular surgery, 4. Swelling caused by lesions of the musculoskeletal system: a) muscle pathology, and b) an inflammation of the tendon sheath, and c) fracture, 5. Reflex Sympathetic distrofiya. 6. Edema in patients with lesions of the nervous system, 7. Allergic 8. Hereditary angioedema otek. 9. Premenstrual swelling;
III. Edema caused by taking drugs: a) hormones (corticosteroids, female sex hormones, estrogen, progesterone, testosterone). B) antihypertensive drugs (Rauwolfia alkaloids apressin, methyldopa, β-blockers, clonidine, minoxidil, Calcium blockers tubules). In ) antiinflammatory drugs (phenylbutazone, naproxen, ibuprofen, indomethacin). g) other drugs (antidepressants midantana). IV. Pseudoedema 1. Myxedema 2. Systemic scleroderma. 3. Dermatomyositis.
The defeat of the myocardium (myocarditis, dilated cardiomyopathy, myocardial, ischemic heart disease). The overload of the heart muscle (aortic or mitral regurgitation, ventricular septal defect, patent ductus arteriosus). Causes of cardiac edema. The overload of the heart muscle pressure (hypertension, aortic stenosis, narrowing of the mouth of the pulmonary artery). Systemic and pulmonary hypertension.
Overloading infarction combined (combination of the above reasons, complex congenital and acquired heart defects). Causes of cardiac edema The state with the highest cardiac output (hyperthyroidism, severe anemia, massive obesity, cirrhosis of the liver). Violation of diastolic ventricular filling: hypertrophic and restrictive cardiomyopathy, hypertensive heart disease (in the absence of dilatation of the left ventricle), isolated mitral stenosis, constrictive pericarditis and pericardial).
