Diagnosis of abuser By Prof Dr Sherif Mohamed


Diagnosis of abuser By Prof. Dr: Sherif Mohamed Hassan El-Qannishy Associate Consultant & Professor of Analytical Toxicology and Biochemistry Emergency Hospital - Analytical Toxicology Unit Forensic Medicine & Clinical Toxicology Department Faculty of Medicine - Mansoura University

TOXICOLOGY

TOXICOLOGY n Greek words toxicos and logos is the study of the adverse effects of chemicals on living organisms. n It is the branch of medical science, which deals with poisons with special reference to their source, character, properties, symptoms they produce, and of remedial measures.

Substances that cause disturbances to organisms n All substances are poisons, there is none which is not a poison. n PARACELSUS (1493 -1541 ) n

Narcotics n n From ancient Greek "to make numb“ Any psychoactive compound with any sleep-inducing properties.
 Abuse n Use of drugs without any medical prescription.")
1) Abuse n Use of drugs without any medical prescription.
 Dependence Continue to take a drug n In order to avoid discomfort of")
2) Dependence Continue to take a drug n In order to avoid discomfort of its absence ( withdrawal symptoms ) n

Dependence Psychic dependence Physical dependence • It is the desire for • It is an altered physiological continuous intake of the state in which the person is drug to experience a in a compulsory need of a psychological effect. drug • Withdrawal symptoms are mild or slight. sever. • Slight psychic dependence known as habituation
Tolerance • Tendency to increase the dose of the drug.")
3)Tolerance • Tendency to increase the dose of the drug.

What is addiction? n Addiction = Abuse + Dependence + Tolerance n If the Addict attempts to stop drug abuse, a lot of dangerous physical and psychological symptoms will instantly appear "withdrawal symptoms". withdrawal symptoms

Substance Morphine Barbiturates Alcohol Benzodiazepines Alcohol Cocaine Cannabis Physical dependence Psychic dependence Severe Present Severe, occurs rapidly Very severe, occurs slowly With prolonged heavy use Present Slight Tolerance Marked Less marked Present With prolonged use Present Slight & to some actions only questionable (? ) Slight

Reasons for Addiction : Lack of awareness regarding dangers of drug abuse. Poor religious. Broken homes. Bad companionship. Unemployment. n n n

Signs of Addiction A Anger Absence F friends Fat

L Lifestyle Lonely M Mood Money

Dreams of addiction Reality of addiction
 1970 regulates the manufacture")
Drug Abuse Prevention and Control Act Controlled Substances Act (CSA) 1970 regulates the manufacture , distribution, and dispensation of drugs with a potential for abuse. n The CSA classifies drugs with the potential for abuse into five schedules (I–V) to indicate their level of control n n Drugs in Schedule I have the highest potential for abuse and addiction. n Drugs in Schedule V have the least potential for abuse and addiction.

Schedul Abuse e Potential Prescription Requirement Examples I high; no accepted Medical use no prescription permitted heroin, LSD (lysergic acid diethylamide), marijuana, tramadol II high; accepted medical use Prescription required; no refills permitted without a new written prescription codeine, morphine, and opium III moderate; accepted medical use Prescription required; 5 refills permitted in 6 months certain barbiturates IV low; accepted medical use prescription required; 5 refills permitted in 6 months barbital, V low; accepted medical use no prescription required for individuals 18 or older unless quantities are greater than 4 fluid ounces. cough syrups with codeine, atropine sulfate

TOXICOLOGICAL SAMPLES
 n Hair n saliva")
TOXICOLOGICAL SAMPLES Urine n Blood serum n Vomits (food poisoning) n Hair n saliva n

