Different ways to reduce the incidence of laryngospasm




























- Slides: 30
Different ways to reduce the incidence of laryngospasm in children after Tonsillectomy and Adenoidectomy 麻醉科R 1楊美惠 指導醫師 劉漢平 醫師
Laryngospasm n n May induced by blood or secretion accumulated around pharyhx or any kind of stimulation during emergence It is particularly frequent in children after upper airwy surgery(e. g. adenotonsillectomy) ~about 21 -24% Laryngospasm is essentially a protective reflex which acts to prevent foreign material entering the tracheaobronchial tree. This glottic reflex to inspiration and expiration causes hypercarbia and hypoxia and may be life-threatening.
Current methods n n Deep versus awake extubation IV or aerosolized lidocaine IV magnesium “No Touch” extubation
Emergence airway complications in children: a comparison of tracheal extubation in awake and deeply anesthetized patients. Anesth Analg Patel RI, Hannallah RS, Norden J, et al. 1991; 73: 266 -70 n n Patients: 70 children undergoing either elective strabismus surgery or adenoidectomy and/or tonsillectomy. Methods: Awake extubation group: Extubation at end-tidal halothane concentrations of less than 0. 15% Deep extubation group: end-tidal halothane concentrations of greater than 0. 8%
n n Results: At 1, 2, 3, and 5 min after extubation, patients extubated deep had significantly higher oxyhemoglobin saturations than patients extubated awake (Sp. O 2 97. 6% +/- 3. 7% to 99. 8% +/- 0. 5% vs 93. 7% +/- 4. 8% to 98. 6% +/- 2. 5%). Oxygen saturation values were similar thereafter. The incidence of postoperative laryngospasm, excessive coughing, breath holding, airway obstruction requiring positive pressure ventilation after extubation, or arrhythmias was not statistically different between patients extubated awake or deep.
n These investigators concluded that for healthy children undergoing elective surgery, clinical conditions or the preference of the anesthesiologist should dictate the choice of extubation technique.
Deep extubation Advantages Disadvantages Less likely to cough and strain afterward, thus avoiding the likelihood of laryngospasm and oxygen desaturation. Risk of aspiration and inadequate airway protection.
Lidocaine via IV route n Baraka A. Intravenous lidocaine controls extubation laryngospasm in children. Anesth Analg 1978; 57: 506 -7. n n Study group : receiving an IV bolus of 2 mg/kg of lidocaine 1 min prior to extubation Control group: receiving no lidocaine before extubation Results: Study group: no one developed laryngospasm Control group: 4 of 20(20%) patients had severe laryngospasm after extubation.
Does intravenous lidocaine prevent laryngospasm after extubation in children? Leicht P, Wisborg T, Chraemmer-Jorgensen B. Anesth Analg 1985; 64: 1193 -6. n n n The incidence of laryngospasm was the same between lidocaine and saline groups. They concluded that their results differed from Baraka's because of differences in the time interval time (4. 5 vs 0. 5 to 1. 5 min) between lidocaine administration and extubation, and that the central effect of lidocaine had already dissipated(消散、消失) in the children they evaluated. The duration of action of lidocaine is such that it should be administered 60 -90 s prior to tracheal stimulation or extubation.
Lidocaine via aerosolized form n n Dain DS, Boushey HA, Gold WM. Inhibition of respiratory reflexes by local anesthetic aerosols in dogs and rabbits. J Appl Physiol 1975; 38: 1045 -50. Cross BA, Guz A, Jain SK, et al. The effect of anaesthesia of the airway in dog and man: a study of respiratory reflexes, sensations and lung mechanics. Clin Sci Mol Med 1976; 50: 439 -54. Common conclusions: the inhalation of nebulized 20% lidocaine or 5% bupivacaine has been shown to abolish(廢除、 廢止) the cough reflex in animals Cross et al. found that inhaled aerosolized bupivacaine significantly suppressed coughing triggered by inhaled citric acid or tactile stimulation of the trachea with a suction catheter via tracheotomy stomas.
n Local anesthetics, administered either systemically or as aerosols, can also attenuate bronchospasm by directly relaxing airway smooth muscle, inhibiting mediator release, and/or interrupting reflex arcs
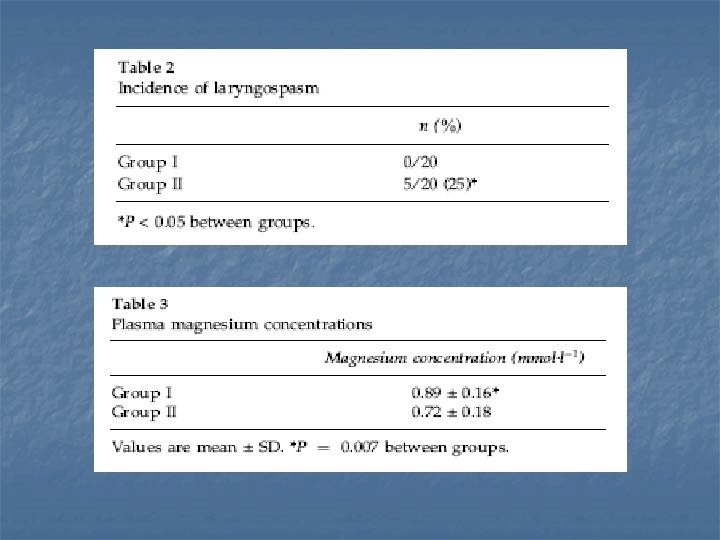
The use of magnesium to prevent laryngospasm after tonsillectomy and adenoidectomy: a preliminary study Gulhas N, Durmus M, Demirbilek S, et al Paediatr Anasth 2003; 13: 43 -7
Methods n n 40 patients, ASA I-II, aged 3 -12 years were scheduled for tonsillectomy or/and adenoidectomy, in a double-blind randomized, prospective manner. Anesthesia course: Induction with sevoflurane Pre-intubation medication: Lidocaine 1 ml/kg, Alfentanil 10 ug/kg, Vecronium 0. 1 mg/kg Maintenance: sevoflurance and N 2 O
n n n Two minutes after intubation, in group I, patients received an infusion of magnesium sulphate 15 mg/kg in 30 ml 0. 9% Na. Cl for 20 min. In group II, patients received only the same amount of 0. 9% Na. Cl. Five minutes before extubation, blood samples from children were collected to assess plasma magnesium concentrations.
