DIAGNOSIS OF TUBERCULOSIS Dr Manie van Rensburg DIAGNOSIS

DIAGNOSIS OF TUBERCULOSIS Dr Manie van Rensburg
")
DIAGNOSIS OF TUBERCULOSIS • • SPECIMENS MICROSCOPY CULTURE IDENTIFICATION SENSITIVITY TESTING DNA DETECTION (PCR) BIOCHEMICAL MARKERS IMMUNOLOGICAL

SPECIMENS • GO WHERE THE GOLD IS • Nonspecific disease - Which specimen ? • QUALITY OF SPECIMEN • Result as good as the specimen received • Sputum / Spit • Pleural biopsy / Pleural fluid • NUMBER OF SPECIMENS • Sputum 2 -3 early morning specimens • Urine – 3 full bladder morning specimens

MICROSCOPY • • DIRECT / CONCENTRATED SPECIMEN ACID-FAST STAIN ZIEHL- NEELSEN OR FLUOROCHROME DETECTION ABILITY • • ZN stain 10 000 organisms/ml for smear positivity Fluorochrome stain – easier to detect organisms Gram stain – Gram positive or ghost organisms Sensitivity 22 -80 %

Ziehl-Neelsen stain

Fluorochrome stain
![CULTURE • LIQUIFIED / [ ] / DECONTAMINATED • DECONTAMINATION • Kills normal flora](http://slidetodoc.com/presentation_image_h/dec0e9d63f79505e9a219722f7a71231/image-7.jpg "CULTURE • LIQUIFIED / [ ] / DECONTAMINATED • DECONTAMINATION • Kills normal flora")
CULTURE • LIQUIFIED / [ ] / DECONTAMINATED • DECONTAMINATION • Kills normal flora and TB bacilli • SOLID MEDIA / LIQUID MEDIA • Solid media - Egg based (LJ) / Agar based (MB) • Liquid media – Middel brook • TEMPERATURE OF INCUBATION • Lower temp – M. marinum, M. ulcerans, M. chelonae, M fort • AUTOMATED SYSTEMS • Continious monitoring of growth (6 w)

Culture media

Culture media

CULTURE • Remains the most sensitive test • Insufficient decontamination • Many contaminated specimens • Target level 5 -10 % • Over decontamination • No contaminated specimens • Decreased mycobacterial yield

IDENTIFICATION • BIOCHEMICAL • Not done – takes weeks to months to do • TB protein detection • Secrete more than 33 proteins • Predominamt protein – MPT 64 – rapid immunochromographic detection test • HPLC • Mycolic acids in the cell wall • PROBES (PCR) • DNA probes Commercial / In house • M tuberculosis and Non tuberculous mycobacteria

AMPATH statistics • 16 % of Specimens are culture positive • 12 % M. tuberculosis (75%) • 1. 5% M. avium – intracellulare (10%) • 2. 5% Other NTM (15%) • 40 -50% Culture pos is ZN positive • 2 -3% Contamination rate

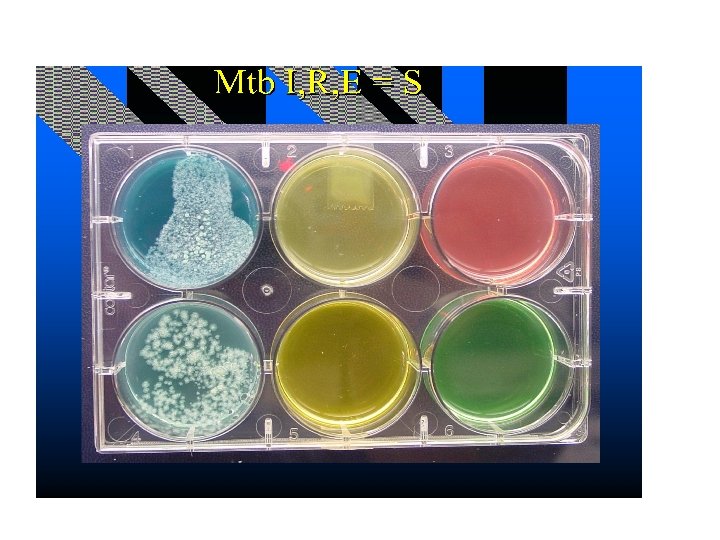
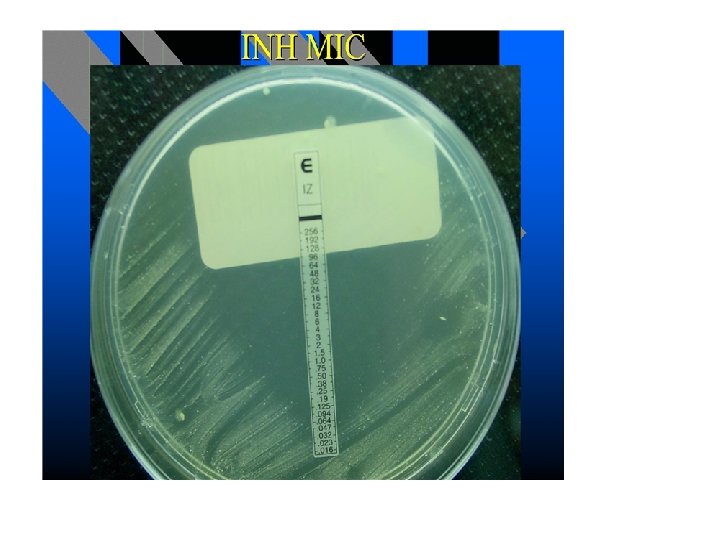
SENSITIVITY TESTING • Breakpoint method – Agar dilution – Not done – Broth dilution – Automated method • MIC’S – E test • GENETIC BASIS (PCR) – Line probe assay