A comparison of the types of samples that can be used in drugs of abuse testing Sample Advantages Disadvantages Urine -Non-invasive -Available in large volumes -Remains positive 2– 3 days -High adulteration potential when collection not witnessed Blood -Difficult to adulterate -Short half-life of drugs -Low drug concentrations -Potential for long-term assessment of drug use -Requires difficult analytical Requires difficult analytical procedures (expensive) Hair Saliva -Difficult to adulterate -Low drug concentrations -Difficult to get large volumes for confirmation
 The person. 2) The drug.")
ACTIVE PRINCIPLES of Drugs It depends on: 1) The person. 2) The drug.
 Urine Blood Hair Alcohol")
Duration of active principles in urine: Name Detect (Days ) Urine Blood Hair Alcohol 3 -12 (12 h) (1 y) Hashish 5 -30 (sometimes 11 w) (sometimes 11 w 1 -6 2 90 (6 h) 90 Opium / Tramadol

Adulteration of urine sample Can I beat a drug test and pass? The best way to pass the drug testing is not to do drugs at all
 loading up on water before a urine drug test")
Methods of Samples Adulteration 1) loading up on water before a urine drug test : 1) loading up on water urine look pale. specific gravity <1010. (Normal: specific gravity 1010 : 1025) 2) Acids (lemon juice, Hydrochloric and nitric acid): 2) Acids p. H <7. (normal urine p. H = 5 : 8 ) 3) Bleach (liquid chlorine): 3) Bleach characteristic odour

What is the most common method of Adulteration ? ? ?
 screening tests 2) confirmation tests. n")
Drug Testing: Divided into two major categories: 1) screening tests 2) confirmation tests. n
 n Rf = Y/X (always ≤")
THIN LAYER CHROMATOGRAPHY TLC n Retardation factors (Rf) n Rf = Y/X (always ≤ 1)

Immunoassay Rapid test detection n Antigen antibody reaction = Urine sample interact with labeled antibody dye.

Immunoassay n Automated drug detection
 n All positive results on immunoassay are must")
Confirmatory test Gas chromatography-mass spectrometry (GC-MS) n All positive results on immunoassay are must be confirmed using GC-MS. n

Test Cut off Amphetamine 1000 ng/ml Barbiturates 100 ng/ml Benzodiazepines 1000 ng/ml Cocaine 300 ng/ml Opiates 300 ng/ml Cannabinoids (THC) 50 ng/ml Tramadol 200 ng/ml

Drugs of TOXICOLOGICAL important
DAT : 1) Ethanol 2) Cannabis 3) Opiates 4) Barbiturates")
Drugs of important : A)DAT : 1) Ethanol 2) Cannabis 3) Opiates 4) Barbiturates 5) Amphetamines 6) Benzodiazepines 7) Tramadol B)TDM : 1) Digoxin 2) Carbamazepines 3) Valproic acid 4) Phenytoin 5) Phenobarbital

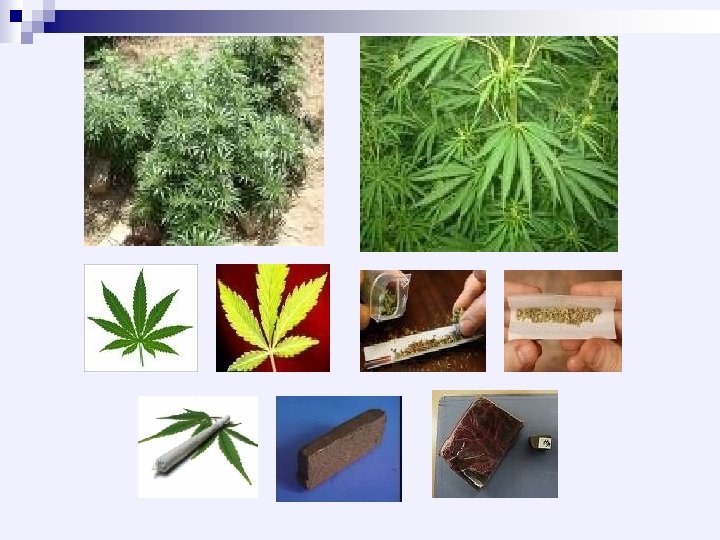
Cannabis
Cannabis : ◙ Other names: 1) In east Africa Hashish & Bango 2) In")
A-2)Cannabis : ◙ Other names: 1) In east Africa Hashish & Bango 2) In America Marijuana ( a Mexican term means pleasurable feeling ) 3) In western Africa Kaif ◙ Active principle : ∆-9 -THC (∆-9 -Tetrahydrocannabinol ) ◙ Important notes : - All parts of the plant are poisonous except the coarse stocks. - THC is fat soluble , which is rapidly cleared from plasma after consumption and stored in body fatty tissues.
Small dose: - Sense of well being Hallucination Euphoria")
☼ Clinical picture of cannabis: 1)Small dose: - Sense of well being Hallucination Euphoria Laughing Joking cheerfulness 2)Moderate dose: - Disorientation of place Disorientation of time Dilated pupil 4 D Red eyes Death Fear 3)Large dose: - Deep coma - Death (Respiratory Failure. )

