Diagnosis and management of arrhythmogenic right ventricular dysplasia
")


 is an inherited disease, typically inherited as an autosomal")



 the")

 in right precordial leads.")






 is an excellent tool for visualising the")





 is used in cases of drug refractory/intolerance or incessant")





- Slides: 36
Diagnosis and management of arrhythmogenic right ventricular dysplasia (ARVD)
DEFINITION ARVD is a disease of the heart muscle associated with ventricular arrhythmias and sudden death. It is characterised by structural and functional abnormalities of the right ventricle caused by the replacement of the myocardium by fatty and fibrous tissue.
The sites of involvement of anatomic abnormalities are found in the so-called triangle of dysplasia 1. the right ventricular subtricuspid areas 2. the apex 3. the infundibulum
Arrythmogenic right ventricular dysplasia (ARVD) is an inherited disease, typically inherited as an autosomal dominant trait with variable penetrance and incomplete expression. There is an autosomal recessive variant associated with palmoplantar keratosis and wally hair named Naxos disease
Prevalence The prevalence in the general population is approximately from 1: 2500 to 1: 5000 Nevertheless, it is dependent on geographic circumstances, for example in certain regions of Italy (Padua, Venice) and Greece (island of Naxos), the prevalence is increased. It accounts for 5% to 10% of unexplained sudden cardiac deaths in individuals under 65 years. It occurs in young adults with a male to female ratio of 2, 7/1. After hypertrophic heart disease, it is the number one cause of sudden cardiac death in young people.
Diagnosis of ARVD is often difficult because there is no single test. Diagnosis is based on the presence of structural, histological, electrocardiographic and genetic factors.
Clinical history First of all, we’ll start with the easier tool, that is, clinical history. Clinical presentation varies from asymptomatic forms to palpitations, fatigue, syncope or even cardiac arrest usually during exercise. These symptoms are due to ventricular ectopic beats, sustained ventricular tachycardia of left bundle branch block configuration or right ventricular failure.
We can identify four stages in the natural history of this disease a) the early or silent phase, it is a subclinical phase with concealed structural abnormalities b) the unstable phase with electrical disorder c) the right ventricular failure phase d) the final phase with progressive biventricular failure, mimicking dilated cardiomyopathy
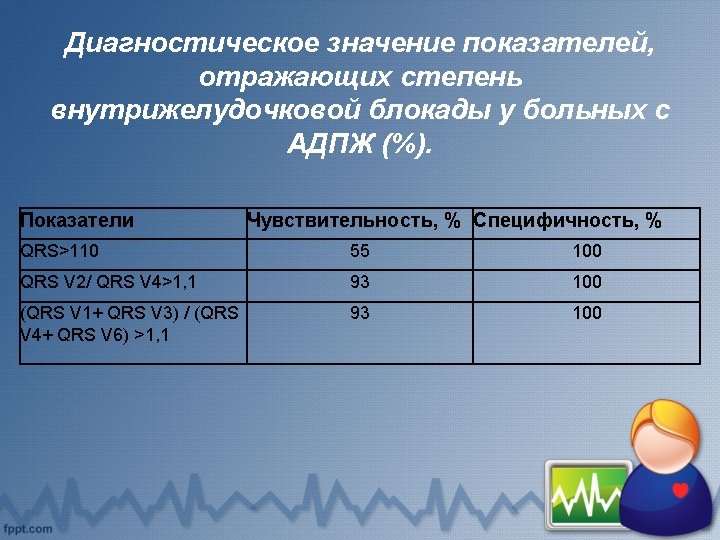
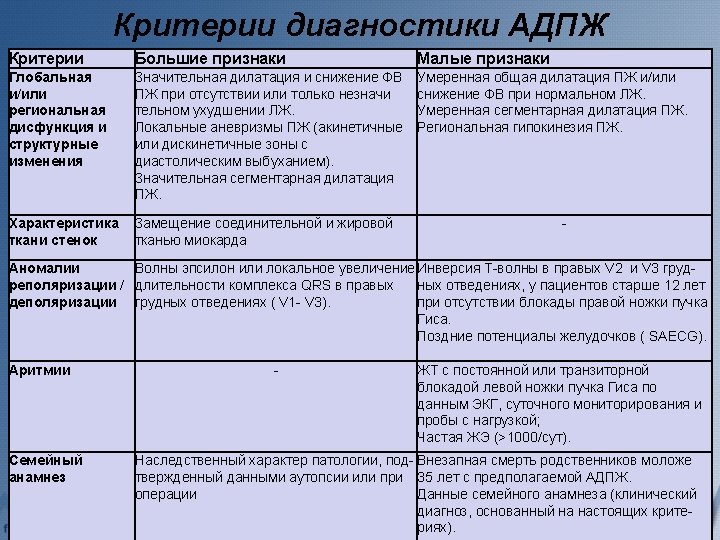