Representative DNA patterns obtained by the MTBDRplus assay. A. Lacoma et al. J. Clin. Microbiol. 2008; 46: 3660 -3667
")
DNA DETECTION • • • DNA is very stable in the environment (lab contam) Is present in dead bacilli Cannot be used to monitor treatment Extraction method of DNA very NB NB Quality of the specimen Our laboratory 3 TB DNA tests are done – Hain test – Gene. Xpert

Hain Test • Developed to do sensitivity testing on smear positive samples – 70% (1= 40%) sensitivity Smear negative samples • Confirms presence of M. tuberculosis • Sensitivity for INH and Rifampicin • Second line sensitivity testing

Gene. Xpert • Presence of MTB and sensitivity to Rif – ZN neg specimens – sens 75% • • • False rifamicin resistance (few) – major implications POC testing Hardware expensive Reagents expensive Wastage Robust system

Laboratory flow diagram • Decontamination / ZN / Culture • ZN pos – For molecular ID and Sens • ZN neg – Culture

Biochemical markers • ADA • Urinary Lam test

Biochemical markers • ADA – Presently total ADA is determined – Adenosine ---ADA ---> Inosine – Total ADA increased in TB, bacterial inf, RA, lymphoproliferative disorders, empyema – Iso enzymes • ADA 1 in all cells • ADA 2 in stimulated monocytes and macrophages – ADA 2 elevated in TB and RA

Biochemical markers • Urine Lam test – Cell wall component – lipoarabinomanan – Excreted in urine (lateral flow test) – Used in HIV infected individuals with low CD 4 count < 100 cells/ul (WHO 2015) – Sensitivity 28% - 65% – Specificity 90% - 97% – Prognosticator – 2 x greater mortality test pos
 – Nearly 100 years old –")
Immunological • Mantoux skin test (Tuberculous skin testing) – Nearly 100 years old – Diagnosis latent infection – PPD standarised (RT-23) – PPD 5 TU injected intradermally (Wheal) – False negative • Technical, advanced TB, malnutrition, elderly, HIV – False positive • BCG (1 yr 40% 10 yr 20%), NTM,
 tests – TB spot test or TB gold")
Immunological Interferon gamma release assay (IGRAS) tests – TB spot test or TB gold test – Lymphocytes stimulated (ESAT 6, CFP 10, TB 7. 7)– interferon production pos test – We prefer the TB spot test (less intermediate results) – Not distinguish between active and latent infection – Increased specificity (BCG/NTM not false pos) – Improved sensitivity – TB children with HIV – One patient visit

Pearls • • Go where the gold is Result is as good as the specimen received Culture remains gold standard PCR quicker result – less sensitive

Questions • Can you do a TB pcr test on blood in a patient with pulmonary TB? • Can you do TB pcr on a post treatment patient? • Does a negative TB microscopy, culture or TB pcr test exclude TB? • Why do you send 3 specimens for TB?

REFERENCES • Principles and practices of infectious diseases Mandell, Bennett, Dolin • Manuel of Clinical Microbiology Murry, Baron et. Al • Rapid Molecular Detection of Tuberculosis and Rifampin resistance Boeheme et al. N Eng J Med 361; 11 1005 -1015 • Molecular Diagnosis of Mycobacteria Clinical Chemistry 47: 5 809 -814
- Slides: 28