Short-term effects of cannabis Dry mouth "cotton mouth" n Muscle relaxation n Increased heart rate n
. n Testicular cancer increased risk of 70%")
Long-term effects Mental problems (schizophrenia and depression). n Testicular cancer increased risk of 70% n Increased risk of infertility. n

Faces of Cannabis Effects begin within few minutes, peak 30 mins. last 2 hours 25 -30% remains in the body

Investigations for Cannabis : ►Qualitative test: - For urine sample. ► False positive results with 1) Anti-tussive drug (Marinol) 2) Anti-inflammatory/ Anti-rheumatic (Nuprin, Motrin/Aleve) 3) anti-histaminic (Phenergan, Promethegan) 4) Analgesic (Orudis KT) 5) Vitamin B , Riboflavin (B 2, Hempseed Oil) 6) Chemotherapy (Nabilone)

Very important Strict Observation during sampling

Lastly Longer decision times Leading to slower responses to situations

Impact of cannabis on fertility: Reduces sperm production. n Reduces sperm motility. n Incrases number of abnormal sperm. n Increases DNA damage (Induce premature labour) n Plasma of smokers have significant - lower total testosterone level - higher FSH and LH concentrations. n

Normal Semen Analysis

CASA


Opiates
Opiates : ■ source: Papapaver somniferum plant")
A-3)Opiates : ■ source: Papapaver somniferum plant
")
Opiates includes : Codeine n Morphine n Heroine ( cause Perforated nasal septum ) n
 Stimulation stage : n n Sense of well being")
Cl. P of opium: 1) Stimulation stage : n n Sense of well being Euphoria Hallucination laughing 2) Depression stage : n n n Unpleasant sensation Sleepiness Fixed PPP

Investigations for Opium : ► Qualitative test: - For urine sample. - False positive results with 1) Pain prescriptions for 1) 2) Cough suppressants (containing codeine) 2)


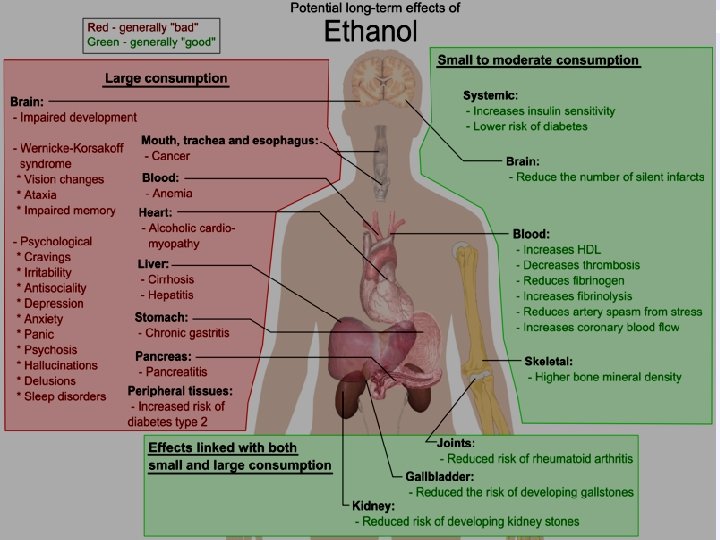
Ethanol
Ethanol : C/P: Depends on ethanol bl. Level : - 1)Asymptomatic: <0. 05 gm%")
A-1)Ethanol : C/P: Depends on ethanol bl. Level : - 1)Asymptomatic: <0. 05 gm% 2)Mild toxicity: 0. 05 -0. 15 gm% Drowsiness 0. 05 -0. 15 gm% Euphoria Behavioral changes (Real man appear) Aggressiveness 3)Moderate toxicity: 0. 15 -0. 25 gm% Flushing ( Alcohol flush) Hiccough Ataxia Emesis Eye manif. ( blurring of vision ) Ms. Manif. (staggering gait / tremors)
Severe toxicity : 0. 25 -0. 35 gm% Alcohol coma 5)Death : >0. 35")
4)Severe toxicity : 0. 25 -0. 35 gm% Alcohol coma 5)Death : >0. 35 gm% Due to (Resp. Failure in early death ) (Liver cell failure & fatty liver in late death) In mild and moderate intoxication hypoglycemia is commonly present.
Qualitative test: - For urine sample 2)Quantitative test: - For")
Investigations for Ethanol : 1)Qualitative test: - For urine sample 2)Quantitative test: - For blood sample - Enzymatic method (Alcohol DH)