Diagnostic tests • There are several ECG features in the criteria diagnosis of ARVD: a) T wave inversions in V 1 through V 3 (minor diagnostic criterion, but one of most common ECG abnormality present in 85% of patients b) QRS duration = 110 ms in V 1 through V 3 c) Epsilon wave (electric potentials after the end of the QRS complex). It is a major diagnostic criterion found in up to 30% of cases of ARVD.
Recording a post-excitation epsilon wave (arrows) in right precordial leads.
12 lead ECG recording of VT with left bundle branch block morphology
• Other ECG markers of ARVD have been reported: QRS and QT dispersion, parietal block defined as a QRS duration in leads V 1 through V 3 that exceeds the QRS duration in lead V 6 by > 25 ms, a prolonged S-wave upstroke in V 1 through V 3 = 55 ms (it was seen as the most prevalent ECG feature in 95% of ARVD
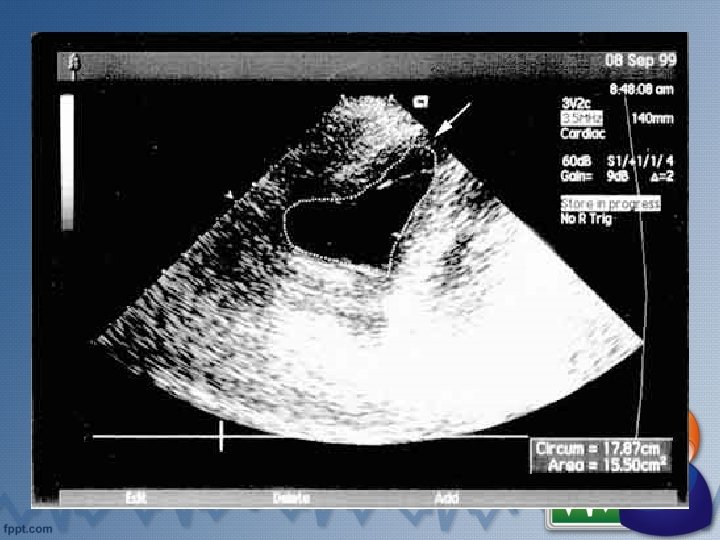
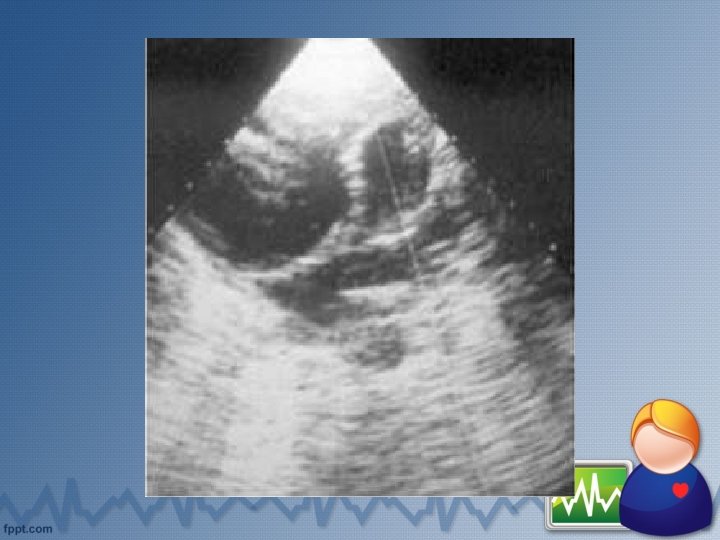
Echocardiography is the initial diagnostic approach in patients suspected of having ARVD. Principal findings are: - right ventricular dilation and hypokinesia - isolated dilatation of the right ventricular outflow tract - increased reflectivity of the moderator band - end-diastolic aneurysms - akinesis-dyskinesis of the inferobasal segment and the right ventricular apex - prominent apical trabeculae
Computed tomography Findings of ARVD on electron-beam computed tomography are: - the presence of epicardial fat or intramyocardial fat deposits - conspicuous trabeculations with low attenuation - dilated hypokinetic right ventricle - scalloped appearance of the right ventricular wall
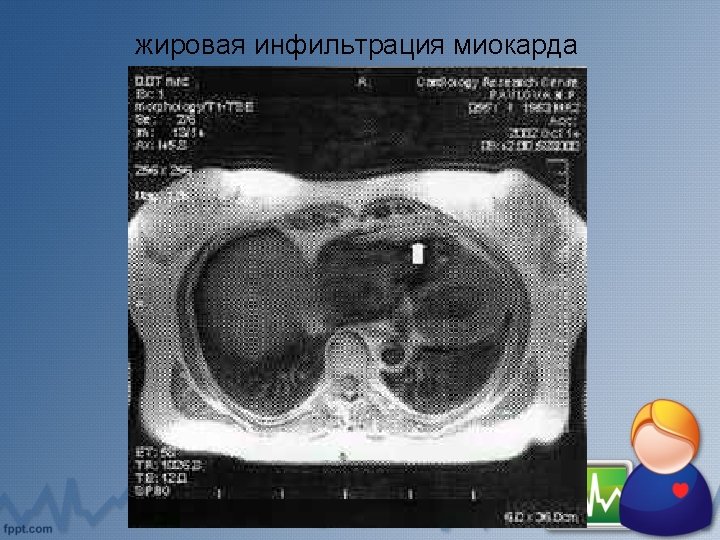
Cardiovascular magnetic resonance imaging Magnetic resonance (MR) is an excellent tool for visualising the right ventricle, it allows a threedimensional evaluation of ventricular anatomy, volumes and when compared against other techniques it can better recognise the replacement of myocardial fatty and fibrofatty tissue, although fatty infiltration of the right ventricle is not exclusive of ARVD, as it occurs in more than 50% of normal hearts in elderly people. However the presence of transmural fatty replacement or diffuse thinning of the right ventricle myocardium should be considered to be a major criterion for the diagnosis of ARVD
The typical criteria that can be demonstrated with MR are: v presence of high-signal intensity areas indicating the substitution of myocardium by fat (major criterion) v fibrofatty replacement which leads to diffuse thinning of the right ventricular myocardium (major criterion) v aneurysm of the right ventricle and right ventricular outflow tract (major criterion) v dilatation of the right ventricle and right ventricular outflow tract (when severe, major criterion; when mild, minor criterion) v regional contraction abnormalities (minor criterion) v global systolic dysfunction (major criterion) and global diastolic dysfunction (minor criterion)
