Dialyzer Math The Math Terms of Hemodialysis Kuf



 is needed to ultrafilter 3 L of fluid")


")



")





 / Pre BUN")

 Better: Kt/V = -ln(R-0. 008 * t) Better")







 --------(115")
- Slides: 29
Dialyzer Math
The Math Terms of Hemodialysis Kuf Efficiency Flux Performance Ko. A Kt/V URR Recirculation
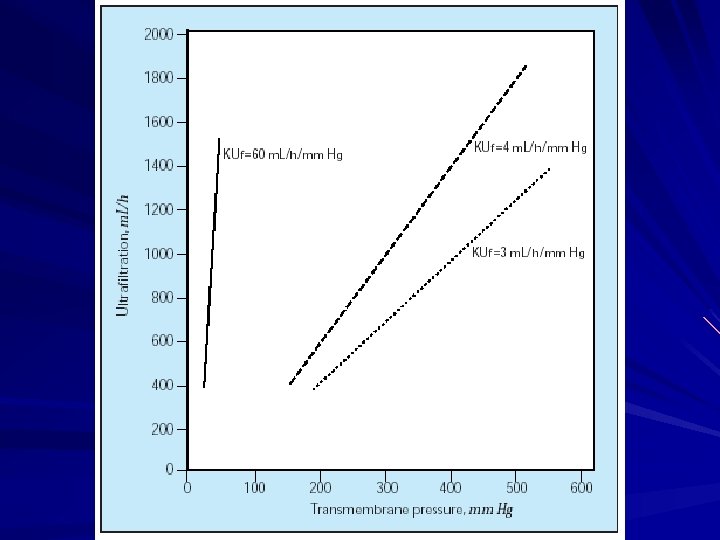
KUf Permeability of Water m. L of water per hour per mm Hg KUf = Volume/hrs / (transmembrane gradient)
KUf Questions What Transmembrane Pressure (TMP) is needed to ultrafilter 3 L of fluid over 3 hours with an F-40 filter? 50 mm. Hg What Transmembrane Pressure (TMP) is needed to ultrafilter 3. 5 L of fluid over 3 hours with an 8 L filter? 103 mm. Hg
Self-Assessment KUf Question Pre-HD weight in a patient on chronic HD is 2. 4 kg above dry weight. He is usually dialyzed for 4 hours. If the KUf of the dialyzer is 3, what is the TMP in mm. Hg required to bring his weight down to the dry weight? 100 300 200 400
Self-Assessment KUf Question Pre-HD weight in a patient on chronic HD is 2. 4 kg above dry weight. He is usually dialyzed for 4 hours. If the KUf of the dialyzer is 3, what is the TMP in mm. Hg required to bring his weight down to the dry weight? 100 300 200 400
Clearance K K = f (Ko. A, QD, QB)
Self-Assessment Question The solute transport of a dialyzer is dependent on all of the following except: l Ko. A l QB l QD l Priming volume of the dialyzer
Self-Assessment Question The solute transport of a dialyzer is dependent on all of the following except: Ko. A QB QD Priming volume of the dialyzer
Efficiency - Ko. A Dialyzer Mass Transfer Area Coefficient Ko. A = f (Ko, surface area) Ko = f (pore size, membrane thickness) m. L/min Usual efficiency: 500 -700 High efficiency: > 700
Using Ko. A Once Ko. A of a dialyzer is known, the clearance (K) of urea can be calculated given the QD and the QB Charts or Graphs available for each dialyzer
Getting the K from Graphs
Using the dialyzer with Ko. A of 400 shown below, what’s the clearance of urea at a QD of 500 m. L/min and a QB of 350 m. L/min?
So What’s Flux, Performance & Efficiency? Efficiency: Ko. A Performance: Clearance Flux: KUf
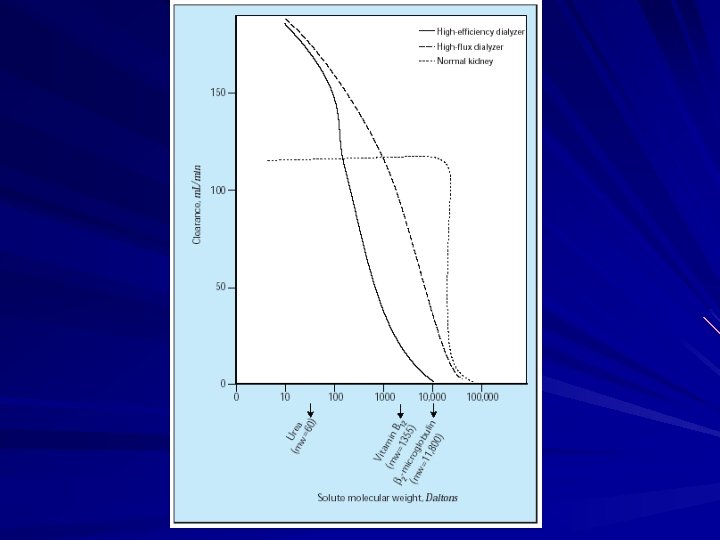
Flux Refers to size of pores High Flux is KUf > 20 m. L/hr/mm. Hg Urea Clearance – Same for high-flux vs high efficiency Beta-2 Microglobulin – More clearance with high-flux