#- False positive results : n n with other volatile reducing agents with ( such as : methanol = found in cheap beverages ) "fermented or decomposed" foods: - fermentation is the conversion of a carbohydrate such as sugar into an acid or an alcohol ( ethanol ). - More specifically, fermentation can refer to the use of bacteria to create lactic acid in certain foods. - Many fermented foods, such as soy sauce, contain a significant amount of alcohol.

Results of food fermentation Ethanol n Vinegar, in the form of acetic acid n Ammonia n Lactic acid n Carbonic acid n
 is which can cause blindness , due")
Methanol n Minimal toxic dose (60 ml) is which can cause blindness , due to its metabolization to formaldehyde blindness formaldehyde & formic acid leading to systemic acidosis (serum p. H drops below 7. 2) N. B: Blindness is not at once. (Normal serum p. H =7, 35 -7. 45). n Formic acid in the urine reduces Fehling's solution , so gives false positive result of diabetes.

Amphetam ine

Amphetamine uses: 1. It is used by students : To keep them wakeful and alert during exam. , This may lead to physical dependence on the drug. 2. It is used therapeutically as: a- Nasal inhalation for decongestion b- For treatment of obesity
. n Dextroamphetamine sulphate injection (Dexedrine) (Maxiton forte). n")
Amphetamine preparations Amphetamine sulphate (Benzedrine). n Dextroamphetamine sulphate injection (Dexedrine) (Maxiton forte). n

☼ C/P of Amphetamine: THE PRIDE-C

Talkativeness T Tachycardia Tachypnea Hypertension H Hyperthermian Halluciations E Euphoria

P R I Palpitations Rigidity Insomnia Dilated pupil D Death (Renal Failure / Respiratory Failure) C Convulsions Coma

Investigations for Amphetamine : Qualitative test: - For urine sample. #- False positive results : Amantadine/Chlorpromazine/Phentermine/ Ranitidine/Thioridazine/Trazodone n

BARBITURATES
.")
Therapeutic uses: Hypnotics n General anaesthesia n n Psycho-analysis (Truth serum).

Classification: They are classified according to the duration of action into: n n Long acting: (6 -8 hours): e. g. phenobarbital "luminal", "veronal". Intermediate acting: (4 -6 hours) e. g. Amobarbital "Amytal". Short acting: (about 3 hours): e. g. Secobarbital Na "Seconal" Ultra-short acting: (15 minutes or more) e. g. thiopental Na "Pentothal".
. n Respiration:")
n CNS: CNS depression (ranging from mild sedation and hypnosis to coma). n Respiration: Respiratory depression. n Cardiovascular system: direct myocardial depression effect causing decreased force of contraction with reduced cardiac output. So, a fall in the blood pressure.

n GIT: decrease motility, tone and secretion. n Kidney: oliguria or even anuria due to hypotension. n Uterus: Hypnotic doses don't impair the uterine contraction during labour. Full anaesthetic doses decrease the force and the frequency of uterine contraction during labour and may inhibit the foetal respiration after delivery.

