Diagnostic Classification Manual for InfantsToddlers DC 0 3
 Mindy")


 before")








 p p p Used")
 n Used to document")








- Slides: 24
Diagnostic Classification Manual for Infants/Toddlers DC: 0 -3, Revised (Zero to Three, 2005) Mindy Kronenberg, Ph. D. Go to http: //www. zerotothree. org/child-development/early-childhoodmental-health/diagnostic-classification-of-mental-health-anddevelopmental-disorders-of-infancy-and-early-childhood-revised. html for DC 0 -3 R forms and checklists Adapted the Colorado DC: 0 -3 To. T (2004 and 2005), in conjunction with the Irving Harris Program in Child Development and Infant Mental Health and Project BLOOM, University of Colorado Health Sciences Center. Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD 1
Purpose of the DC: 0 -3 R p To provide a developmentally sensitive diagnostic tool for diagnosing young children p To consider the impact of relationships p To complement the DSM-IV for young children – both use a multi-axial framework to allow for examination of the various areas that may influence the clinical presentation Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Diagnostic Classification Development by Zero To Three: National Center for Infants, Toddlers and Families p p p p 1987 -2003 Diagnostic Classification Task Force convened 1990 -2003 Task Force expanded 1994 Diagnostic Classification: 0 -3 published 1997 DC: 0 -3 Casebook published 2003 -2005 DC: 0 -3 R Task Force convened 2003 DC: 0 -3 Training Task Force 2005 Diagnostic Classification: 0 -3 R released Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Diagnostic Classification: 03 R p Requires multiple sessions over time (3 -5 minimum) before completing diagnosis p Assesses vulnerabilities, difficulties, strengths, and adaptations in such major development areas as: n n n p social interactions emotional regulation developmental maturation Considers the impact on the child of the family unit, the community and the culture Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Diagnostic Classification: 03 R p The goal of diagnosis is to obtain a complete understanding of the infant, in the context of his/her family p Diagnosis is an ongoing process p The diagnostic process leads to the development of a comprehensive prevention and/or treatment plan Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Diagnostic Classification Manual for Infants/Toddlers DSM-IV DC: 0 -3 R Axis I Clinical Disorders, Other conditions that may be the focus of clinical attention Primary Diagnosis Axis II Personality D/O, Mental Retardation Relationship D/O Classification Axis III General Medical Conditions Medical & Developmental D/O & conditions Axis IV Psychosocial & Environmental Problems Psychosocial Stressors Axis V Global Assessment of Functioning Functional Emotional Developmental Level 6
Axis I Diagnoses 100. Posttraumatic Stress Disorder p 150. Deprivation/Maltreatment Disorder p 200. Disorders of Affect p n n 210. Prolonged Bereavement/Grief Reaction 220. Anxiety Disorders of Infancy and Early Childhood p p p n Separation Anxiety Disorder Specific Phobia Social Anxiety Disorder (Social Phobia) Generalized Anxiety Disorder Not Otherwise Specified (NOS) 230. Depression of Infancy and Early Childhood p p n 221. 222. 223. 224. 225. 230. Major Depression 231. Depressive Disorder NOS 240. Mixed Disorder of Emotional Expressiveness Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis I Diagnoses 300. Adjustment Disorder p 400. Regulation Disorders of Sensory Processing p n 410. Hypersensitive 411. Type A: Fearful/Cautious p 412. Type B: Negative/Defiant p n n 420. Hyposensitive/Underresponsive 430. Sensory Stimulation-Seeking/Impulsive Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis I Diagnoses p 500. Sleep Behavior Disorder n n p 510. Sleep-Onset Disorder 520. Night-Waking Disorder 600. Feeding Behavior Disorder n n n 601. Feeding Disorder of State Regulation 602. Feeding Disorder of Caregiver-Infant Reciprocity 603. Infantile Anorexia 604. Sensory Food Aversions 605. Feeding Disorder Associated with Concurrent Medical Condition 606. Feeding Disorder Associated with Insults to the Gastrointestinal Tract
Axis I Diagnoses p 700. Disorders of Relating and Communicating n p 710. Multisystem Developmental Disorder (alternative for PDD-NOS for children under 2 years) 800. Other Disorders (DSM-IV-TR or ICD 10) Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Adapted from ZERO TO THREE /National Center for Infants, Toddlers, and Families. 2005. Diagnostic Classification: 0 -3 R; Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood Revised. [Wright & Northcutt (2005)]
