Diagnosis and Therapy in Benign Paroxysmal Positional Vertigo
 Dr. Nadir Ali Syed Head,")
Diagnosis and Therapy in Benign Paroxysmal Positional Vertigo (BPPV) Dr. Nadir Ali Syed Head, Section of Neurology Aga Khan University

• • Introduction to BPPV Pathophysiology of most BPPV History and physical exam Canalith repositioning therapy

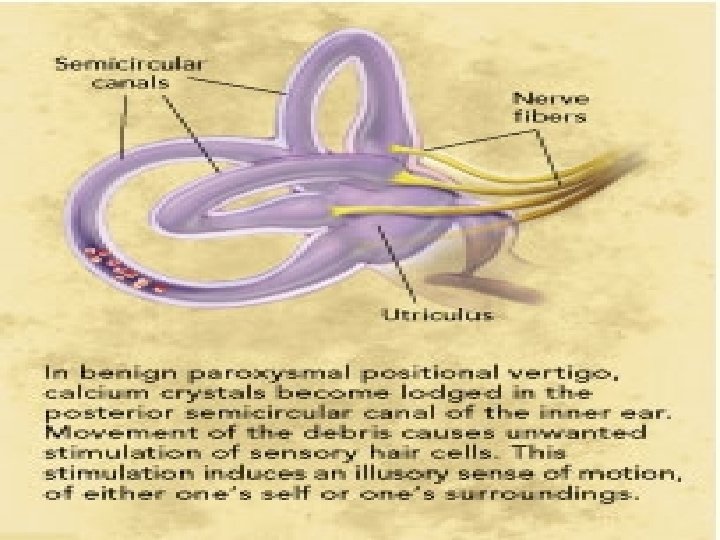
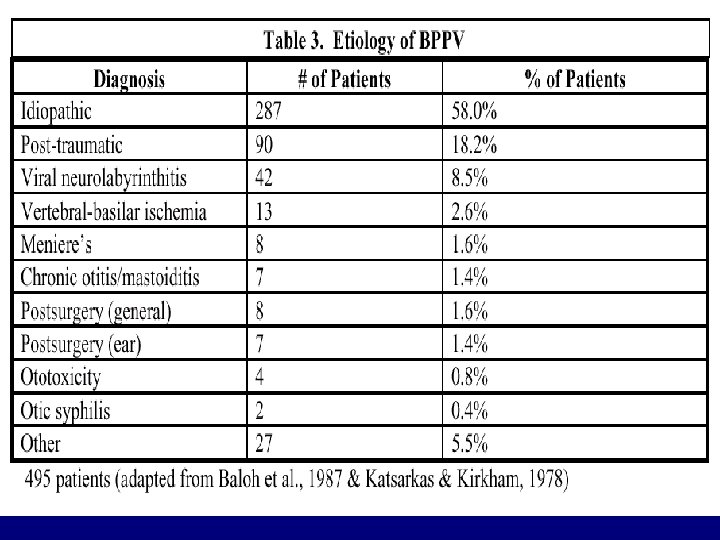
Introduction: • BPPV is a peripheral vestibular disorder • causes spells of vertigo that last less than 1 minute when the patient moves their head. • 1 in 4 people will suffer it at some time during their lifetime • It is now a readily treatable condition

• • Introduction to BPPV Pathophysiology of most BPPV History and physical exam Canalith repositioning therapy

• • Introduction to BPPV Pathophysiology of most BPPV History and physical exam Canalith repositioning therapy

History • Patients complain of vertigo that usually goes away in a few seconds to a minute if they do not move their head again. • often occurs in the morning when they get up or turn over in bed • poor balance may last for several hours after a bout of positional vertigo.

Frequency of complaints in patient with BPPV from standardized questionnaire Poor balance Sense of rotation Trouble walking Lightheadedness Nausea Sense of tilt Sweating Sense of floating Blurred vision 57% 53% 48% 42% 35% 24% 22% 15%