Investigations for BARBITURATES Qualitative test: - For urine sample. #- False positive results : Ibuprofen /Naproxen

Benzodiazepines

Benzo. Therapeutic uses: Anticonvulsant n Treatment of anxiety states. n Market names: Rivotril /Apetryl/ Parkinol. n

B Bullous skin lesions. E Intellectual impairment N Nausea / Vomiting / Vertigo Z Headache O Coma D Diplopia / Drowsiness / Dysarthria

Investigations for Benzo Qualitative test: - For urine sample. #- False positive results : n Oxaprozin n Sertraline

Captagon

Captagon, the trademark name for the synthetic fenethylline. stimulant n Was first produced in the 1960 s to treat depression. n

Captagon Fenethylline = amphetamine + theophylline Captagon CNS Irritability/ Cardiac Heart rate Paranoia Diarheaa

Cocaine

Mode of consumption of Cocaine n Chewing the leaves of coca. n I. V. injection of the drug. Snuffing of its powder which may be adulterated with irritating substances as boric acid (thus, nasal septum perforation). n

Cocaine abuser n Tactile hallucination, the addict feels as if insects were creeping under his skin "cocaine bugs or formication". n Dangerous Euphoria may be unlike the calm morphine abuse. n n n Tremors and pain in the muscles and joints. Anorexia, loss of appetite and wasting. Perforated nasal septum.

► Qualitative test: - For urine sample. ► False positive results with n Amoxicillin n Tonic water

EYE SIGNS

Dilated pupil Red eyes Fixed PPP Blurring of vision Cannabis opium Ethanol Mydriasis Amphetamine Diplopia Benzodiazepines

TDM

Digoxin
Digoxin (lanoxin): A therapeutic drug used for cardiac patients with CHF or supraventricular tachycardia.")
B-1)Digoxin (lanoxin): A therapeutic drug used for cardiac patients with CHF or supraventricular tachycardia. n It has a cumultive effect & narrow therapeutic/toxic ratio. n Therapeutic Dose : 0. 25 mg. daily (1 x 1) n Fatal dose : 2 -4 mg. n Fatal period : 30 min. - 24 h. n

Cl. P of digoxin toxicity: GIT symptoms: Nausea / Vomiting Abdominal pain Diarrhea Cardiac symp. : Bradycardia (pulse may fall to 20/min. ) Visual symp. : Color vision (yellow &or white vision ) Blurring of vision & diplopia CNS symp. : Headache CNS symp. : Confusion

Investigations for Digoxin : n Serum blood level (Normal 0. 8 - 2. 1 ng/ml) When to take blood Pre-dose preferably Or at least 6 hours after oral dose to allow distribution n How often to repeat 1 week after initiation or dose change n

Digoxin Half-life 30 -40 hours Time to steady state sampling >1 week Loading dose IV 10 microgram/kg in 100 m. L saline over 2 hr oral 15 microgram/kg (750 -1, 500 micrograms in divided doses) Maintenance dose 62. 5 micrograms – 250 micrograms once daily When to take blood Pre-dose preferably (at least 6 hours after oral dose to allow distribution) How often to repeat 1 week after initiation or dose change Sampling method Li-heparin/SST Signs of toxicity Anorexia, nausea, vomiting, various arrhythmias, atrial tachycardia, 10 -15 mg fatal in adults, Target range 1 -2 microgram/L Practical issues 125 mcg tablet 100 mcg liquid (2 m. L) 80 mcg iv

Carbamazepine
 Carbamazepine: n n n Anticonvulsant & antiepileptic Seizures. Mania, mental illnesses & depression.")
B-2) Carbamazepine: n n n Anticonvulsant & antiepileptic Seizures. Mania, mental illnesses & depression. It works by reducing abnormal electrical activity in It works by reducing abnormal electrical activity the brain. Trade names: Tegretol.

What are the hazards during using Carbamazepin ? ? ? n Life-threatening allergic reactions. These risks are highest in Asian people who have a genetic (inherited) risk factor. Anaphylactic shock. n Decreases the number of blood cells (WBCs & n platelets).

