DIAGNOSIS AND TREATMENT OPTIONS IN HEAD AND NECK









, Maxillary sinus (15%) 35% had CNS extension from sinus/orbit")





























- Slides: 43
DIAGNOSIS AND TREATMENT OPTIONS IN HEAD AND NECK NEOPLASMS EVAN S. BATES, M. D. DEPT. OF OTOLARYNGOLOGY
NASAL/SINUS TUMORS Overall incidence: 1: 100, 000 80% SCCA, 10% ACC/AC Risk factors: environmental exposure Diagnosis CT/MRI, biopsy Treatment Surgical resection Chemotx/XRT
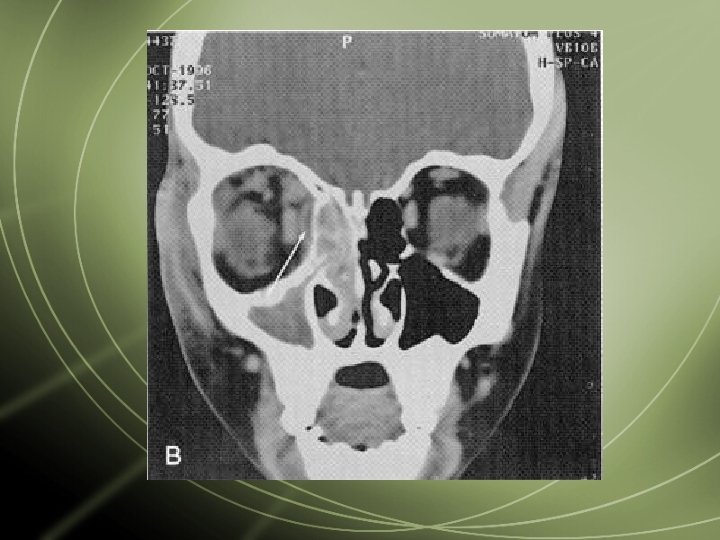
CASE PRESENTATION This 37 yo male presented with a 4 -5 week H/O an enlarging left neck mass. 3 months earlier he noted episodes of left nasal congestion with eye discomfort. PMH: ASD repair 3/96 H/O smoking 1 ppd/15 yr. , quit 5 yr. go Exam: nasal: polypoid mucosa left inf. turbinate oropharynx: nl. neck: 6 x 5 cm firm, mid. Cervical mass
EVALUATION FNAB: + for malignant cells immunostain profile suggests medullary CA MRI: large left neck mass, adenopathy in levels 2 -4, small left intraparotid masses. Thyroid nl. CXR: nl. Laboratory: calcitonin 2, CEA <0. 7, TSH, LFT’s nl.
DIFFERENTIAL DIAGNOSIS Lymphoma Primary salivary neoplasm mucoepidermoid CA, squamous CA, adeno. CA Thyroid neoplasm anaplastic CA, medullary CA Sinus neoplasm squamous CA, adeno. CA Unknown Head & Neck Primary
SURGICAL MANAGEMENT Left radical neck dissection Left total parotidectomy
SURGICAL FINDINGS Normal thyroid gland Multiple parotid cysts Large left neck mass w/ additional adenopathy Frozen section c/w malignant neoplasm Permanent section c/w rhabdomyosarcoma, alveolar type
SURGICAL MANAGEMENT Left endoscopic turbinectomy, resection of nasal mass findings large polypoid mass on posterior inf. Turbinate with extension superiorly along lateral nasal wall to middle meatus path rhabdomyosarcoma