Classification by HNK ND Strazhesko and VH Vasilenko: 1. Phase I - Initial: The Hidden Tax manifested dyspnea, palpitations, fatigue only during exercise. At rest, hemodynamics not narushena. 2. Stage II A: Signs Tax alone expressed moderately, exercise tolerance is reduced, there are violations in a large or small circle of blood, asthma attacks, radiographic, in some cases, ECG signs of secondary pulmonary hypertension, peripheral edema, and observed a moderate increase in liver size.
Stage II B: The salient features of the HNK alone, severe hemodynamic abnormalities in the large and in the pulmonary circulation. Stage III - Terminal: with little movement or even alone severe hemodynamic, metabolic, irreversible degenerative changes in organs and tissues.
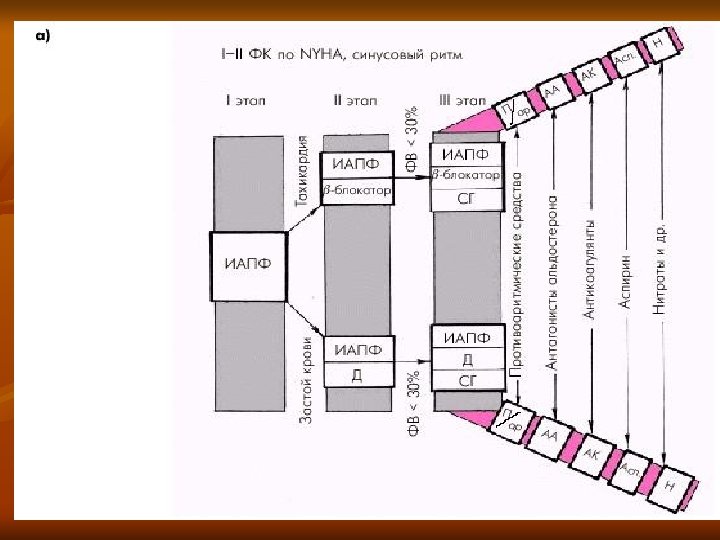
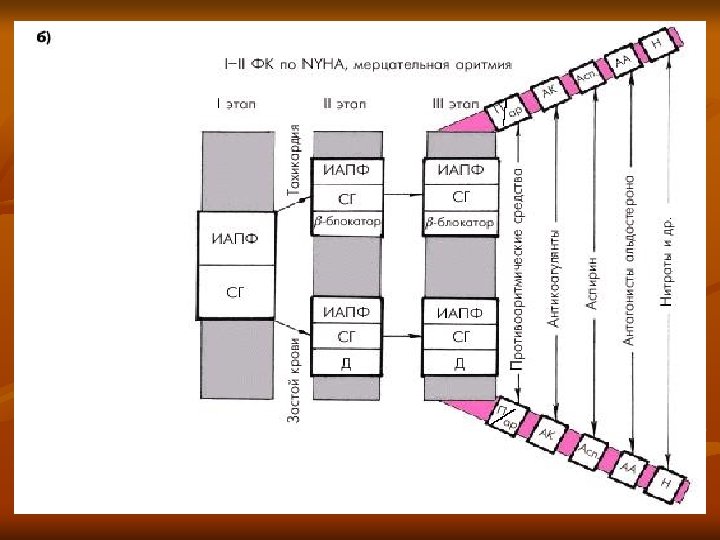
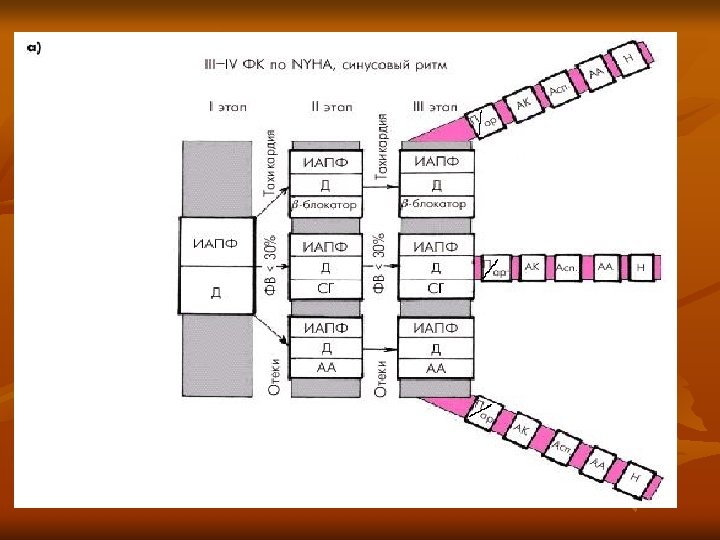
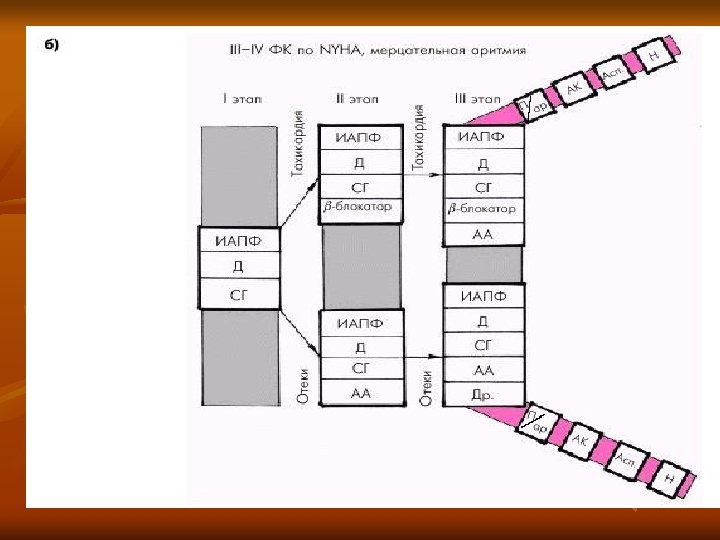
HNK classification of the New York Heart Association (NYHA): I-class patients with heart disease, but without limitation of physical activity. Asymptomatic left ventricular dysfunction II-Class - Patients with diseases of the heart, causing a slight limitation of physical activity. Light hearted nedostatochnost III Class - Patients with diseases of the heart, causing a significant reduction in physical activity. Moderate heart failure tyazhesti. IV Class - Patients with heart disease who perform even minimal physical activity causes discomfort. Severe heart failure
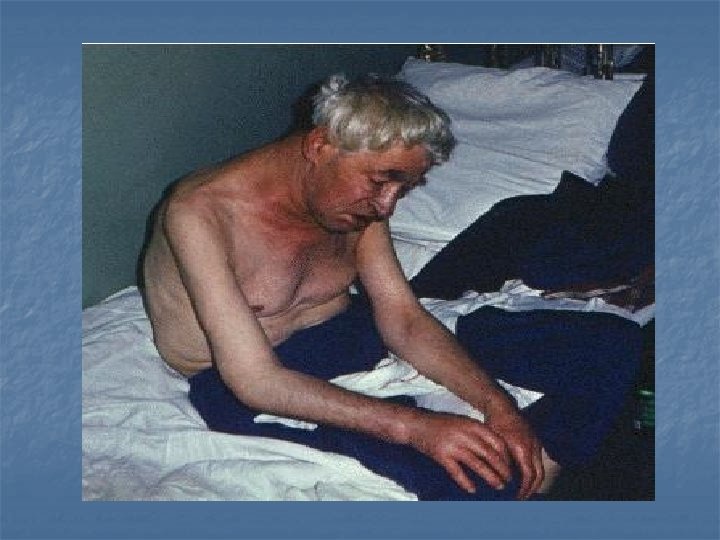
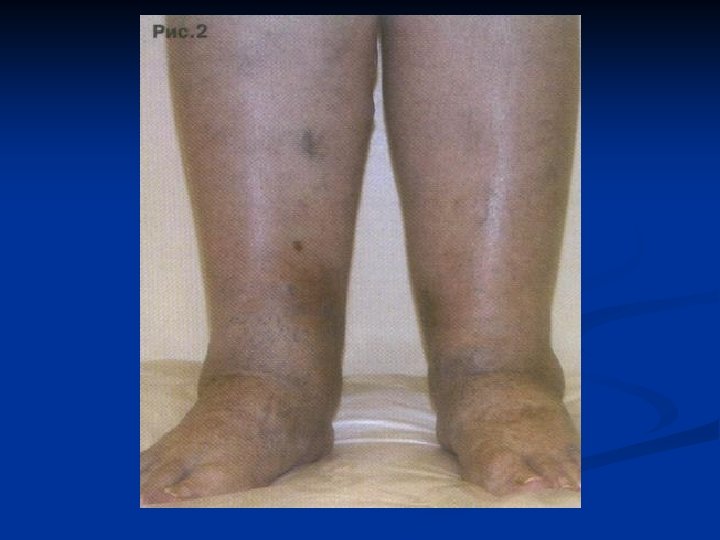
