Diagnosis and tt planning in FDPII Dr Jitendra


























- Slides: 28
Diagnosis and tt planning in FDP-II Dr Jitendra Rao Dept of Prosthodontics
Indication for FDP/FPD • • • Mutilated crown or tooth Missing tooth Endodontically tt teeth Discolored teeth Fractured tooth Spacing
Contraindication • • High caries index High DMF index Unfavorable abutments Age below 18 yr of age Medically compromised patients Neurological patients Xerostomic patients Patients with radiotherapy and chemotherapy
Articulators: Articulators vary widely in the accuracy with which they reproduce the movements of the mandible. Non-adjustable articulator: device/instrument that is capable of only a hinge opening Semi-adjustable articulator: • Allows a close approximation of anatomic distance between the axis of rotation and the teeth • casts are mounted using facebow pproximate transverse horizontal axis, the radius of movement produced on the articulator will reproduce the arc of closure with relative accuracy and any resulting error will be slight • Inter condylar distances are adjustable to small, medium and large configurations
• This type of articulator can be used for the fabrication of most single units and fixed partial denture • Use face bow-arbitrary • Arcon articulators e. g. Whip mix– used more for fixed restoration • Non arcon e. g Hanau series- used for complete denture Fully adjustable articulator: • designed to reproduce the entire character of border movements, including immediate and progressive lateral translation, and the curvature and direction on condylar inclination • Inter condylar distance is completely adjustable • Face bow -kinematic
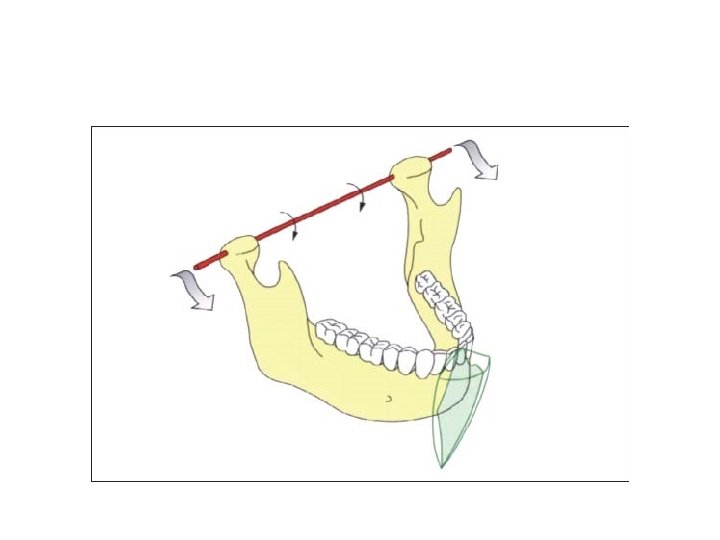
Locating the transverse hinge axis • axis of rotation that is as close as possible to the transverse horizontal axis of the patient’s mandible • The most accurate way to determine the hinge axis is by the “trial and error” method developed by Mc. Collum and Stuart in 1921 (using a kinematic face bow). • Arbitrary face bows can also use but they must have an acceptable accuracy. • Caliper style ear piece face bows possess a relatively high degree of accuracy with 75% of the axes located by it falling within 6 mm of the true hinge axis
Single tooth restoration • INTRA CORONAL RESTORATIONS - depended on the strength of the remaining tooth structure for structural integrity e. g inlay, onlay • EXTRA CORONAL RESTORATIONS If insufficient tooth structure exists to retain the restoration within the crown of the tooth, an extracoronal restoration, or crown is needed. – Partial veneer crown – Full metal crown
TREATMENT PLANNING FOR REPLACEMENT OF MISSING TEETH Important ones are ØBiomechanical factors ØPeriodontal factors ØEsthetics ØFinancial factors ØPatient’s wishes
Abutment Evaluation § Abutment is a tooth, portion of tooth or portion of a dental implant that supports or retain a prosthesis § Abutment teeth are called upon to withstand the forces normally directed to the missing teeth, in addition to those usually applied to the abutments • Whenever possible an abutment should be a vital tooth. However, a tooth that has been endodontically treated which is asymptomatic with radiographic evidence of a good seal and complete obturation of the canal can be used as an abutment. If the endodontically treated tooth does not have sound tooth
• The roots and their supporting tissues should be evaluated for 3 factors: • Crown-root ratio • Root configuration • Periodontal ligament area
Ideal crown-root ratio for a tooth to be utilized as a fixed partial denture abutment
Studies by Klaffenbach in 1936 have shown that occlusal forces exerted against prosthetic appliances have been shown to be considerably less than that against natural teeth (about 160 lb) FPD against RPD 26. 0 lb FPD against FPD 54. 4 lb FPD against natural teeth 150. 0 lb
Root configuration-
Periodontal ligament area. Johnston et al in 1971 in their statement designated as “Ante’s law” said that the root surface area of the abutment teeth had to equal or surpass that of the teeth being replaced with pontics