Ways to Measure Adequacy URR Kt/V
URR The Urea Reduction Ratio (Pre BUN – Post BUN ) / Pre BUN R = 1 - URR
Simple Kt/V R = e – Kt/V R = 1 – URR
Kt/V Calculations Good: Kt/V = -ln(R) Better: Kt/V = -ln(R-0. 008 * t) Better Yet: (sp. Kt/V) Kt/V = -ln (R - 0. 008 * t) + (4 - 3. 5 * R) * UF/W Best: In-line monitoring
sp. Kt/V Formula Breakdown Urea generation during dialysis -ln (R - 0. 008 * t) + (4 - 3. 5 * R) * UF/W Raw Urea Reduction Adjustment For Volume Removed
Problem A new patient weighing 60 kg comes in with newly discovered ESRD. The BUN is 120. For the first run, you choose to drop the BUN no more than 20% using a small surface area dialyzer with K of 250 m. L/min. – A: How long should the treatment be? – B: What’s the URR?
Tougher Problem A new patient weighing 25 kg comes in with newly discovered ESRD. The BUN is 100. For the first run, you choose to drop the BUN no more than 20% using an F-40 filter at a QB of 200 m. L/min and QD of 500 m. L/min. – A: What’s the Urea Clearance (K)? – B. How long should the treatment be?
All the following are true of high/low flux hemodialyzers except: A. Conventional HD uses high-flux membranes B. High efficiency HD refers to a rapid removal of small solutes C. Low flux HD is good for urea clearance D. High flux HD uses membranes with large pore size
All the following are true of high/low flux hemodialyzers except: A. Conventional HD uses high-flux membranes B. High efficiency HD refers to a rapid removal of small solutes C. Low flux HD is good for urea clearance D. High flux HD uses membranes with large pore size
Recirculation Running the same blood through the dialyzer over and over Overestimates adequacy Easiest Measure: 3 -Sample Method – Peripheral (P) – Arterial from Dialyzer (A) – Venous from Dialyzer (V) (P-A) / (P-V) = Recirculation Accepted Recirc % is ~ 12%
Recirculation Question A 16 year old being dialyzed daily in the PICU via a Shiley in the PICU has predialysis BUN of 120 mg/d. L and post-HD BUN of 30 mg/d. L despite restriction of protein and no evidence of catabolism. You suspect recirculation. What samples do you ask to be drawn?
Recirculation Question Pre-Dialyzer BUN: Post-Dialyzer BUN: Peripheral Venous BUN: (115 – 100 ) --------(115 - 65) 15 = -----50 100 65 115 = 30 %