When HNK edema: - develops gradually localized symmetrically - Mostly in the feet and legs. - In bedridden patients edema appear on the back, in the sacrum. - The material is cold to the touch, cyanotic, the elasticity of its reduced during prolonged edema observed trophic changes. - Swelling usually moderately dense, leave a hole when pressed with your finger, move with changes in body position. - The development of edema is usually preceded by a more or less prolonged period of breathlessness. - Often, swelling of the skin and subcutaneous tissue is accompanied by ascites, hydrothorax (predominantly right -sided). - There is jugular venous distention, shortness of breath, enlargement of the liver.
Cardiac tamponade in exudative pericarditis usually develops during tumor, uremic and idiopathic pericarditis. Physical examination: hepatomegaly, ascites (perekarditichesky psevdotsirroz Peak), prevailing over peripheral edema, and in addition: - Swelling of the neck veins, often growing on inspiration (Kussmaul's sign) - The paradoxical pulse - There is growing pale skin with severe cyanosis of the lips, nose and ears. - Swelling of the face and neck is expressed to a greater extent than in heart failure - "consular" head, "Stokes collar. “ - Sometimes also developed swelling shoulder and arm.
Clinic of constrictive pericarditis is characterized by a triad of Beck: high venous pressure, ascites, "small quiet heart. " Clearly visible large veins throbbing, their diastolic collapse. Similar clinical picture has constrictive cardiomyopathy in amyloidosis, sarkaidoze, hemochromatosis.