Endomyocardial biopsy Histological diagnosis is definitive, however endomyocardial biopsy is controversial because of the segmental nature of the disease and the samples are usually obtained from the septum. Complications can occur such as tamponade and perforation
Management of patients with ARVD Before treatment, we have to know predictors of mortality and risk stratification. The study of Hulot et al found that at least 1 episode of left bundle-branch block ventricular tachycardia, clinical signs of right ventricular failure and left ventricular dysfunction were associated with cardiovascular deaths. The problem is that the appearance of sudden death is not related to disease progression and sudden death could be the first manifestation of the disease.
Catheter ablation Radiofrequency ablation (RF) is used in cases of drug refractory/intolerance or incessant ventricular tachycardia. The goal of RF ablation is to eliminate conduction pathways. It is associated with complete success in only 30 to 65% of cases. Due to the progressive and diffuse nature of the disease, it is difficult to abolish multiple arrhythmogenic foci.
Implantable cardioverter-defibrillator Patients considered at high risk for sudden cardiac death should receive an implantable cardioverter-defibrillator (ICD). They are those who: 1) have been resuscitated from cardiac arrest with a history of syncope, 2) have threatening arrhythmias that are not completely suppressed by antiarrhythmic drug therapy and 3) with a family history of cardiac arrest in first degree relatives (primary prevention).
ICDs work by providing antitachycardia pacing and defibrillation shocks when arrhythmias occur. ICD therapy is feasible and safe in patients with ARVD with a low incidence of short term and long term complications. This tool has an important role in the treatment of ventricular arrhythmias, more than three quarters of ARVD patients received appropriate ICD therapy during an average of 3, 5 years of follow up
Cardiac failure treatment When right ventricular or biventricular failure appear, treatment consists of the current therapy for heart failure including diuretics, beta blocking agents, angiotensin-converting enzyme inhibitors and anticoagulants. Curative therapy in case of refractory congestive heart failure and/or arrhythmias is cardiac transplantation.
Take care your heart!
Использованная литература • Diagnosis and management of arrhythmogenic right ventricular dysplasia (An article from the E-Journal of the ESC Council for Cardiology Practice) Authors: Pérez Díez D. , Brugada J. • АРИТМОГЕННАЯ ДИСПЛАЗИЯ/КАРДИОМИОПАТИЯ ПРАВОГО ЖЕЛУДОЧКА Седов В. М. , Яшин С. М. , Шубик Ю. В. • Arrhythmogenic right ventricular cardiomyopathy Author: Pennell D. J. • Подготовил: Магистрант 1 курса Фатхуллаев З. Х.