Axis II: Relationship Classification p Assesses the parent-infant relationship and includes consideration of: n n n p Overall functional level of both the child and the parent Level of distress in both the child and the parent Adaptive flexibility of both the child and the parent Level of conflict and resolution between the child and the parent Effect of the quality of the relationship on the child’s developmental progress Two tools for evaluating relationship classification n n PIR-GAS Score Relationship Problems Check List Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis II: Relationship Classification Parent-Infant Relationship Global Assessment Scale (PIR-GAS) p p p Used to assess the quality of infant-parent relationship Typically completed after multiple clinical evaluations Relationship problems may or may not occur with symptomatic behaviors Assess the intensity, frequency, and duration of difficulties Similar to the DSM-IV-TR’s Global Assessment of Functioning scale p p p 100 -81=Adapted relationship 80 -41 = Features of a disordered relationship 40 -0 = Disordered relationship Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis II: Relationship Classification p Relationship Problems Check List (RPCL) n Used to document problems or lack of problems in a relationship, recording the extent of certain features of a parent-infant relationship (include abuse and neglect) and rates them on behavioral quality, affective tone, and psychological involvement Overinvolved Underinvolved Anxious/Tense Angry/Hostile Abusive Verbally Abusive Physically Abusive Sexually Abusive
Adapted from ZERO TO THREE /National Center for Infants, Toddlers, and Families. 2005. Diagnostic Classification: 0 -3 R; Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood Revised. [Northcutt & Wright (2005)]
Axis III Medical and Developmental Disorders and Conditions p Indicate any coexisting physical (including medical and neurological) and/or developmental diagnoses made using other diagnostic and classification systems n Many psychiatric symptoms can be caused by medical illnesses. Pediatric or other medical evaluation is highly recommended. Some examples include: Mood disorder symptoms = Endocrine disorders p Abrupt onset irritability, motor dyscoordination, restlessness = Heavy metal toxicity. p 16 Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis IV: Psychosocial Stressors p p Provides a framework for identifying and evaluating psychosocial and environmental stressors that may influence the presentation, course, treatment, and prevention of mental health symptoms and disorders in young children Recognition that the impact of stressors depends on: n n n p Severity, intensity and duration, and predictability Developmental level of child Buffering capacity of caregiving adults Includes a Psychosocial and Environmental Checklist Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis V: Emotional and Social Functioning Indicates the developmental level at which the infant organizes affective, interactive, communicative, cognitive, motor, and sensory experiences, as reflected by the infant’s functioning p Assessment is based on observations of infants interacting with parent(s) or significant caretaker p Rates the quality of the child’s play based on essential processes or capacities p Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Axis V: Emotional and Social Functioning p Capacities for Emotional and Social Functioning Rating Scale: n n n Attention and regulation (birth – 3 mos. ) Forming relationships or mutual engagement (3 – 6 mos. ) Intentional two-way communication (4 – 10 mos. ) Complex gestures and problem solving (10 – 18 mos. ) Use of symbols to express thoughts and feelings (18 – 30 mos. ) Connecting symbols logically and abstract thinking (30 – 48 mos. ) Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD
Adapted from ZERO TO THREE /National Center for Infants, Toddlers, and Families. 2005. Diagnostic Classification: 0 -3 R; Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood Revised. [Wright & Northcutt (2005)]
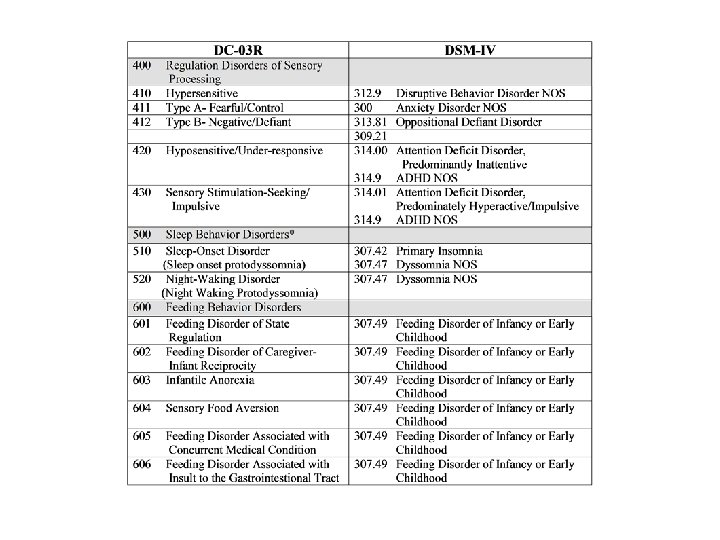
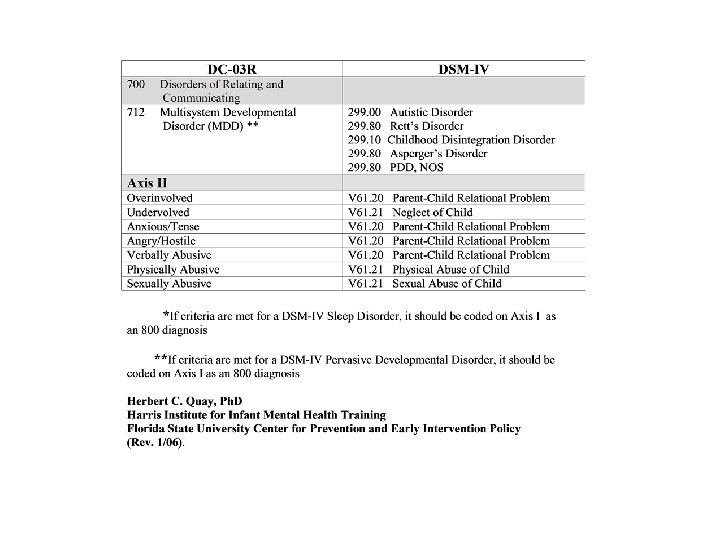
Conceptual Crosswalk Between DC-03 R and DSM IV Herbert C. Quay, Ph. D Harris Institute for Infant Mental Health Training Florida State University Center for Prevention and Early Intervention Policy (Rev. 1/06)
DC: 0 -3 R Summary p p p Developmentally informed Axis I describes clinical symptoms and disorders found in young children Axis II highlights relational concerns Axis III provides a place for medical and/or developmental diagnoses derived using other systems Axis IV examines the impact of psychosocial stressors Axis V looks at the child’s emotional and social functioning Copyright 2006, the FSU CPEIP and Robert J. Harmon, MD