Jepsen in 1963 has reported areas of the root surfaces of the various teeth which is also termed as Jepsen’s rule Root Surface Area (mm) Teeth Maxillary Mandibular Central Incisor 204 154 Lateral 179 168 Canine 273 268 First PM 234 180 Second PM 220 207 First Molar 433 431 Second Molar 431 426
Biomechanical Considerations • All fixed partial dentures, long or short spanned bend and flex under masticatory load • Bending or deflection varies directly with the cube of the length and inversely with the cube of occlusogingival thickness of the pontic • ( D α L 3 ) where D is defelection, L is length of the pontic span on given occlusogingival height • Compared with a fixed partial denture having a single tooth pontic span, a two tooth pontic span will bend 8 times as much • Double abutments are sometimes used as a means of overcoming problems created by unfavourable crown-root ratios and long span. There are several criteria that must be met, if a secondary abutment is to strengthen the fixed partial denture
SPECIAL PROBLEMS Pier abutments: § An edentulous space can occur on both sides of a tooth, creating a lone, free standing pier abutment § Physiologic tooth movement, arch position of the abutments and a disparity in the retentive capacity of the retainers can make a rigid 5 -unit fixed partial denture as a less than ideal plan of treatment § Forces are transmitted to the terminal retainers as a result of the middle abutment acting as a fulcrum, causing failure of the weaker retainer
Pier abutment
• The use of a non-rigid connector has been recommended to reduce this hazard • The most commonly used non-rigid design is a T shaped key that is attached to the pontic and a dove tail key way placed within a retainer • The key way of the connector should be placed within the normal distal contours of the pier abutment and the key should be placed on the mesial side of the distal pontic • Non rigid connector transfer shear stress to bone rather than connector as well as minimize mesiodistal torqueing of abutment
Tilted Molar Abutments • When the teeth are mesially tilted beyond an optimal degree of tilt deleterious forces act over the abutment causing vertical bone loss around the mesial portion of teeth thus further compromising periodontal support and weakening of the abutment • If these teeth are used as abutment for fixed partial dentures it will lead to failure of prosthesis • The over-all objective in molar uprighting is ideal positioning of the molar which will eventually become an abutment tooth for a fixed prosthesis. The ideal position will provide an optimal periodontal environment for the molar
§ A proximal half crown can be used as a retainer on the distal abutment. This preparation design is a 3 ¼ crown that has been rotated 90°. It can be used only if the distal surface is untouched by caries § A telescoping crown and coping can also be used as a retainer for the tilted molar. A full crown preparation with heavy reduction is made to follow the long axis of the tilted molar. An inner coping is made to fit the tooth preparation. The proximal half crown that will serve as the retainer for the FPD is fitted over the coping § A non-rigid connector is another solution to the problem. A full crown preparation is done on the tilted molar, with its path of insertion parallel with the long axis. A box form is placed on the distal surface of the premolar to accommodate a keyway in the distal of the premolar crown
Cantilever FPDs • A cantilever FPD is one that has an abutment or abutments at one end only, with the other end of the pontic remaining unattached. This is a potentially destructive design with the lever arm created by the pontic • Abutment teeth for cantilever FPDs should be evaluated for lengthy roots with a favorable configuration, good crown root ratios and long clinical crowns.
Canine Replacement FPD/ Canine Rule • This is a problem because often the canine lies outside the interabutment axis • The abutments are the lateral incisor, usually the weakest in the entire arch and the first premolar, the weakest posterior tooth • A FPD replacing maxillary canine is subjected to more stress than that replacing a mandibular canine, since forces are transmitted outward on the maxillary arch. So the support from secondary abutments will have to be considered.
Books • Rosensteil • Shillingburg