Edema occurring in diseases of the kidney -formation of edema associated with reduced urine output (daily amount of urine of 500 ml or less. ) - Body weight increased in a short time. - Swelling appear in the morning and go throughout the day. - Swelling of the subcutaneous tissue is initially limited, local, in the following (sometimes rapidly) takes the common nature of the edema (anasarca). - Typically start swelling from the face (around the eyes, eyelids, cheeks, etc. ) and distribute it to the trunk and limbs. - Observed accumulation of fluid in the cavities, often ascites and pleural effusion is rare.
-Often occurs swelling of internal organs (heart, liver, lungs, brain), which can cause a clinical picture depending on the location. - Characterized by rapid appearance of edema and also fairly rapid disappearance. - Hydropic pale skin, normal temperature. - Consistency swelling soft, doughy. - For large swelling are signs degeneration of skin and its appendages: dry, sometimes shiny, atrophic, epidermal peeling, brittle, dull hair and nails. - Swelling quickly shifted when changing body positions. - Leave the hole when pressed with your finger that quickly returns to its original position. - In most cases, dyspnea, usually does not occur. The liver is not increased.
- When hydrops may stretch of subcutaneous fat in the limbs to form a swollen blisters, detachments of the epidermis, the skin tears streaming edema fluid (erysipelas, cellulitis. ) - When urinalysis reveals proteinuria, hematuria, and pyuria cylindruria. When testing of blood observed anemia, hypoproteinemia, Dysproteinemia, hypercholesterolemia, increased erythrocyte sedimentation rate, the level of urea, creatinine, increased fibrinogen, Ig. M, antistreptolysin-O titer, CRP, α - and γglobulin, reduced Ig. G content, etc.
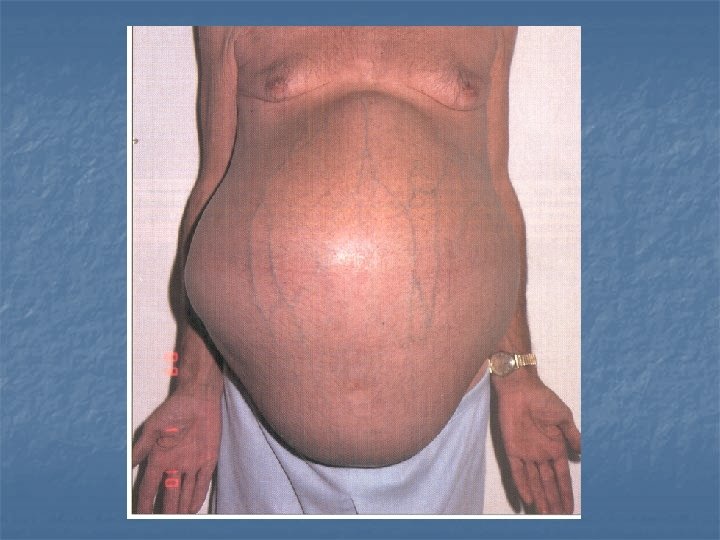
Swelling of hepatic origin. - History reveals virus hepatitis, alcoholism, toxic - No overt signs of violation of the heart and kidneys Identify symptoms of chronic liver disease (cirrhosis), arterial spider hemangioma, liver palm (erythema), gynecomastia and developed venous collaterals in the abdominal wall; - Swelling localized mainly in the abdominal cavity with the formation of ascites. - Swelling in the legs joined by relatively rarely - occur without clinical signs for a small amount of liquid;
-With increasing amounts of liquid are observed abdominal distension, discomfort, anorexia, nausea, heartburn, pain in the right upper quadrant, respiratory disorders. Puffiness or bulging sides of abdomen - Symptom geoidal or "splashing" on auscultation - Shortening the percussion sound in the side of the abdomen with a change of position of the patient or the appearance of dullness in the center of the abdomen with the knee-elbow position the patient. - Ascites may be associated with swelling of the vulva, umbilical or inguinal hernia, pleural effusion, most righthanded. In the blood, change in the amount of bilirubin, enzymes.