Carbamazepine toxicity: n n n Dry mouth.
 n False")
Investigations for Carbamazepine : Serum blood level (Normal 4 - 12 ng/ml) n False positive results with TCA. n When to take blood Pre-dose n How often to repeat After dose changes (5 -7 days) n

Carbamazapine Half-life 30 hr then 15 hr due to autoinduction Time to steady state sampling 5 -7 days after dose change Loading dose Slow titration: 100 -200 mg bd oral > increasing by 100 -200 mg each week Maintenance dose 200 -800 mg bd When to take blood Pre-dose How often to repeat After dose changes (5 -7 days) Sampling method Heparin Target range 4 -12 mg/L

Valproic Acid
Valproic Acid : Anticonvulsants drug. n Seizures. n Mania. n n Trade names: Depakene")
B-3)Valproic Acid : Anticonvulsants drug. n Seizures. n Mania. n n Trade names: Depakene :

Valproic acid IMPORTANT WARNING: Irregular heart beat. Difficulty breathing & swallowing Blurred or double vision. Thinking about killing himself or planning or trying to do so. Sleepiness / Coma V
 If")
Investigations for Valproic Acid : n Serum blood level (Normal: 50 -100 mg/ml) If you have diabetes Valproic acid can cause false results on urine tests for ketones (DKA? )


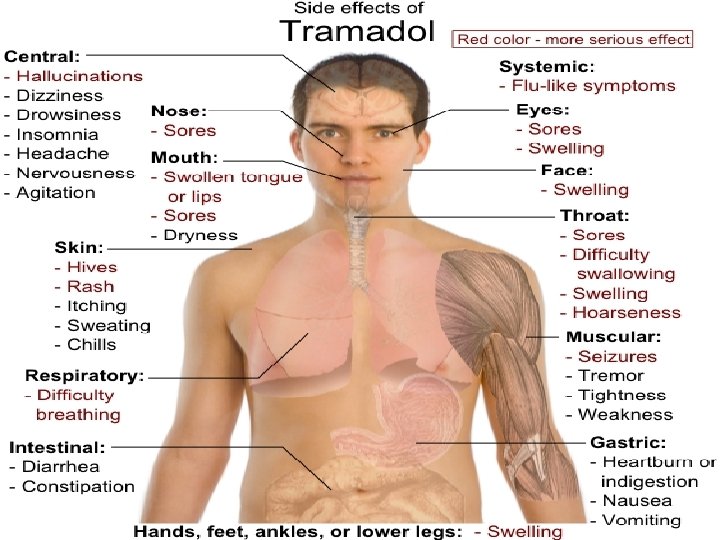
What is tramadol? A popular painkiller medication. n A 4 - phenyl-piperidine analogue of codeine synthetic agents. n Centrally acting synthetic opioid analgesic n It helps to get rid of the pain, by blocking transmission of pain information for brain receptors. n

Different brands of the drug on the market Tamol, Ultram, Ultracet, Ryzolt, Tramal, and Tramacet. n Tramadol is excreted in breast milk. n

Therapeutic dosage 50– 100 mg every 4– 6 h. n The total daily dose should not exceed 400 mg with adult. n A peak blood concentration within 2 hrs. n

n Once a prolonged use of the drug , it is usually result in dependence, and resistance to drugs. dependence

Tramadol has been shown to cross the placenta. n Tramadol has been shown to cross BBB. n Tramadol has a cumulative excretion in breast milk within 16 hours postdose n

Tramadol abuse Swelling n Sweating n Tremors n

Phenytoin

Phenytoin Half-life 22 hours but caution: saturable metabolism Time to steady state sampling Varies considerably between patients (1 -5 weeks) Loading dose 18 mg/kg slow iv infusion for status epilepticus over 30 -60 mins (ECG recommended) Maintenance dose 100 mg 6 -8 hourly iv (convert to od if stable) 200 -500 mg once daily po When to take blood Pre-dose How often to repeat Sample within 2 -3 days of initiation Then again 3 -5 days later. If no change, monitor weekly. Sampling method Li-heparin/SST Signs of toxicity nystagmus, diplopia, ataxia, confusion, slurred speech, hyperglycaemia, respiratory/circulatory depression (2 -5 g lethal) Target range 10 -20 mg/L