RHABDOMYOSARCOMA: MD ANDERSON EXPERIENCE 5 yr. Survival 44%, 60% w/combined TX. Poor survival adult onset of disease alveolar histology-distant mets Symptoms: nasal obstruction (60%), facial pain (41%), facial swelling (38%), proptosis (35%), epistaxis (27%)
RHABDOMYOSARCOMA: UCLA EXPERIENCE Orbit (35%), Maxillary sinus (15%) 35% had CNS extension from sinus/orbit Histology not a factor in prognosis Overall survival 34% Trend toward conventional surgery followed by intensive chemo/XRT
RHABDOMYOSARCOMA Most common head&neck tumor in children, rare in adults 69% advanced @ presentation (Group III, IV) Ethmoid sinus most common site (46%) Nodal mets (46%), systemic mets(26%) Management: chemo/XRT/surgery 7. 6% 5 yr. survival
NOSE EXAMINATION
Usually seen in chronic sinusitis or chronic allergy patients Topical corticosteroids of minimal benefit Polyps require sugical excision and biopsy followed by long term allergy management NASAL POLYPS
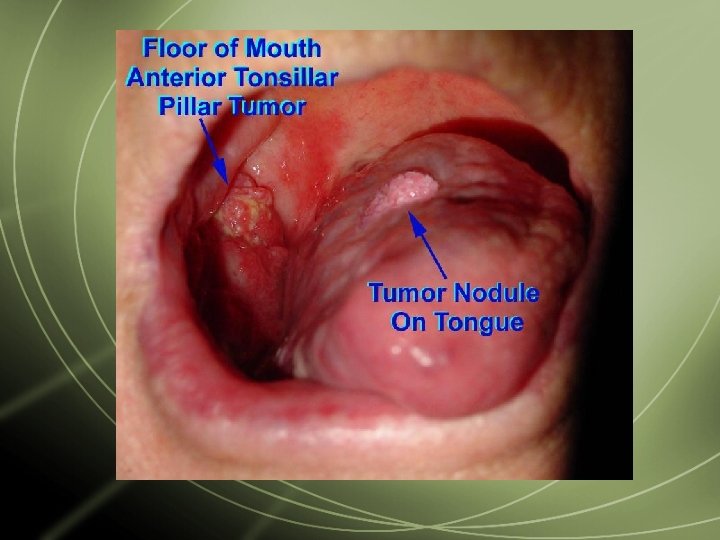
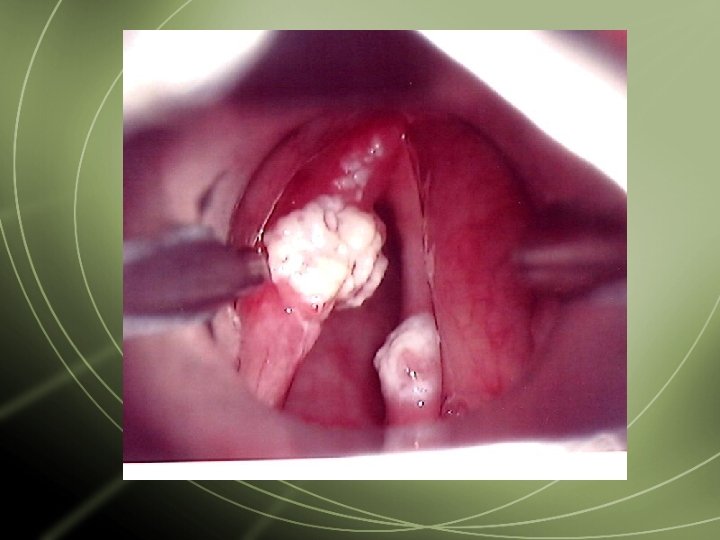
OROPHARYNGEAL CARCINOMA Usually presents with painful oral ulcer Adult males 50 -70 yrs. old Risk factors: smoking, ETOH Majority of tumors SCCA, lymphoma Management: Surgery/XRT XRT/CHemotx
TONSILLAR CARCINOMA 20 -30% present with neck metastases Evaluation with CT/MRI, Chest CT, PET scan, LFT’s Management must include neck disease Stage I survival 80 -90%, Stage IV survival 2540% Treatment standard involves surgery/XRT
TONGUE NEOPLASMS 3% of all CA in US, 50% of CA in India, 3 rd most common malignancy in France >90% SCCA, associated with tobacco use, ETOH Survival rate decreased with lymphatic involvement Treatment focused on surgery/XRT Reconstruction of prime importance
TONGUE CARCINOMA Tongue lesions can be resected primarily due to tongue redundancy Primary closure vs. local flap XRT for incomplete resection, T 2 or greater lesions or nodal disease