Enteropathy with increased loss belka. Pervichnaya exudative enteropathy characterized by increased protein loss through the ectatic lymphatic vessels of the mucous membrane of the small intestine. The main clinical manifestations: - expressed massive gipoproteinemicheskie often asymmetrical edema - swelling appear on the legs, arms, face, lower back - sometimes anasarca - Pretty quickly develop ascites and pleural effusion - Diarrhea appears to edema, often at the same time with them.
- Chair without mucus, blood - Patients concerned about abdominal pain, polifekaliya, persistent bloating, rumbling, increased flatulence, In secondary exudative enteropathy leading signs - increasing protein deficiency with a significant decrease in body weight, edema - ascites syndrome, degenerative changes in all organs and body systems.
Allergic edema. - Allergic edema appear in the form of so-called angioedema, sometimes together with hives and other allergic diseases (asthma, vasomotor rhinitis, hay fever). - Urticaria and Angioedema more common in girls. - A few minutes after exposure to the allergen on the skin of the patient appears erythema, urticaria occur then, much itchy elements.
- Skin eruptions are very diverse, ranging nodules, blisters of various sizes and shapes. - In reaction to food before the typical rash patient feels tingling tongue, lips, palate, swelling in these places, often a sharp pain in his stomach. Can be perioral and perianal dermatitis. - A new observation conjunctivitis, rarely difficulty in breathing due to edema of the larynx. Occasionally, patients develop vomiting, collapse, anaphylaxis.
Inflammatory edema are local, such as around the boil, carbuncle, cellulitis and other purulent lesions. Mechanism of their formation is associated with propotevanie fluid from the blood vessels into the area of inflammation, which accumulate in large amounts of hydrogen ions. A distinctive feature of the inflammatory edema is flushing of the skin, pain at rest or on palpation, increased local temperature. They usually develop on one leg or arm. Not accompanied by changes in urine, except for a small transient proteinuria (in the form of traces) as a result of high fever and intoxication.
Myxedema - Characteristic of the expressed primary or secondary hypothyroidism due to a lack of thyroid hormones in the body. - This leads to increased tissue gipofilnosti that swell more than normal. - Characteristic: drowsiness, lethargy, loss of memory, slow speech, movements, fatigue, decreased performance, arthralgia. - Swelling of the face and extremities, pits on pressure remains
The nature of edema fluid like mucus (mucosal edema, myxedema. ) - Skin is dry and pale, with a yellowish tinge. - The friability and loss of hair on the head, the lateral third of the eyebrows. - Language thickened around the edges - impressions of the teeth. - Hoarseness. - Reduction in body temperature. - Bradycardia, deafness heart tones, sometimes a normal heart rate, tachycardia rarely. - The tendency to hypotension in 10 -20% of patients with hypertension, which is usually reduced or eliminated during therapy with thyroid medications. - Often develops hypochromic and IDA. - Some patients may develop laktoreya and amenorrhea.
The causes of edema of the lower extremities: - Acute deep vein thrombosis. - Chronic venous insufficiency. - Lymphedema. - Chronic arterial insufficiency. - Lack of blood circulation. - Pathology of the liver. - Osteoarticular pathology (deforming osteoarthritis, reactive polyarthritis) - idiopathic orthostatic edema. .
Venous edema, associated with acute and chronic thrombosis of the deep veins of the extremities. - One-sided defeat. - The swelling appears suddenly, often against a background of health. - For acute thrombosis typical pain on palpation of the swelling with the advent of the pit on pressure. -Swelling covers both tibia and femur. - In the early days of wearing the growing nature of the edema, accompanied by arching pain in extremity, It flows with increased venous pattern on the thigh and groin area. - After a few weeks of swelling umenshaetsya but does not disappear almost never.
Chronic venous insufficiency is developing varicose -postthrombophlebitic or diseases of the lower extremities. - Mandatory sign-nodular transformation of the presence of the superficial veins, usually bilateral disease. - In terms of venous stasis is the difficulty of reabsorption and consequently an increase in interstitial fluid. - Excess fluid is removed from the tissue lymphatic capillaries. - At some point in the disease course, this equilibrium is disturbed, reserve capacity of the lymphatic system is not enough. Then, and edema.