Extubation criteria n n n Analgesia with paracentamol administered rectally Adequate spontaneous respiratory function was reestablished (VT>5 ml/kg, respiratory rate > 12 breath/min) and complete clearance of blood and secretions. Extubation at deep plane of anaesthesia.
Results
Characteristics of Magnesium n n n 1. 2. A predominantly intracellular cation An important cofactor in many enzymatic reactions Two theory of magnesium action on CNS: CNS depressant or (Co)analgesic effect if used as a supplement to GA. - The haemodynamic and neurological changes observed after administration of magnesium suggest that it has no direct general anaesthetic properties, but causes a sleep-like state due to cerebral hypoxia from progressive respiratory and cardiac depression. - Magnesium also poorly penetrates the BBB.
n If an appropriate depth of anesthesia can be used as a precaution to prevent laryngospasm, the effects of magnesium to increase anesthetic depth may be responsible.
n 1. 2. 3. Another major effect of magnesium is muscle relaxation via three mechanisms: Calcium antagonist Partial or complete impedance of muscle endplate depolarization by decreasing Ach released from nerve ending possibly. Change membrane transport mechanism like local anesthetics
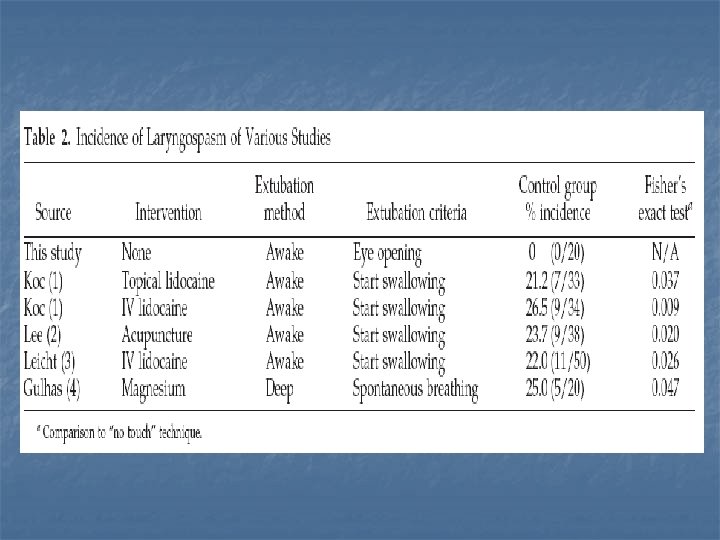
The Incidence of Laryngospasm with a “No Touch” Extubation Technique After Tonsillectomy and Adenoidectomy Ban C. H. Tsui, Wagner, Cave Anesth Analg 2004; 98: 327 -9
Background n Many of studies in these fields have focused on pharmacological or invasive interventions, such as topical lidocaine, IV lidocaine, acupuncture, or IV magnesium to prevent laryngospasm, whereas little attention has been placed on the importance of extubation technique.
No Touch technique n n n Blood and secretions are carefully suctioned from the pharynx The patient is then turned to the lateral (recovery) position with adequately anesthetized Discontinued gas while positive ventilation was continued with 100% oxygen until spontaneous ventilation returned. No further stimulation is allowed until patients spontaneously wake up. Tracheal extubation was performed when patients were able to open their eyes.
Patient data
Results n n Laryngospasm did not occur in any of our 20 study patients. Oxygen saturation levels never decreased to less than 92% and no patients experienced severe coughing.
Severity of Laryngospasm: 0= no laryngospasm; 1= stirdor on inspiration; 2=total occlusion of the vocal cords; 3= cyanosis. Severity of cough: 0= none, 1= slight, 2= moderate, 3= severe.
n If swallowing was used as a clinical indicator for extubation, the patients may have been extubated in a light plane of anesthesia because swallowing does not necessarily indicate consciousness but rather the return of laryngeal reflexes.
Brief suggestion n Perform suction thoroughly just prior volatile anesthetics was turned off. Decide whether deep or awake extubation would be suitable for the patient and perform extubation at exact timing Different invasive way to reduce the incidence of laryngospasm could be chosen based on patient’s condition.
Management of laryngospasm n n 1. 2. 3. The operational definition for laryngospasm was complete airway obstruction unrelieved by manoeuvres to relieve soft tissue obstruction, associated with Sp. O 2≦ 85%. Therapy methods were standardized according to the following protocol: Positive pressure ventilation with 100% O 2 with face mask Administration of lidocaine 1 mg/kg, Administration of succinylcholine 1 mg/kg and tracheal intubation.