TONGUE MASS Neurofibroma Mucosal covered mass rather than ulcerated lesion Surgical resection alone is sufficient
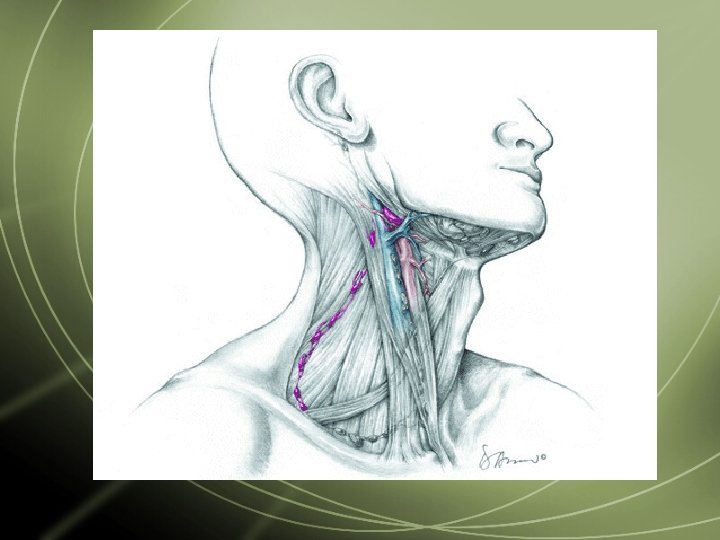
NECK EXAMINATION
NECK MASSES KEY TO DIAGNOSIS IS HISTORY TIME COURSE OF MASS PAINFUL/TENDER RECENT INFECTIONS/TRAUMA SMOKER? PHYSICAL EXAM LOCATION OF MASS FIRM/CYSTIC/TENDER/MULTI PLE MASSES
NECK MASSES IF YOU SUSPECT INFECTION, TREAT WITH 1 COURSE OF ANTIBIOTICS IF NO RESOLUTION, REFER TO ENT EVALUATION HEAD & NECK EXAM FNA-B CT/MRI
NECK EXAMINATION
THYROID MASS Large thyroid mass suspicious for malignancy FNA-B important Surgical resection with CN X monitor Post-operative therapy dependent on path
LIP CARCINOMA Uncommon site for oral carcinoma Usually managed with wide local excision Frequently seen in pipe smokers
HOARSENESS MANAGEMENT: REFER TO ENT IF PROLONGED OR DIAGNOSIS UNCERTAIN INDIRECT LARYNGOSCOPY BE SUSPICIOUS OF MALIGNANCY IN SMOKERS AT ANY AGE
LARYNGEAL CARCINOMA Usually seen in smokers Extremely hoarse voice for several weeks May have referred otalgia Obviously needs laryngoscopy/biopsy
LARYNGEAL CARCINOMA Treatment goals shifted to larynx preservation based on 1992 VA study 11, 000 new cases annually, >90% have smoking exposure Induction chemotx/XRT preserves larynx in 64% patients XRT for T 1/T 2 lesions 5 yr. Survival 70 -80% for T 3< lesions, 40% for T 4 lesions
LARYNX EVALUATION
VOCAL CORD NODULE Usually a gravelly/hoarse voice History of voice overuse/singers Voice rest may help Often associated with GERD ENT eval. for laryngoscopy
HOARSENESS ASSOCIATED WITH URI SELF-LIMITED RESOLVES IN 7 -21 DAYS PROLONGED RESOLUTION IN SMOKERS MANAGEMENT ANTIBIOTICS (S. AUREUS) HUMIDIFICATION STEROIDS
HOARSENESS CHRONIC HOARSENESS VOCAL OVERUSE VOCAL FOLD POLYPS GERD PRESBYLARYNGIS ACUTE HOARSENESS IF ASSOCIATED WITH NECK TRAUMA--ER