Lithium

Lithium Half-life 24 hours Time to steady state sampling 4 -5 days after starting or change in therapy or sodium/fluid intake Loading dose 400 mg-1. 2 g daily Maintenance dose 400 mg – 1, 200 mg od po When to take blood pre-dose How often to repeat Weekly until dose stable then at least 3 -monthly Sampling method Plain tube Signs of toxicity Hyperreflexia & hyperextension of limbs, convulsions, psychoses, syncope, renal failure, circulatory failure, coma, death Target range 0. 4 – 1. 0 mmol/L Practical issues Slow release brands not interchangeable

Theophylline

Theophylline /Aminophylline iv Half-life 8 hours Time to steady state sampling 2 hours post load, then 12 hours into infusion Oral: 5 days after starting Loading dose 5 mg/kg iv if treatment naïve in 100 m. L over 20 mins Maintenance dose Infusion 0. 5 mg/kg/hour (500 mg in 500 m. L) Oral: 200 -500 mg 12 -hourly (slow release) When to take blood Infusion : 24 hours after dose Oral : pre-dose & at least 4 -6 hours post-dose How often to repeat As required Sampling method Li-heparin/SST Signs of toxicity Nausea, vomiting and haematemesis, agitation, restlessness, dilated pupils and convulsions, hypotension and life-threatening cardiac arrhythmias Target range 10 -20 mg/L Practical issues Slow release brands not interchangeable Theophylline 790 mg = Aminophylline 1, 000 mg

How to write an analytical toxicology report ? ? ?

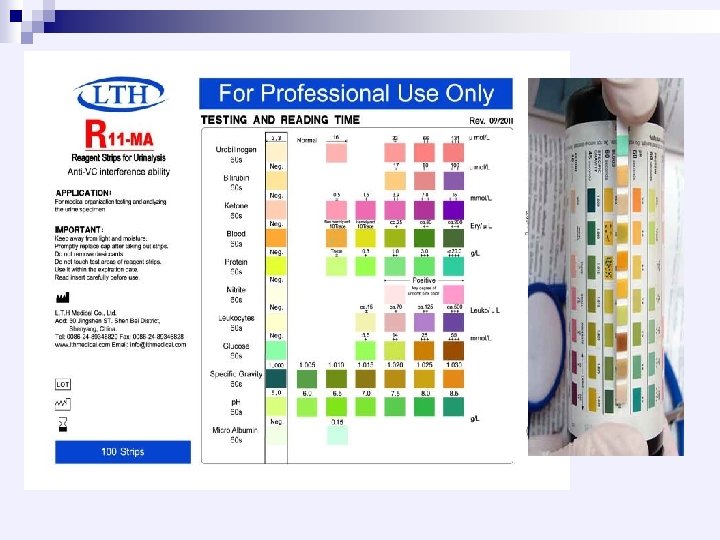
/ ﺩ 0 ﺃ Referred by Prof. Dr. / ﺍﻟﺴﻴﺪ ﻋﻦ ﺍﻟﻤﻘﺪﻡ ﺍﻟﺘﺤﻠﻴﻞ ﻧﺘﻴﺠﺔ ﺍﻟﻤﻘﺪﻡ 2010 / / / ـــــــﺎﺭﻳــــﺦ / ﺍﻟﺴﻦ / ﺍﺧﺬﻫﺎ ﺍﻟﺴﺎﺑﻖ ﺍﻷﺪﻭﻳﻪ ANALYTICAL Site of Sample collection: Urine Sp. Gr. : Urine p. H : Urine Nitrite : TOXICOLOGY ………. . . Thanks for reference REPORT Inside/Outside Lab. ( N. : 1005 -1025 ) ( N. : 5 – 8 ) ( N. : negative ) Signature ►These results are preliminary results & must be confirmed by HPLC or GS/MS


Thank You
- Slides: 126