- He appears in the second half of the day, towards evening, localized in okololodyzhechnoy zone and the lower third of the leg. - By the end of the day discomfort when using their preferred shoe ("reduction" in size). Most patients notice the appearance of a trace of socks ("symptom of socks"). - Swelling is transitory in nature, ie completely disappears after a night's rest. - An additional criterion is the presence of trophic disorders of the surface tissues (hyperpigmentation, lipodermatosclerosis, trophic ulcers), which never occur in acute venous thrombosis
Lymph edema, may be congenital in nature (primary lymphedema). - Mainly develop between 10 -40 years. - Swelling looks one-sided. - First, there is usually transient edema, which appears in the second half of the day on the foot and lower leg. - Then, in the later stages of the swelling becomes permanent and can cover the entire limb. - Characterized by swelling of the foot cushion. - Varicose veins are rare. - Lymph edema more stable and slower to regress when we picked up the limb. - They are characterized by a thickening and swelling of the skin change the type of "peel appelsina" painful on palpation.
Edema encountered in osteoarticular diseases: - It is almost always local and occurs in the area of the affected joint in the acute period of the disease, combined with the severe pain and limitation of motion in the affected joint. After a course of treatment of edema disappears, although the longterm course and frequent exacerbations deformation of the surrounding tissues ("psevdootek") becomes a constant.
Lipedema - The etiology is not known. - You can talk about the inherited defect in the subcutaneous tissue. - Lipedemu detected only in women. A similar pattern can also be seen in their relatives on the downlink and the uplink. - Characteristic symmetrical increase in subcutaneous fat in the legs only. - The volume and shape of the hips and feet remain unchanged. - Do not show signs of chronic venous insufficiency. - Wears orthostatic character. - There is a growing before menstruation, prolonged sitting, bathing in the warm water, uncontrolled use of salt. - Palpation of the lower leg is often painful.
The tactics of a general practitioner in the edematous -ascitic syndrome is necessary to establish the correct and mutually trusting relationship with the patient. - Conduct a detailed analysis of complaints, medical history and physical examination data. - Put the correct diagnosis by examination. - Recommend plan for inspection and necessary treatment. - If necessary send to a specialized hospital.
Diagnostic studies in patients with otekami 1. A minimum of laboratory and instrumental investigations: Complete blood and urine total protein and protein fractions of blood, blood electrolytes, ECG, X-ray of the chest. 2. If necessary, we provide additional laboratory and instrumental investigations: serum protein electrophoresis, liver function tests, Determination of T 4 and T 3 in the blood serum
- Ultrasound - Chest X-ray - Echocardiography - CT scan and chest - Radionuclide Angiography - Doppler examination of the vessels - phlebography - CT of the abdomen - lymphangiography - biopsy
In the treatment of edema syndrome is necessary to observe the following plan: 1. Treatment of the underlying disease. 2. Rational order of treatment for patients Making optimum physical and psychological environment at home and at work. 3. Clinical nutrition: Diet - a full, quickly digestible, rich in proteins, vitamins and potassium. At high fluid retention and hypertension limited amount of salt and water.
Treatment of renal edema. - Corticosteroids, cytostatics, pulse therapy, plasmapheresis, hemosorbtion - Symptomatic treatment with ACE inhibitors, diuretics (hydrochlorothiazide, furosemide, Uregei) - Stroke In nephrotic to prevent the development of hypovolemia and to restore circulating blood (w / in reopoligljukin, dextrans, gemodez, protein solutions).
Treatment of hepatic edema. - Diuretics: spironolactone, furosemide -protein preparations - fresh frozen plasma, albumin - Abdominal paracentesis - Astsitosorbtsiya - Ultrafiltration of blood - Surgical treatment.
Gipoproteinemicheskoy treatment of exudative enteropathy -reduction protein loss - Eliminating diarrhea - treatment of dysbiosis and the syndrome of inadequate intake - Correction of metabolic disorders - Protein hydrolysates, anabolic hormones, calcium supplements, iron, vitamins - If necessary, antibiotics, corticosteroids - and thiazide Potassium -sparing diuretics.