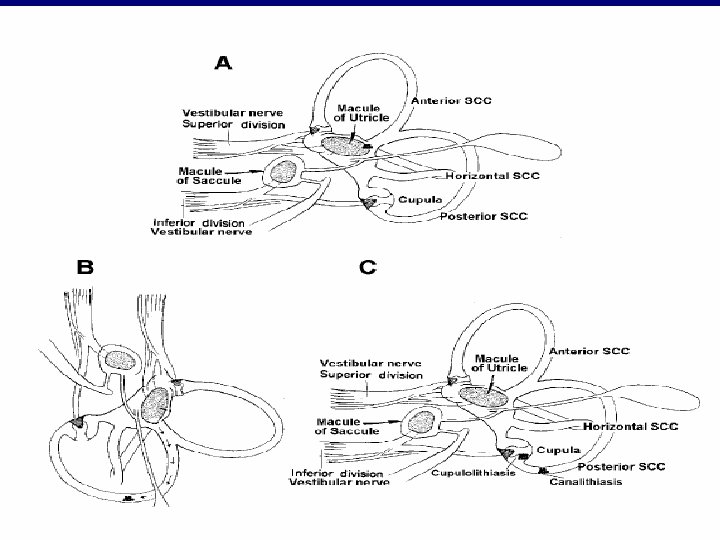
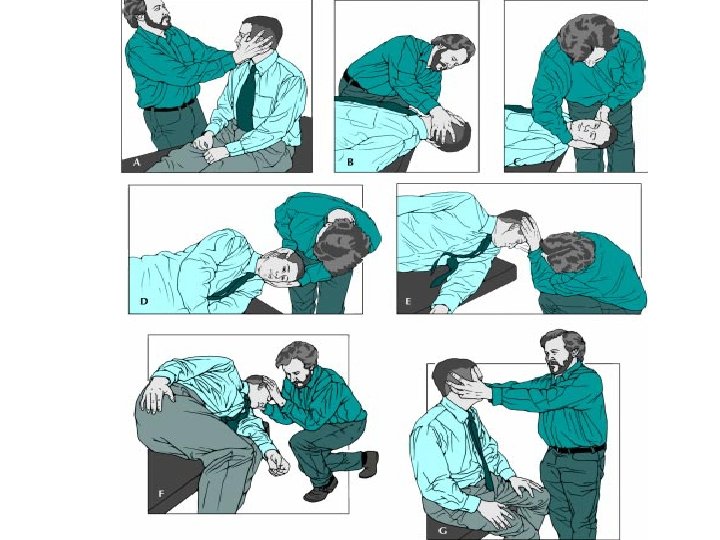
Physical Exam Diagnosis of BPPV is secured by eliciting nystagmus and vertigo after the head is moved in the plane of one of the SCC Bedside tests to diagnose BPPV: Dix-Hallpike Test

• • Introduction to BPPV Pathophysiology of most BPPV History and physical exam Canalith repositioning therapy
 for posterior SCC BPPV It is effective in 85 -95%")
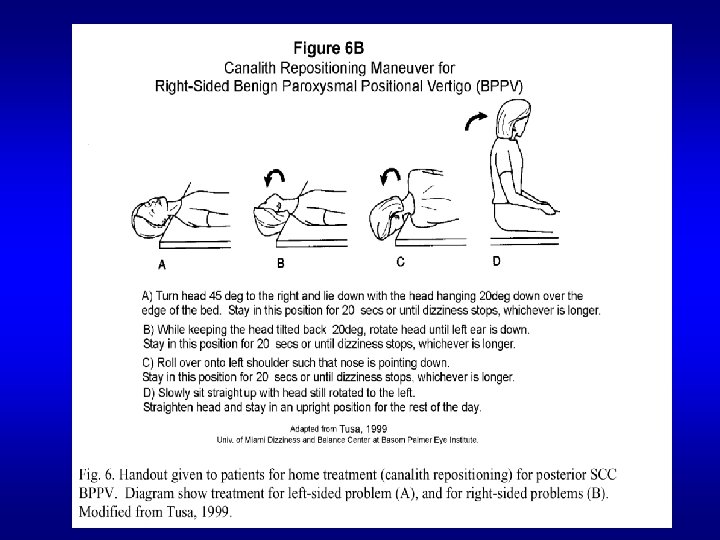
Canalith Repositioning Therapy (CRT) for posterior SCC BPPV It is effective in 85 -95% of patients with one treatment Epley, 1992, 1996, Herdman et al, 1993, Weider et al, 1994, Welling et al, 1994, Fung et al, 1996,

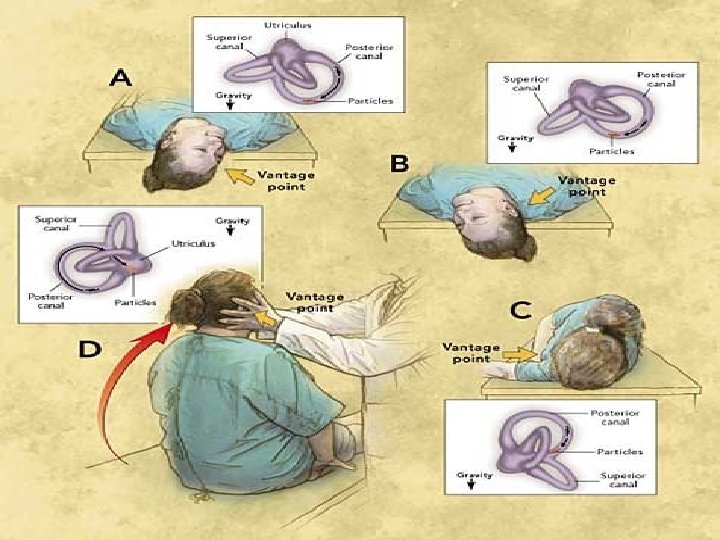
Treatment of posterior SCC BPPV • Therapy is based on treatments that move the otoconia in the SCC back to the utricle. • Once it is in this location it is reabsorbed into the macule of the utricle. • Medication is not indicated, as this is a mechanical problem. • there is no treatment that can prevent the recurrence of the

Summary Posterior and anterior semicircular canal BPPV comprises majority of BPPV, and may be treated effectively by CRT. THE END Acknowledgments: David Solomon, Ronald J. Tusa Michael C. Schubert, Terry D. Fife American Academy of Neurology Massachusetts Medical Society
- Slides: 19